Article Text

Abstract
Objective To demonstrate the spectrum of autoimmune retinopathy (AIR) associated with immunotherapy for advanced cutaneous melanoma.
Methods and analysis Retrospective chart review on patients with advanced cutaneous melanoma who developed AIR after initiating immunotherapy. Complete ophthalmic examination and relevant ancillary testing were performed on each patient. The presence of AIR-associated anti-retinal antibodies was confirmed by western blot and/or immunohistochemical staining. Ophthalmic and systemic outcomes after treatment for AIR were followed over time. A systematic review of AIR associated with immunotherapy for cutaneous or non-ocular mucosal melanoma was carried out in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Results Case 1 developed photopsia and nyctalopia with electroretinographic findings characteristic for melanoma-associated retinopathy 1 week after initiating ipilimumab/nivolumab immunotherapy. Case 2 experienced new severe bilateral visual field loss associated with anti-retinal and anti-optic nerve antibodies while on maintenance nivolumab immunotherapy. Case 3 developed decreased visual acuity due to acute exudative polymorphous vitelliform maculopathy within 2 weeks of initiating ipilimumab/nivolumab immunotherapy. All patients had concurrent extraocular immune-related adverse events in addition to the presence of anti-retinal antibodies on serological testing. 14 published cases of AIR associated with immunotherapy for cutaneous or non-ocular mucosal melanoma were identified and reviewed.
Conclusions Immune checkpoint inhibition can trigger the development of AIR with varied clinical manifestations in patients with advanced cutaneous melanoma. This study highlights the need for close monitoring in cutaneous melanoma patients receiving immunotherapy who develop new visual symptoms with or without funduscopic changes, as well as the potential role for screening of patients prior to initiating immunotherapy.
- retina
- immunology
- diagnostic tests/investigation
- electrophysiology
- treatment other
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Immunotherapy for the treatment of cutaneous melanoma may induce autoimmune retinopathy (AIR).
What are the new findings?
AIR induced by immunotherapy may have a variety of manifestations.
Visual prognosis of immunotherapy-induced AIR is variable.
How might these results change the focus of research or clinical practice?
It is important to recognise AIR early.
Screening prior to initiating immunotherapy may be warranted.
Collaboration with a medical oncologist is crucial in the management of these complex cases.
Introduction
The combination of nivolumab and ipilimumab has recently emerged as a first-line treatment for advanced cutaneous melanoma. Both nivolumab and ipilimumab are checkpoint inhibitors of immune cellular proliferation and function.1–3 Nivolumab is a human monoclonal antibody directed against programmed cell death protein 1 (PD-1). Ipilimumab is a human monoclonal antibody directed against cytotoxic T lymphocyte-associated protein 4 (CTLA-4). The two agents block non-redundant inhibitory pathways in T cell activation and therefore enhance host immune responses against malignant cells. They have been shown to improve overall survival in patients with advanced cutaneous melanoma among other cancers.1 2
Both ipilimumab and nivolumab, however, often cause immune-related adverse events (irAEs) with an incidence as high as 96% when used in combination.2 Severe irAEs requiring treatment occur in up to 59% of patients receiving combination therapy, which contrasts with the lower incidence of such irAEs among patients receiving monotherapy with nivolumab alone (21%) or ipilimumab alone (28%).2 Discontinuation of therapy was required more frequently with combination therapy than with monotherapy, further demonstrating the cumulative proinflammatory effect of these agents.2
The most common irAEs are dermatological, occurring at rates as high as 62%, while gastrointestinal and endocrine organ toxicities occur in up to 51% and 34% of patients, respectively.1 2 Ophthalmic irAEs secondary to immunotherapy are relatively rare with a reported incidence of about 1%.4 5 Roberts et al suggested the possible exacerbation of melanoma-associated retinopathy (MAR) after initiating pembrolizumab, a monoclonal anti-PD-1 antibody, in a patient with metastatic cutaneous melanoma.6 Kim et al4 were the first to report MAR in the setting of nivolumab and ipilimumab. For context, the first reports of MAR were published in the 1980s,7–9 long before the advent of immunotherapy. MAR encompasses a spectrum of autoimmune retinopathy (AIR) in patients with melanoma. MAR is analogous to carcinoma-associated retinopathy (CAR), an entity that is associated with rod and cone dysfunction due to non-ocular carcinoma. MAR and CAR both fall under the category of AIR, which includes various retinal pathologies resulting from molecular mimicry between antigens—either neoplastic or non-neoplastic—and various retinal proteins.10
It is conceivable that immunotherapy for melanoma could lead to the generation of new autoantibodies or increased titers of existing autoantibodies with resultant retinopathy. Herein, we present three cases of AIR associated with nivolumab/ipilimumab immunotherapy for advanced cutaneous melanoma and a systematic review of AIR cases related to immunotherapy for cutaneous and non-ocular mucosal melanoma. We highlight the remarkable variability of its clinical presentation and argue in favour of a causal relationship between immunotherapy and AIR given the development of symptoms after initiating immunotherapy.
