Article Text

Abstract
Melanoma associated retinopathy is a rare paraneoplastic complication of metastatic cutaneous malignant melanoma. It may present years after the original diagnosis of melanoma. Here we describe a patient with this condition who presented with persistent photopsias and visual loss. We will discuss the electroretinographic findings and their utility.
Statistics from Altmetric.com
The story
Three months prior to presentation, a 67-year-old woman first noticed ‘lights’ in the outer lower quadrant of the visual field of her left eye. She described them as ‘resembling ripples in water with light shining on it’. They were noticeable all the time, both in the dark and in the light. Over the next 2 months these gradually spread to all areas of vision in both eyes, more marked peripherally than centrally. They were at their worst in bright light and first thing in the morning. Colour vision and night vision remained subjectively normal. Twelve years earlier, she had had a malignant melanoma excised from lateral to the left eyebrow with no subsequent evidence of metastatic disease. She had no other past medical history or any systemic symptoms.
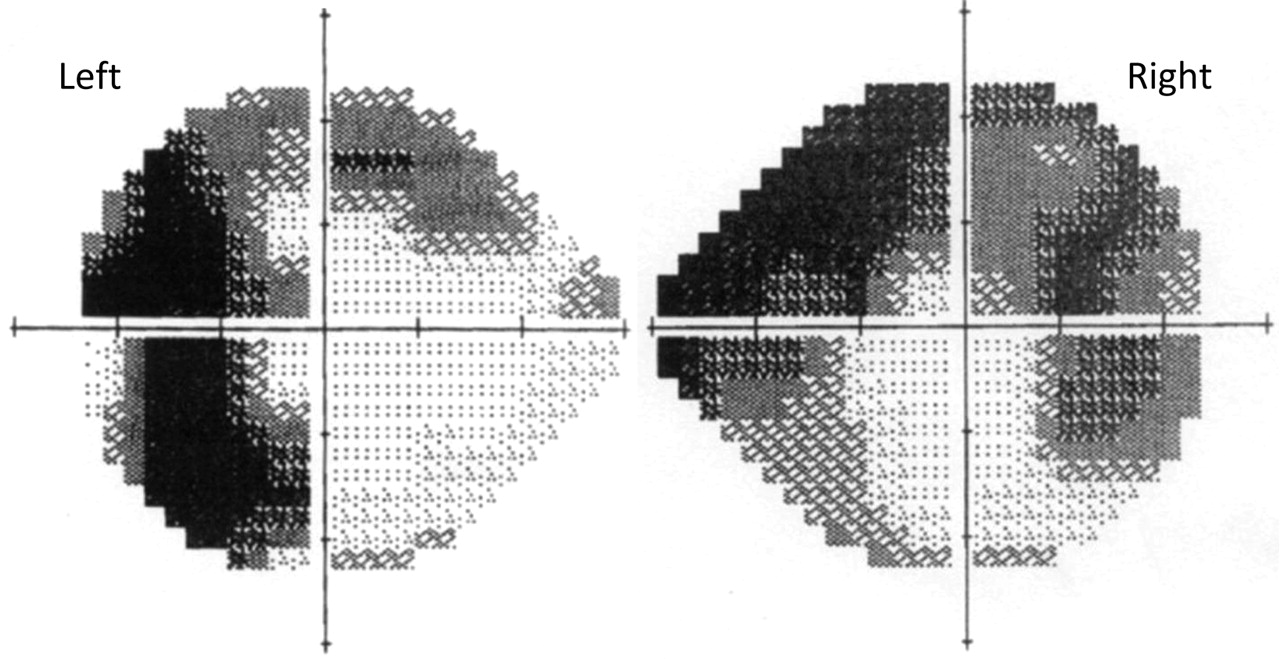
On examination, her visual acuity, colour vision and fundi were all normal with no relative afferent pupillary defect. However, although her visual fields were normal to confrontation, automated static perimetry showed large, incongruous, relative field defects in both eyes (figure 1). The remainder of the examination was normal.

Humphrey automated static perimetry showing large incongruous field defects in both eyes. The shading within each area of the visual field represents the intensity of light needed for detection—that is, the darker the area the greater the visual loss.
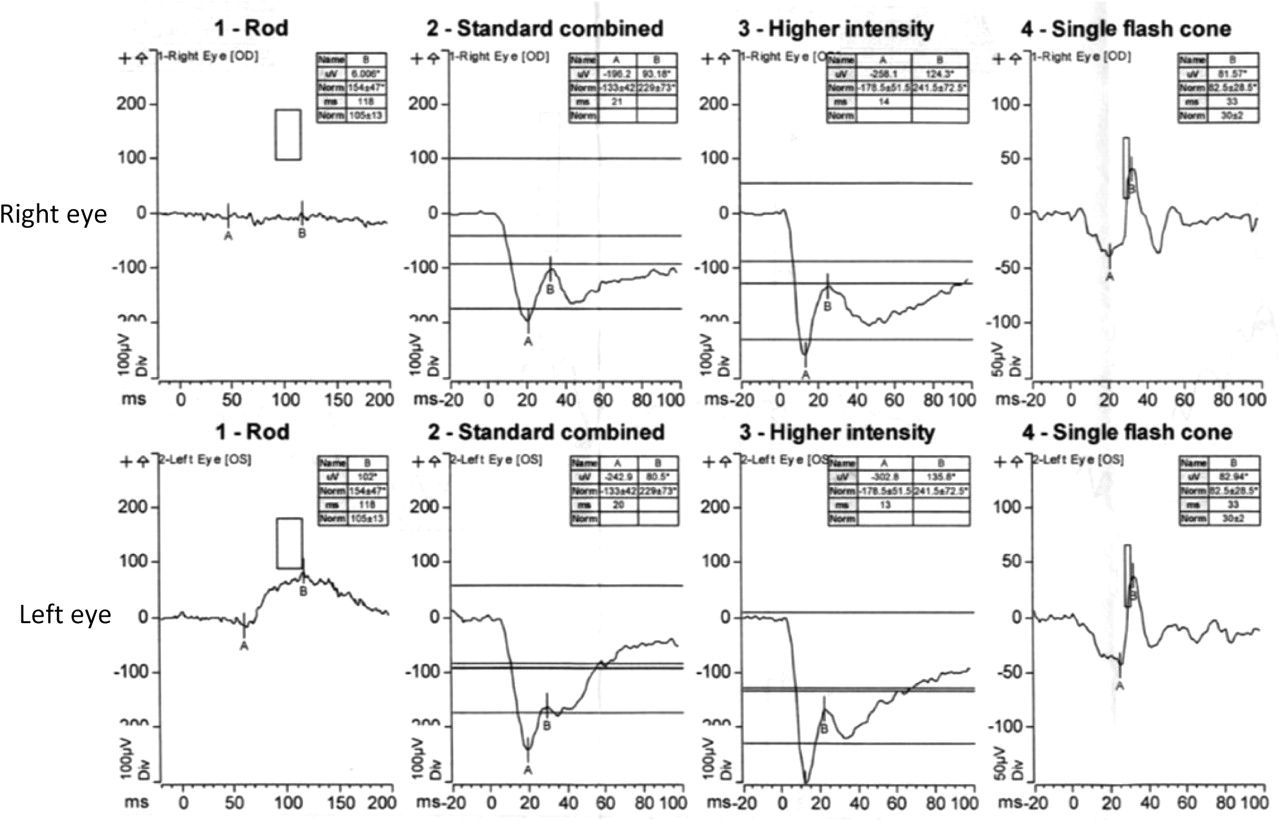
On the basis of her visual symptoms and her past history, melanoma associated retinopathy (MAR) was suspected. Scotopic flash electroretinogram (ERG) revealed an absent rod response in the right eye (figure 2) with a reduced response in the left eye. The A wave in the mixed response was normal but the B wave was reduced such that the mixed ERG never became positive (a so-called ‘negative ERG’) (figure 2). Photopic cone responses were normal in amplitude but delayed (figure 2), and 30 Hz flicker responses were also normal (not shown). Pattern ERG (a measure of ganglion cell response) showed reduced amplitudes (figure 3). In the long flash ERG, the ‘off’ response was normal while the ‘on’ response was reduced (figure 4). Multifocal ERG was almost normal, with just a slight increase in latency (not shown). These electrophysiological abnormalities are typical of MAR although they may also be seen in complete and incomplete congenital stationary night blindness, acquired unilateral night blindness1 (neither fit the clinical picture here), dystrophinopathy (our patient had no symptoms or signs of this) and autosomal dominant negative ERG (no family history although her family members were not examined).1 Retinoschisis, central retinal artery occlusion and central retinal vein occlusion can also give similar findings on ERG but these can be easily differentiated by their clinical features.