Materials and methods
A retrospective chart review was performed on patients with advanced cutaneous melanoma treated at the Yale Cancer Center who developed visual symptoms after initiating immunotherapy between 1 July 2017 and 30 June 2021. Complete ophthalmic examination was performed on each patient, including ancillary testing such as optical coherence tomography (OCT), automated visual field testing, and electroretinography (ERG). The presence of anti-retinal antibodies was confirmed by Western blot and/or immunohistochemical staining by the Ocular Immunology Laboratory, Oregon Health and Science University. Ophthalmic and systemic outcomes after treatment for AIR were followed over time.
A systematic review was carried out in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines11 where applicable (protocol in online supplemental information). Inclusion criteria included PubMed-indexed articles, articles written in English, onset of visual symptoms after initiation of immunotherapy for cutaneous or non-ocular mucosal melanoma and clinical evidence of AIR. Exclusion criteria included immunotherapy for malignancies other than cutaneous or non-ocular mucosal melanoma and onset of visual symptoms or ocular findings prior to initiation of immunotherapy. A search was carried out on PubMed using the following search terms: “melanoma” AND (“retinopathy” OR “maculopathy”) AND (“immunotherapy” OR “checkpoint inhibitor” OR “pembrolizumab” OR “nivolumab” OR “ipilimumab”). Studies were screened and assessed for eligibility by a single reviewer. Studies selected for inclusion were then reviewed by two independent reviewers. A flow diagram depicting the systematic review process was created using the PRISMA2020 ShinyApp.12 Variables sought included the patient’s sex, patient’s age, immunotherapy at the onset of visual symptoms, onset of visual symptoms after initiation of immunotherapy, best-corrected visual acuity (BCVA) at presentation, ocular finding(s), anti-retinal antibodies detected, concurrent systemic irAE(s), treatment for AIR, cessation of immunotherapy and duration of follow-up. Outcome measures included ocular outcomes and systemic outcomes if reported. Simple percentages of outcome measures were calculated. For measures involving time, median and interquartile range (IQR) were calculated. Missing data were recorded as ‘not reported’. The synthesised data were presented in a table.
Supplemental material
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
The main findings of the three cases are summarised in table 1.