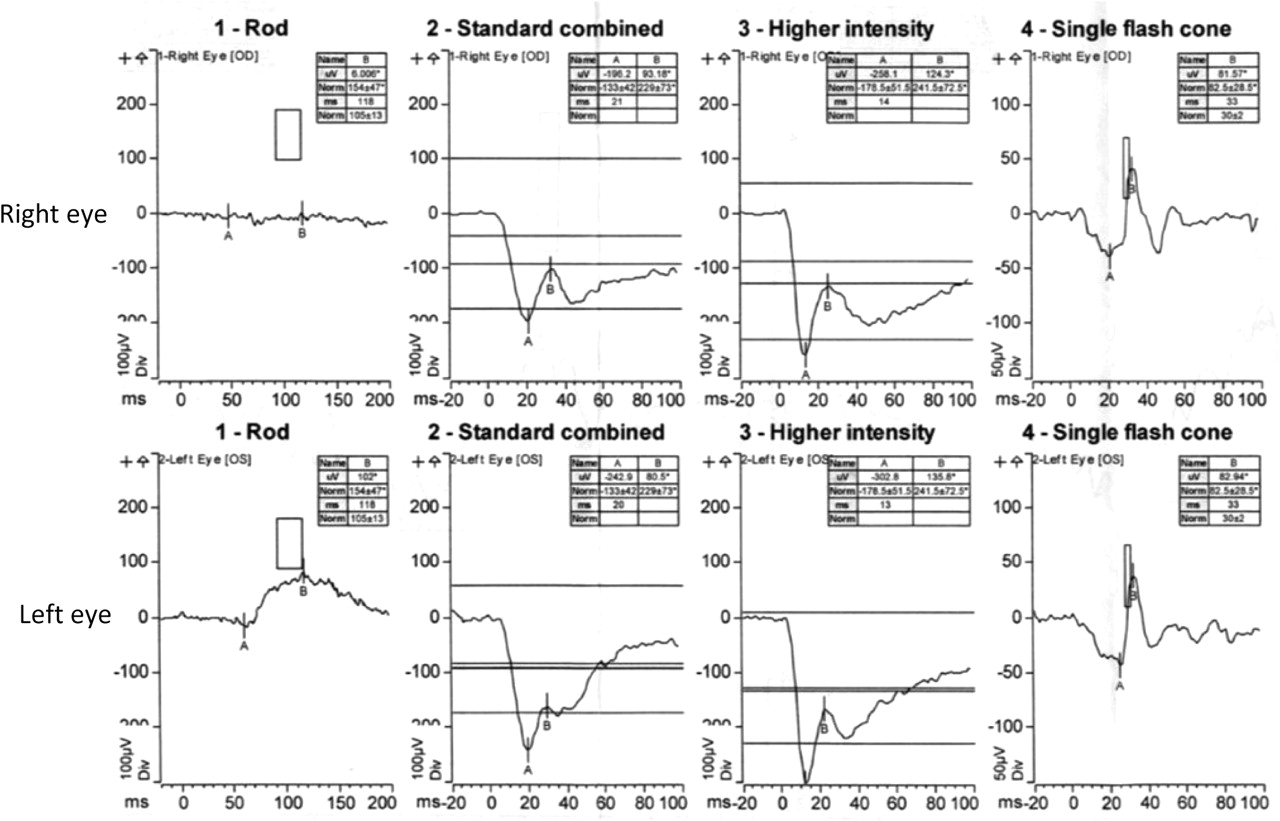
Composite flash electroretinogram (ERG) involves light and dark adapting the eye in turn and then stimulating the retina using flashes of light. The rod response (column 1) is detected by flashing a dim light into dark adapted (scotopic) eyes; in this case it is absent in the right eye (top row) and reduced in the left eye (bottom row). The boxes indicate the expected ranges of normal responses in terms of amplitude and latency. The ‘standard combined’ ERG (column 2) measures both rod and cone responses. It is performed by dark adapting the eyes and then stimulating the retina with a single flash of white light. In the recording from this patient, the A waves are of normal amplitude and duration. However, the B waves are reduced in amplitude in both eyes. B waves would normally reach positive values. As the ERG tracing does not cross the baseline this is known as a ‘negative ERG’. Reduction in B wave amplitude is thought to reflect bipolar