Summary of cases in case series
Case 1
A Caucasian woman in her late 70s presented with two large, palpable left inguinal lymph nodes and was found to have stage IIIC cutaneous melanoma 8 years after wide local excision of a stage IA cutaneous melanoma of the left ankle. She developed photopsia within one week after starting her first cycle of ipilimumab (3 mg/kg) and nivolumab (1 mg/kg). Her BCVA was 6/7.5 in both eyes (OU) and her ophthalmic exam, including dilated fundus exam and macular OCT, were unremarkable (figure 1). Immunotherapy was continued for two more cycles, after which she developed transaminitis, hypopituitarism and dermatitis in addition to worsening photopsia and nyctalopia. Radiologic staging studies conducted after her third cycle of immunotherapy confirmed regression of her inguinal lymphadenopathy. Immunotherapy was discontinued, and high-dose intravenous corticosteroids were administered. A full-field electroretinogram (ERG) (Desktop E3 Diagnosys, Lowell, Massachusetts, USA) revealed attenuated b-wave amplitudes but preserved a-wave amplitudes OU (figure 1), indicative of bipolar cell dysfunction. The presence of anti-GAPDH, anti-arrestin, anti-enolase and anti-TRPM113 antibodies were confirmed on Western blot; antibodies against photoreceptors and bipolar cells were detected on immunohistochemistry (Ocular Immunology Laboratory, Oregon Health and Science University). With the initiation of high-dose corticosteroids and intravenous immunoglobulin (IVIG), her BCVA stabilised to 6/7.5 OD, 6/9 OS. She was maintained on a slow prednisone taper but symptoms of nyctalopia persisted at 18 months after the onset of visual complaints and b-wave amplitudes remained severely attenuated on repeat full-field ERGs. Her visual acuity gradually declined to 6/9 OD, 6/18 OS at last follow-up. She subsequently developed mononeuritis multiplex with subacute left-sided weakness, constipation and urinary retention. This progressed to involve the diaphragm, causing hypoventilation and hypercapnia. She reported stable vision and declined further follow-up with the Ophthalmology service. She died from progressive respiratory failure 34 months after her initial visual symptoms.

(Case 1) Macular OCT of (A) right eye and (B) left eye. (C) ERG of both eyes showing preserved a-wave (indicated by "a") and diminished b-wave (indicated by "b") responses, typical of melanoma-associated retinopathy. ERG, electroretinography; OCT, optical coherence tomography.