cell dysfunction. Column 3 (‘higher intensity’) shows the standard combined ERG response to a higher intensity light flash. This is thought to improve sensitivity, especially with regard to the A wave. Again, the B wave is of reduced amplitude in both eyes. The cone responses (column 4) are detected by flashing a red light into light adapted (photopic) eyes. Here they are of normal amplitude but are slightly delayed. The rectangular boxes indicate the expected range of normal responses. The markers labelled A and B allow the magnitude of the response to be calculated, as they represent the trough and peak of the ERG recording, respectively.
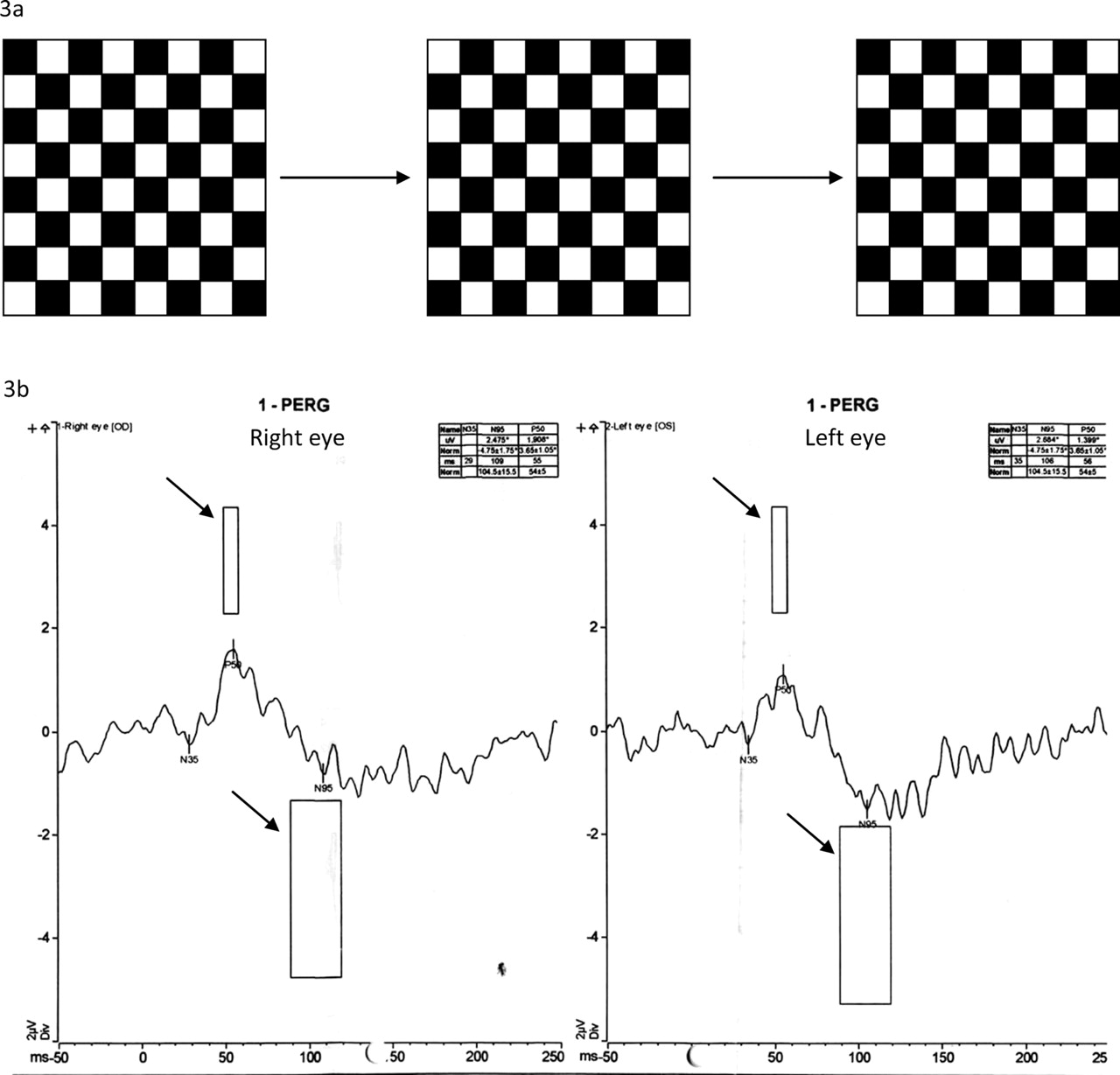
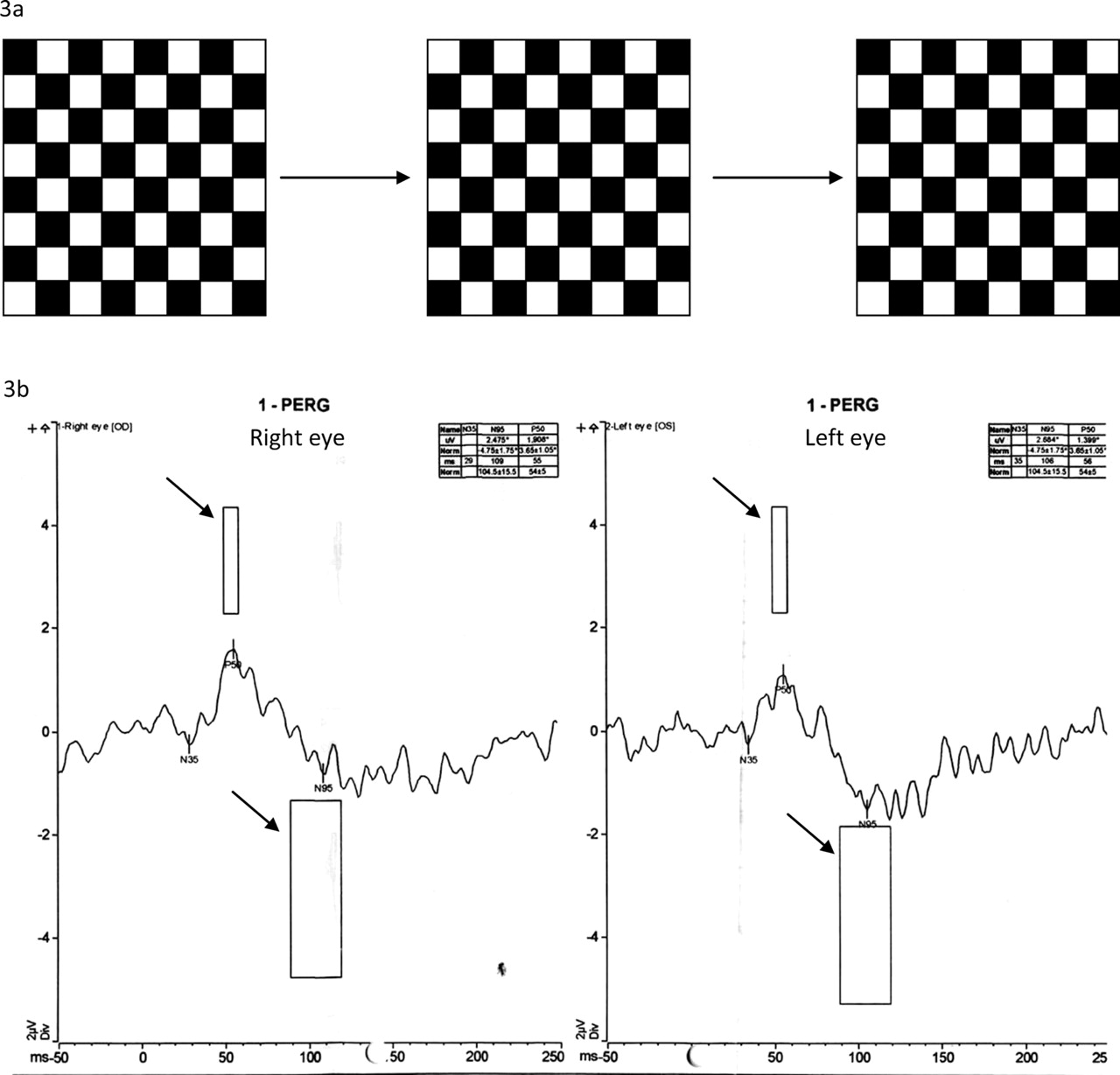
Pattern electroretinogram (PERG) is thought to assess ganglion cell function. (a) Pattern ERG checkerboard, reversed at a fixed frequency. (b) Pattern ERG recording (arrowed boxes indicate expected response). Our patient demonstrated reduced responses in both eyes.