Case 2
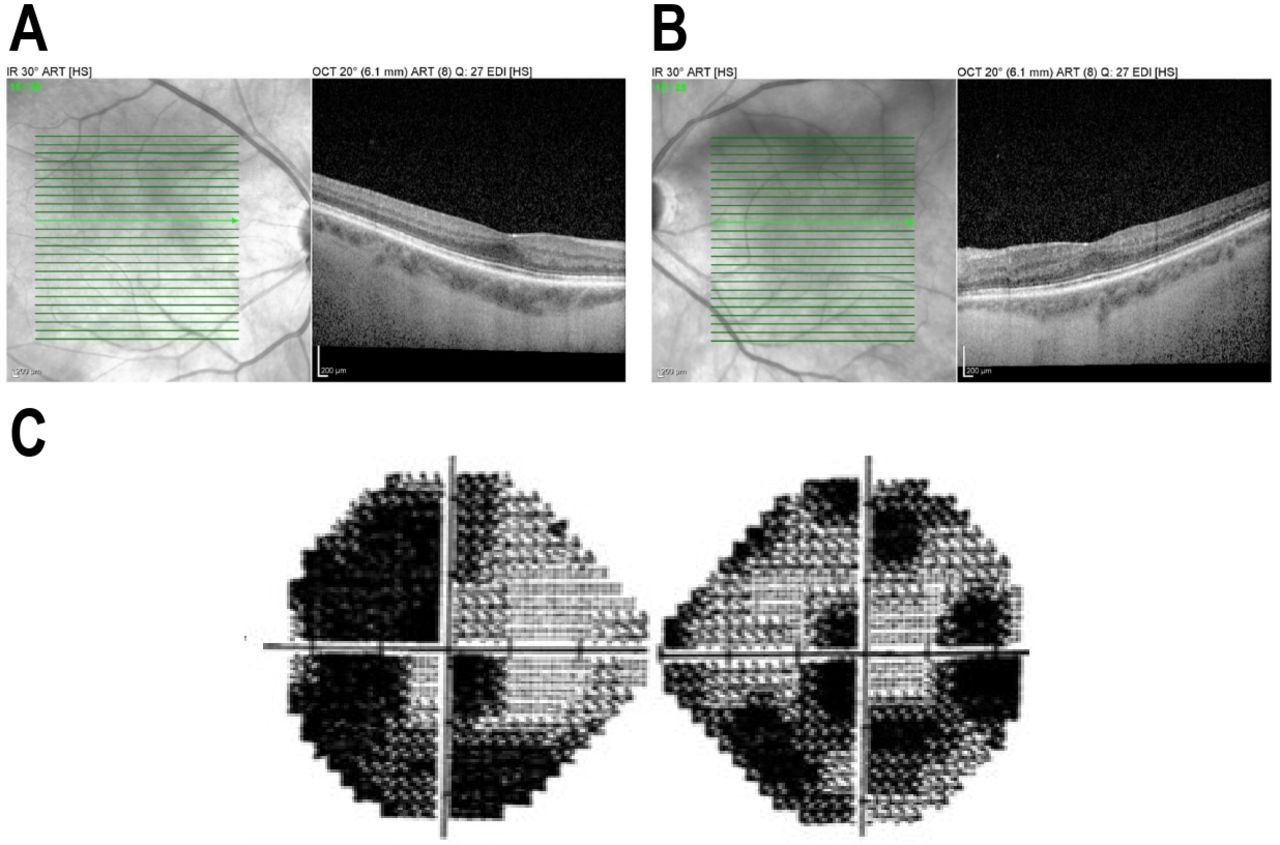
A Caucasian woman in her late 50s presented with a large palpable right-upper quadrant mass that was found to be a hepatic metastasis from stage IV cutaneous melanoma. She underwent four induction cycles of ipilimumab (3 mg/kg) and nivolumab (1 mg/kg) followed by 48 cycles of maintenance nivolumab monotherapy (240 mg). Her treatment course was complicated by a pulmonary sarcoidosis-like reaction and pneumonitis treated with systemic corticosteroids and temporary cessation of nivolumab monotherapy. When she reported floaters after cycle 48 of nivolumab (34 months after initiation of immunotherapy), silt lamp and funduscopic examination revealed posterior vitreous detachment without intraocular inflammation. Nivolumab monotherapy was continued through cycle 52, after which she noticed visual field deficits. BCVA was 6/7.5 OU. Repeat ophthalmic exam was unchanged and Macular OCT was unremarkable (figure 2). Automated visual field testing demonstrated bilateral concentric visual field defects (figure 2). ERG demonstrated normal scotopic a- and b-wave amplitudes in both eyes. Antibodies against recoverin, aldolase, enolase, transducin-α,14 TRPM113 were present on MAR Western blot; antibodies against bipolar cells were detected on immunohistochemistry (Ocular Immunology Laboratory, Oregon Health & Science University). In addition, anti-optic nerve antibodies were detected, suggesting autoimmune optic neuropathy as a contributor to her progressive visual field loss. Radiologic staging studies found a near-complete response of her melanoma with dramatic regression of her hepatic metastasis. Immunotherapy was discontinued. After she received intravenous immunoglobin (IVIG), Rituximab and plasma exchange therapy, her visual symptoms and visual field deficits neither improved nor progressed. She had melanoma recurrence in a portacaval lymph node that was resected via robotic surgery two years after discontinuation of immunotherapy. Her visual field deficits remained unchanged 31 months after onset of her visual symptoms, with visual acuity at 6/7.5 OD, 6/6 OS. She remained melanoma-free at last follow-up.

(Case 2) Macular OCT of (A) right eye and (B) left eye. (C) Humphrey visual field 24–2 demonstrates bilateral concentric visual field loss. OCT, optical coherence tomography.
Case 3
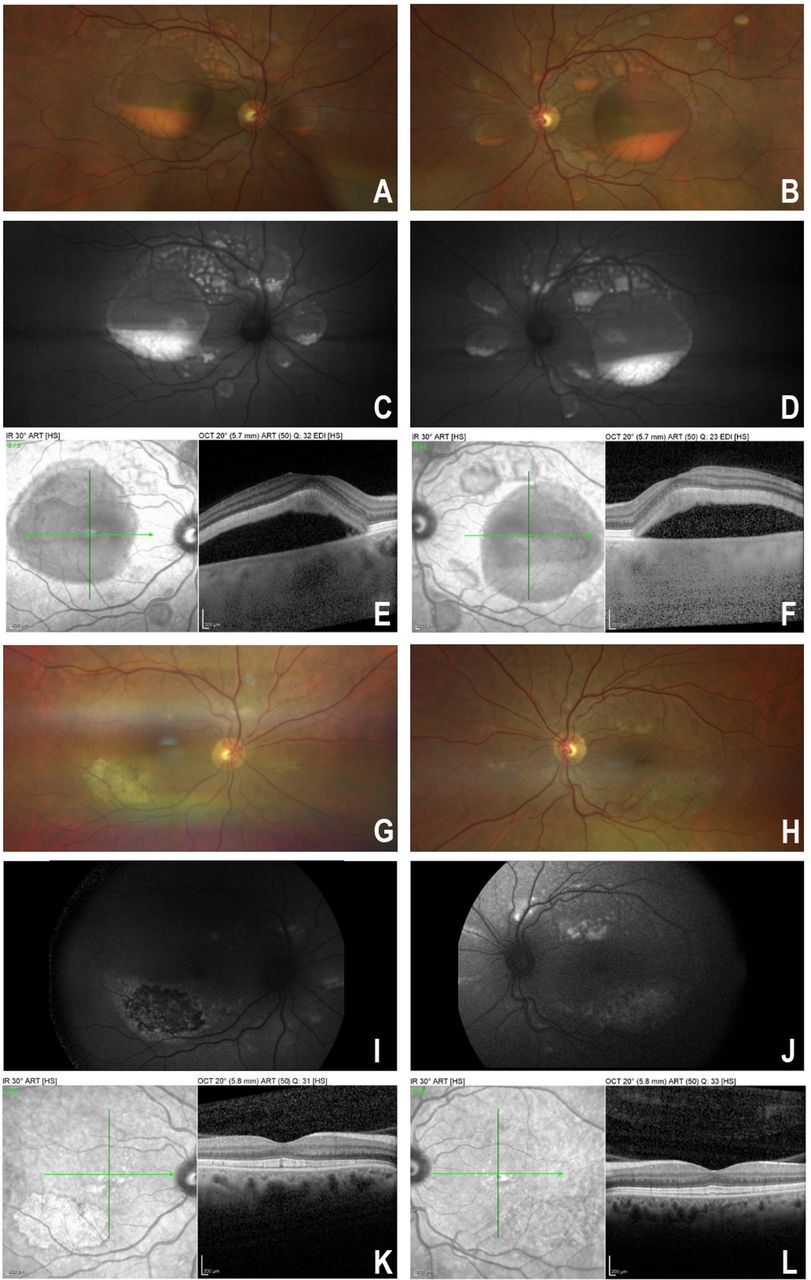
A Caucasian male in his early 50s presented with a 5 mm pigmented lesion under the toenail of his large right toe and two enlarged right inguinal lymph nodes consistent with stage IIID acral lentiginous melanoma. He underwent one cycle of ipilimumab (3 mg/kg) and nivolumab (1 mg/kg) and within two weeks of beginning therapy developed blurred vision OU. He had concurrent hypothyroidism and vitiligo that were thought to be irAEs. His BCVA at that time was 6/12 OD and 6/9 OS with a normal funduscopic examination. One month later when he complained of worsening blurring of vision, BCVA was 6/30 OD, 6/21 OS. Bilateral serous retinal detachments and vitelliform deposits (figure 3A–F), consistent with acute exudative polymorphous vitelliform maculopathy (AEPVM), were found. ERG revealed normal b-wave amplitudes under both photopic and scotopic conditions, but electro-oculography (Diagnosys Espion 3 desktop model) demonstrated a decreased Arden ratio of 1.4 OU (normal ≥1.8) indicating decreased trans-retinal pigment epithelial voltage potential. The patient was found to have anti-bestrophin 1 antibodies (Ocular Immunology Laboratory, Oregon Health and Science University), which have been associated with paraneoplastic AEPVM.15 He also manifested anti-retinal antibodies against arrestin, enolase and transducin-α on Western blot as well as anti-bipolar cell antibodies on immunohistochemistry.14 Immunotherapy was discontinued after the first cycle as a result of his ocular findings. He declined treatment with intravenous immunoglobulin (IVIG). He was treated with posterior sub-Tenon’s corticosteroid injections and had gradual resolution of the subretinal fluid over 20 months with slow improvement of his BCVA to 6/6 OU; however, the vitelliform lesions persisted for 39 months. Unfortunately, his systemic disease progressed, with development of new bulky right iliac lymphadenopathy and right adrenal metastasis. He underwent surgical debulking of the right iliac lymphadenopathy and adjuvant radiation therapy. He was initially maintained on Dasatinib. However, he developed further progression of his melanoma with new metastases in his chest, abdomen, pelvis, scrotum and inguinal nodes. He also developed new right cerebellar and right superior parietal lobe lesions and underwent gamma-knife radiation therapy. Nivolumab was restarted with Sorafenib approximately one year after his initial visual symptoms, with partial response of his melanoma to treatment on repeat imaging and no recurrence of his visual symptoms. At 39 months since the onset of visual symptoms, the vitelliform lesions have regressed (figure 3G–L) and his visual acuity remained stable at 6/6 OU.