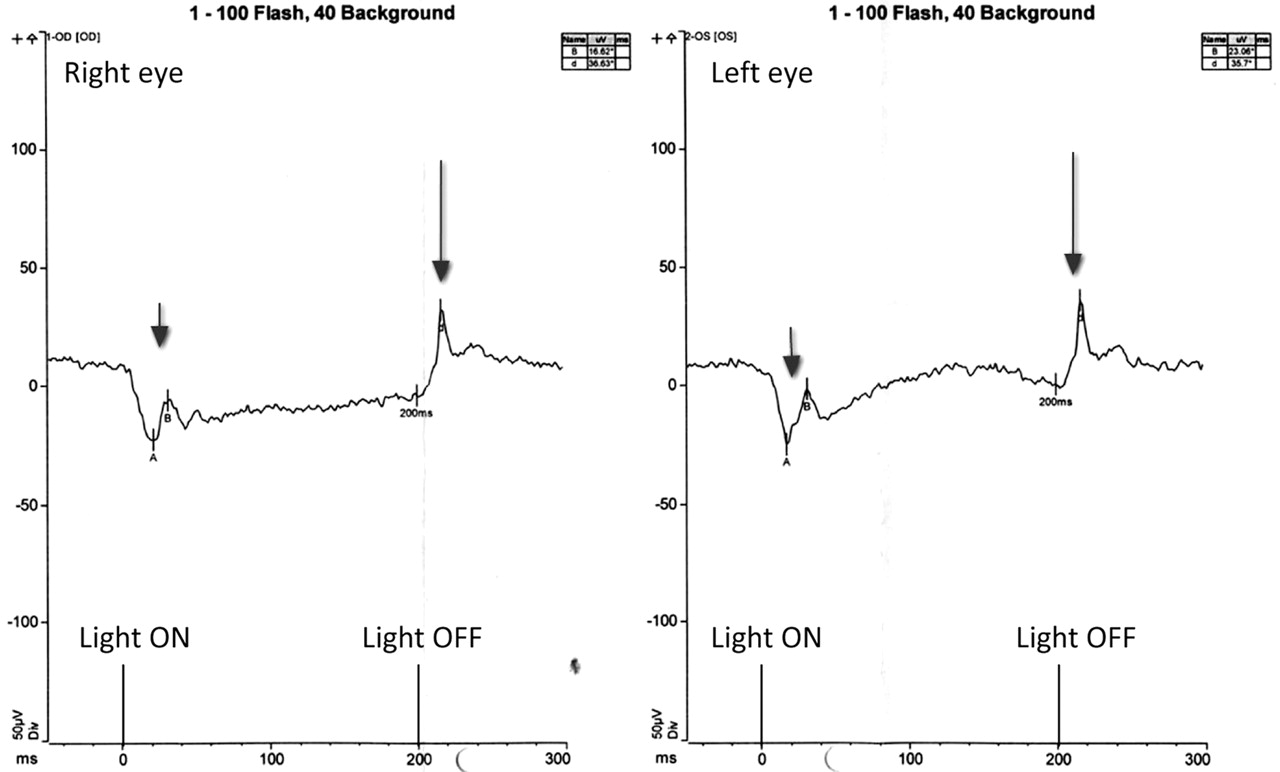
Long flash electroretinogram (ERG). A longer flash of light is used than in the standard ERG—typically 200 ms. The ‘on’ response (short arrow) is seen as the light stimulus comes on. This is attenuated in both eyes, more so in the right than the left. The ‘off’ response (long arrow) is seen as the light stimulus turns off, and is normal in both eyes. This pattern is thought to be a result of bipolar cell dysfunction.