{kind=link}
{kind=link}
{kind=link}
(Case 3) Fundus photographs of right eye and left eye show multiple, well-circumscribed areas of serous retinal detachments with gravitational pooling of vitelliform deposits in each cavity (A, B). Autofluorescence images demonstrate hyperfluorescence of the pooled fluid (C, D). Macular OCT through the largest macular serous detachment in each eye showing subretinal fluid and hyperreflectivity corresponding to the vitelliform deposits (E, F). Fundus photographs of right eye and left eye show resolution of areas of serous retinal detachments (G, H). Autofluorescence images demonstrate residual hyperfluorescence of resolved areas of retinal detachment (I, J). Macular OCT showing resolution of subretinal fluid (K, L). OCT, optical coherence tomography.
Systematic review
53 records were identified and screened using the specified search strategy (see flow diagram, (online supplemental figure 1). 20 reports appeared to meet inclusion criteria and were sought for retrieval. Of the 20 reports, 1 was excluded because the malignancy treated by immunotherapy was neither cutaneous melanoma nor non-ocular mucosal melanoma.16 6 reports were excluded because visual symptoms or ocular findings were reported prior to the initiation of immunotherapy.6 17–21 14 patients from 13 reports were included in the review22–34 (online supplemental table 1). The patient and ocular characteristics of these cases are summarised in table 2. The most common immunotherapy implicated was nivolumab monotherapy (5/14 patients), followed by pembrolizumab monotherapy (3/14 patients) and ipilimumab/nivolumab combination therapy (3/14 patients). The most common ocular symptoms were blurred vision (6/14 patients), unspecified vision loss (5/14 patients) and photopsia (5/14 patients). The median onset of visual symptoms after initiation of immunotherapy was 7.5 weeks (IQR 5.25–19.75 weeks), with a range of 3 days to 2 years. All patients had bilateral ocular involvement. The retinal findings ranged from classic MAR (4/28 eyes), AEPVM (12/28 eyes), serous retinal detachment (10/28 eyes) to birdshot-like chorioretinopathy (2/28 eyes). Only one patient was tested for anti-retinal antibodies and had a positive result. Concurrent systemic irAEs were reported in 6 out of 14 patients. 12 out of 14 patients were treated with topical, periocular, intravitreal and/or systemic corticosteroids. 10 out of 14 patients required cessation of immunotherapy. Of the only 5 patients who had the outcome of their underlying melanoma reported, 3 patients had progression of disease. The median duration of follow-up was 17 weeks (IQR 4.75–26 weeks).
Summary of patient and ocular characteristics in systematic review
Discussion
This study illustrates the spectrum of AIR associated with anti-retinal antibodies after initiation of immunotherapy in patients with advanced cutaneous melanoma. In all three cases, visual symptoms developed after the initiation of immunotherapy with ipilimumab and nivolumab. The visual symptoms in two cases occurred within two weeks after initiation of immunotherapy (case 1 and 3) and one case (case 2) demonstrated insidious visual field deficits detected during the maintenance phase of immunotherapy. In our systematic review of published cases, the onset of visual symptoms was also highly variable, ranging from within a week to 2 years with a median of 7.5 weeks after the initiation of immunotherapy.