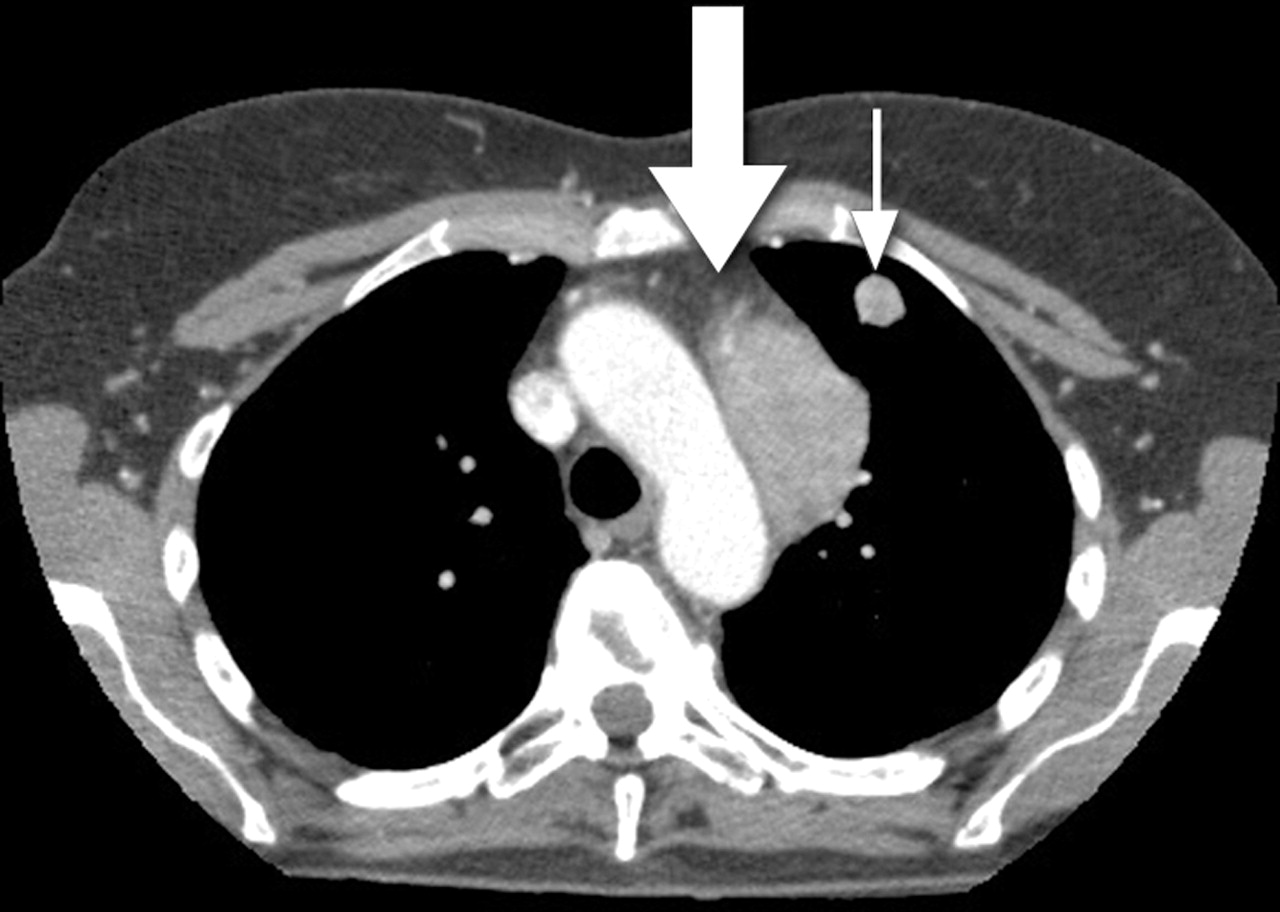
A CT body scan (figure 5) revealed two soft tissue nodules in the left lung, a large mass in the mediastinum and a destructive lesion in the T6 vertebral body. Histology of a pulmonary nodule revealed metastatic malignant melanoma. She was referred to the oncologists who decided to defer treatment until she became symptomatic from her metastatic disease. Without any specific treatment, repeat visual field assessments have shown little progression, the defects remaining largely stable 10 months after diagnosis. An attempt to treat her troublesome photopsias with carbamazepine was unsuccessful.

CT scan of the thorax shows both a mediastinal mass (large arrow) and a pulmonary nodule (thin arrow) consistent with metastases. Histology of a pulmonary nodule showed malignant melanoma.
Box 1 How the electroretinogram is performed
The electroretinogram (ERG) is a test that many neurologists may not have come across. Normally confined to the world of the retinal specialist, it is relatively non-invasive and can provide invaluable insights into retinal pathology.