The presence of anti-retinal antibodies, coupled with the co-occurrence of well-documented irAEs such as endocrinopathy (cases 1 and 3),1 2 35 36 pulmonary sarcoidosis-like reaction and pneumonitis (case 2),37–40 suggests that the heightened immune response triggered by immunotherapy may have played an important role in the pathogenesis of AIR. Notably, all three patients were treated with both ipilimumab and nivolumab, which showed a higher rate of irAEs when used in combination.2 Without routine pretreatment serological screening, it is not possible to determine if these anti-retinal antibodies were already present at subclinical levels before initiation of immunotherapy or if the anti-retinal antibodies were generated as part of a wider autoimmune response triggered by immunotherapy. Indeed, a study by Duvoisin et al41 detected the presence of anti-TRPM1 autoantibodies in 5 out of 15 patients with advanced cutaneous melanoma without visual symptoms compared with weak positivity to these autoantibodies in 1 out of 50 controls without cancer, suggesting that patients with cutaneous melanoma may be more prone to developing anti-retinal antibodies, with or without visual symptoms, than the general population. However, the relevance of individual anti-retinal antibodies as markers of immunotherapy-induced AIR remains incompletely understood. Chen et al found the presence of anti-retinal antibodies against at least one retinal antigen in 13 out of 14 patients without AIR, although 10 of these patients had macular or optic nerve disease.42 Interestingly, none of these patients tested positive for anti-recoverin antibodies, suggesting that anti-recoverin antibodies may be possibly more specific to AIR. Given the high rate of positivity for anti-retinal antibodies even in patients without AIR, the presence of anti-retinal antibodies would need to be interpreted in the appropriate clinical context.
Despite some overlap in the specific anti-retinal antibodies detected between the three cases presented in this study, there is marked variation in the clinical presentation across the three cases. Case 1 may be considered a classic case of melanoma-associated retinopathy (MAR) given the characteristic negative b-wave on ERG in the absence of abnormal fundus findings, albeit with the development of visual symptoms soon after initiation of immunotherapy. In contrast, case 2 presented with profound visual field deficits associated with both anti-retinal and anti-optic nerve antibodies.43–48 The long delay in onset of visual symptoms after initiation of immunotherapy makes MAR unrelated to immunotherapy a possibility, although the patient’s visual symptoms and visual field deficits stabilised after immunotherapy cessation and immunosuppressive treatments. Case 3 is an example of acute exudative polymorphous vitelliform maculopathy (AEPVM), which is also termed acute exudative polymorphous paraneoplastic vitelliform maculopathy (AEPPVM) when found in the context of a malignancy.15 49–52 Paraneoplastic AEPVM or AEPPVM is characterized by the presence of antibodies against the retinal pigment epithelium (e.g. anti-bestrophin 1 or anti-peroxiredoxin 3 antibodies) in addition to a decreased Arden ratio on EOG, serous retinal detachments and vitelliform lesions resembling Best vitelliform macular dystrophy.15 49 51–57 Although AEPVM in Case 3 could be unrelated to immunotherapy, the timing of ocular symptoms and systemic irAEs after immunotherapy initiation support a causative role for immunotherapy. In our systematic review of published cases, there was a spectrum of retinal findings ranging from classic MAR, AEPVM, serous retinal detachment to birdshot-like chorioretinopathy after immunotherapy initiation.
Although it is difficult to make management recommendations based on the small number of cases included in this series, the occurrence of new visual symptoms after initiation of immunotherapy in patients should warrant a prompt ophthalmology evaluation due to the persistence of visual symptoms in a significant proportion of patients despite treatment. Two out of three patients in our case series did not have complete resolution of visual symptoms despite intravenous immunoglobin (IVIG) and systemic immunosuppressive treatments. The patient in case 1 had persistence of decreased dark adaptation despite treatment. Likewise, case 2 demonstrated no improvement in visual field loss following treatment. The patient in case 3 declined IVIG and had gradual resolution of subretinal fluid and visual symptoms over 20 months after treatment with periocular corticosteroid injections. Similarly, in our systematic review of published cases, only 5 out of 14 patients (10 out of 28 eyes) had complete resolution of visual symptoms. The most common visual symptoms reported in our cases series and systematic review were blurred vision, unspecified vision loss and photopsia. Nyctalopia, metamorphopsia, visual field deficits and photophobia were also reported. Notably, all patients had bilateral involvement.