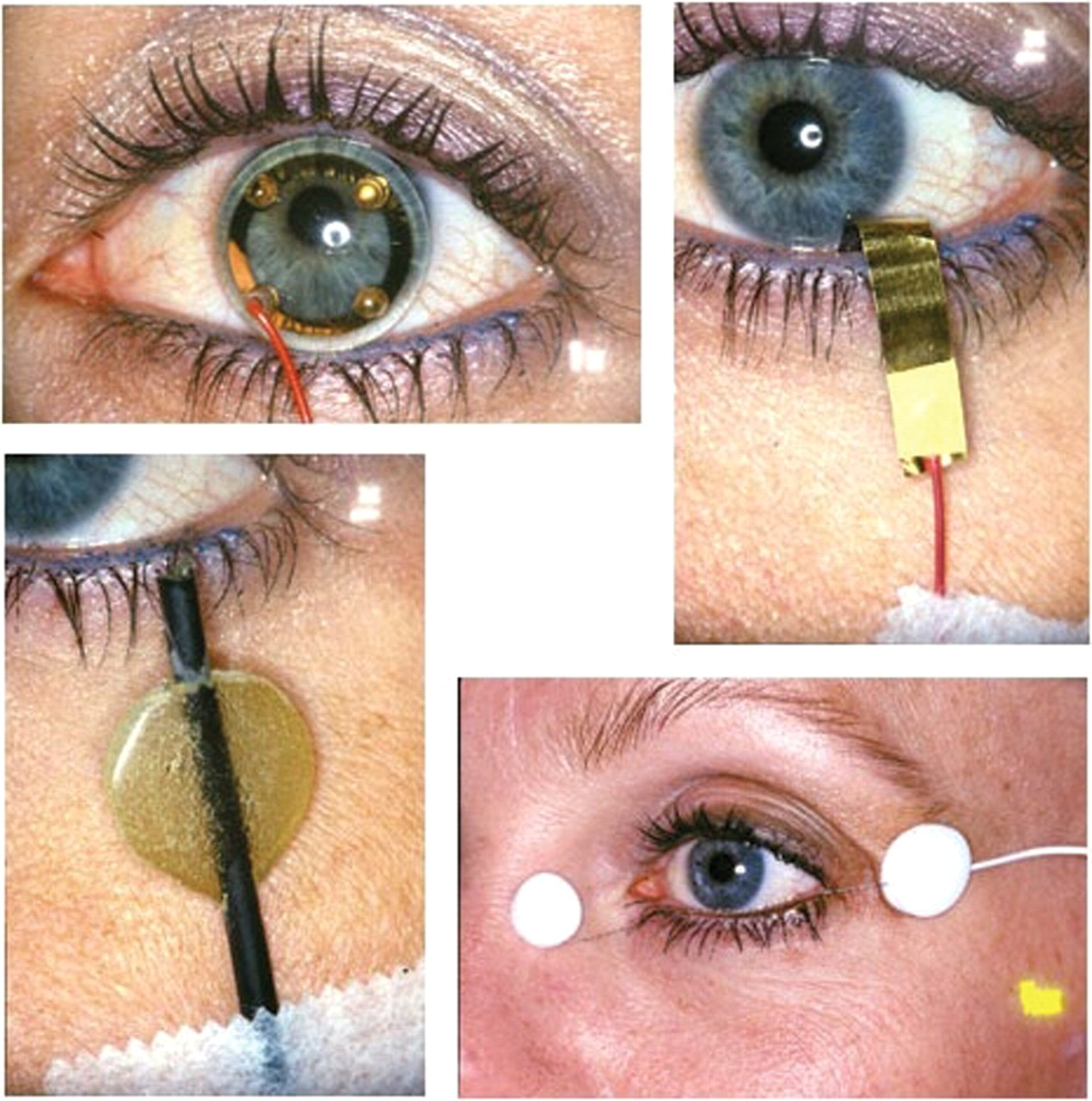
Local anaesthetic is applied to the cornea, and either a contact lens or corneal (recording) electrode is attached (figure 6). In addition to the corneal electrode, a reference (background) electrode is applied to the forehead and an earth electrode to an earlobe. The outputs from recording and reference electrodes are then fed into an amplifier and the results presented as in figure 2. The eye being examined is dark or light adapted, according to the requirements of the test being carried out.
In the flash ERG, the pupil is dilated and flashes of light with a maximum duration of 5 ms are directed onto the entire retina.
The pattern ERG is recorded in a similar manner to the flash ERG. However, the pupils are not dilated and, instead of a flash of light, there is constant light intensity throughout this test. Recordings are made while the patient focuses on a reversing checkerboard pattern similar to the stimulus used in visual evoked potentials.
The multifocal ERG is used to give spatial information about the retina whereas both the standard and pattern ERGs provide a measure of total retinal response.
Depending on the level of light adaptation, the background luminance (light intensity), and the intensity and duration of the flashes of light, a variety of retinal cells can be examined. In all recordings, time (ms) is shown on the x axis and voltage (µV) on the y axis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
There are a number of corneal electrodes that can be used. Simple electroretinogram (ERG) recording devices include contact lens electrodes and gold mylar tape that can be inserted between the lower lid and sclera. Most electrodes require an additional reference electrode to be placed on the forehead. Source: Webvision: http://webvision.med.utah.edu/ Clinical ERG chapter (permission obtained).
Discussion
MAR is a rare paraneoplastic complication of cutaneous malignant melanoma, typically presenting months to years after the initial diagnosis of melanoma but heralding the onset of metastatic disease. Symptoms include persistent shimmering, pulsating or flickering photopsias of gradual onset, with or without night blindness (nyctalopia). Occasionally the symptoms precede the diagnosis of melanoma.2 The differential diagnosis includes direct infiltration of the optic pathway by tumour cells, which can cause visual loss, but this is not usually associated with positive visual phenomena. Late retinal degeneration secondary to radiotherapy for choroidal melanoma may produce similar symptoms but MAR is not associated with choroidal melanoma for reasons that remain unclear. Although this condition is associated with the production of antiretinal antibodies, these are commonly detectable in melanoma patients with no visual symptoms.3
If patients with MAR present to a neurologist unfamiliar with the condition, they might be misdiagnosed as having some sort of migranous aura, or even as being functional. However, most patients with MAR will admit to some degree of night blindness (although our patient did not) although it may take carefully directed and close questioning to discover this. Visual field defects, as seen in our patient, would certainly direct one away from migraine. Both acute vitreous detachment4 and acute idiopathic blind spot enlargement5 can be associated with persistent photopsias with visual loss in the affected eye. These, and other causes of prolonged photopsias with visual loss, such as retinal tears, can be differentiated by careful fundoscopy through dilated pupils (reinforcing the importance of thorough fundoscopy) or, if necessary, referral to an ophthalmologist.
Causes of photopsias
Migraine: aura associated with migraine tends to occur in a hemianopic distribution, rather than monocular, although patients may not differentiate the two (the visual symptoms are more often ‘positive’ than ‘negative’). The auras tend to be stereotyped in each individual patient. Fortification spectra are among the most common visual aura. Elementary visual disturbances include colourless scotoma, photopsias or phosphenes. Simple flashes, specks or hallucinations of geometric forms (points, stars, lines, curves, circles, sparks, flashes or flames) may occur and be single or number in the hundreds. Scotomas are usually accompanied by positive visual phenomena but may occur independently.
Acute posterior vitreous detachment: symptoms are monocular, given the pathogenesis. The combination of floaters and flashing lights is typical. The classical description is of a dim white, or golden, arc of light in the temporal periphery of vision that may be visible only in dim light. In contrast, the floaters may only be noticed when looking at a light background; there may be a variety of shapes and sizes. If the vitreous detachment is associated with haemorrhage, patients may notice a red haze or mist.
Retinal detachment: similar to vitreous detachment, symptoms are monocular. However, visual loss may result from retinal detachment if it is not treated in a timely manner. Initial symptoms include positive photopsias (caused by pathological stimulation of the retina) associated with a shower of floaters. Over time, patients report progressive visual loss, the site of which depends on the site of detachment. If it is not treated, the visual loss can spread throughout the visual field over a number of days.
Melanoma associated retinopathy (MAR): symptoms can include persistent shimmering, pulsating or flickering photopsias of gradual onset, with or without night blindness (nyctalopia).
Acute idiopathic blind spot enlargement (AIBSE): symptoms are monocular. Patients present with visual loss or blurring of vision, typically affecting an area of the temporal visual field. Most patients also report photopsias in the affected area of the visual field. The photopsias may precede the visual loss, and patients may have an afferent papillary defect.
They might be misdiagnosed as having some sort of migranous aura, or even as being functional
The ERG is characteristic: a flat rod ERG, a reduction in the B wave amplitude of the mixed ERG producing a ‘negative mixed ERG’, and a selective defect of the ‘on’ response to long flashes.3
The treatment remains controversial. The natural history is said to be progressive visual loss but there are reports of prolonged stabilisation of symptoms following treatment with corticosteroids, plasma exchange or intravenous immunoglobulin.6 In the absence of controlled trials it is impossible to state with confidence that treatment results in an outcome which is any different from the untreated natural history. We elected not to treat our patient who has remained largely stable for 10 months without any intervention.
Practice points
When assessing a patient with persistent or new onset photopsias, close questioning about any visual loss is needed to exclude potentially sight threatening conditions.
If there is any concern about retinal or vitreous detachment, prompt dilated fundoscopy and ophthalmological assessment are mandatory.
If in doubt, referral to neuro-ophthamology and further assessment with ERG can be invaluable.
If the patient has had a melanoma, however long ago, always consider recurrence and melanoma associated retinopathy.
Acknowledgments
This article was reviewed by Christian Lueck, Canberra.
Footnotes
-
Competing interest None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- Unilateral electronegative ERG of non-vascular aetiology
- Distant cancer effects on standardised testing of peripheral vision
- SD-OCT and autofluorescence characteristics of autoimmune retinopathy
- Autoimmune retinopathy with associated anti-retinal antibodies as a potential immune-related adverse event associated with immunotherapy in patients with advanced cutaneous melanoma: case series and systematic review
- Mimics and chameleons of optic neuritis
- Mizuo–Nakamura phenomenon with a negative waveform ERG
- Cancer-associated retinopathy in ampullary pancreatic cancer
- Disorders of the anterior visual pathways
- Paraneoplastic retinopathy with multiple detachments of the neurosensory retina and autoantibodies against interphotoreceptor retinoid binding protein (IRBP) in cutaneous melanoma
- Electrophysiological evaluation of visual loss in Müller cell sheen dystrophy