The management of advanced cutaneous melanoma in these patients also merits discussion. Although the development of AIR is a relative contraindication to further continuation of immunotherapy, the decision to discontinue immunotherapy represents a therapeutic dilemma that must be balanced against prevention of systemic melanoma progression or recurrence. Only case 1 had a durable systemic response to immunotherapy even after its discontinuation, but she ultimately succumbed to complications associated with mononeuritis multiplex, an irAE. The remaining two cases had recurrence or progression of metastatic cutaneous melanoma following discontinuation of immunotherapy. Case 2 had recurrence at a single portacaval lymph node that was resected but otherwise remained melanoma-free. Case 3 had progression of systemic metastasis that required single-agent immunotherapy with no apparent recurrence of his AIR. Similarly, in 5 out of 14 published cases in which the systemic outcome was reported, 3 cases had progression of their underlying melanoma.
One of the limitations of this case series is the relatively small number of patients due to the rarity of the condition. However, some of our findings were mirrored in our systematic review of published cases. Furthermore, because patients do not routinely undergo serological testing for anti-retinal antibodies and/or evaluation by an ophthalmologist before starting immunotherapy, it cannot be established if these patients have pre-existing AIR that were exacerbated by immunotherapy or new-onset AIR induced by immunotherapy. It is possible that anti-retinal antibodies were present prior to initiation of immunotherapy but the retinopathy only became clinically evident after immunotherapy in these patients.
The limitations of our systematic review include the relatively small number of published cases and their heterogeneity, which limit the scope for an extensive meta-analysis. Furthermore, there is notable variability in clinical practice across the published cases such as the route of administration of corticosteroids. There is also variability in the reporting of variables and outcomes in these cases. For example, variables such as the presence or absence of systemic irAEs as well as systemic melanoma status on follow-up were frequently omitted.
A larger study could evaluate the role of screening patients for baseline anti-retinal antibodies prior to initiation of immunotherapy. Prospective screening of patients may better elucidate the natural history and the spectrum of AIR precipitated by immunotherapy. As the clinical utilisation of immunotherapy expands, there may be an increasing role for the utilisation of risk factors for irAEs which may impact the management of cutaneous melanoma.
Conclusion
AIR remains a poorly understood and likely under-recognised complication of advanced cutaneous melanoma which may be triggered or exacerbated by immunotherapy. Given the diversity of presentations, AIR must be on the differential diagnosis for cancer patients who develop visual symptoms of floaters, photopsia, visual field deficit and/or decreased visual acuity after initiating immunotherapy. Collaboration between the patient’s ophthalmologist and medical oncologist is crucial for individualised management and monitoring of AIR associated with immunotherapy.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Each patient gave informed consent to publish relevant data. The collection of data was approved by the Yale University Institutional Review Board (Protocol ID: 2000025398). This retrospective chart review adhered to the ethical principles outlined in the Declaration of Helsinki.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JSH, JMK, DKJ, KMS and RP-L contributed to the design of the study, data acquisition, data interpretation as well as writing of the manuscript. JSH and RP-L performed the systematic review. SAW, MS, HMK, SDW and NAS contributed to data interpretation and writing of the manuscript. RP-L accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests HMK reports research grants from Merck, Bristol-Myers Squibb and Apexigen. She receives personal fees from Regeneron, Alexion, Prometheus, Corvus, Nektar, Biodesix, Roche-Genentech, Pfizer, Iovance, Immunocore and Celldex. MS is a paid consultant for Genentech-Roche, Bristol-Myers, Astra-Zeneca/Medimmune, Novartis, Seattle Genetics, Nektar, Lilly, Biodesix, Modulate Therapeutics. Newlink Genetics,Molecular Partners, Innate Pharma, Abbvie, Immunocore, Genmab, Almac, Hinge, Allakos,Anaeropharma, Array. He is also on the scientific advisory board for Symphogen, Adaptimmune,Omniox, Pieris, Torque (also receives consulting fees+stock options) and Verseau. SDW is a consultant for Allergan, Genentech and Castle Biosciences. SAW is a consultant for Array Biopharma and Magellan Rx.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.