Article Text

Abstract
Objective The NETRA (Near Eye Tool for Refractive Assessment) is a smartphone-based refractive tool that allows for self-evaluation of refractive error. This study investigates the validity of the NETRA with and without cycloplegia to non-cycloplegic subjective refractions (SR).
Methods and analysis Participants underwent NETRA measurements without cycloplegia, and again after the administration of cycloplegia (cyclopentolate hydrochloride 1%). Non-cycloplegic SR were also performed. Variation of refractive measurements in symmetric dioptric power space were investigated using stereo-pair comets, hypothesis tests for variances and means. Bland-Altman plots were applied to better understand validity of the NETRA against non-cycloplegic SR. Coefficients of repeatability and intraclass correlation coefficients were also determined.
Results The sample included 22 women (64.7%) and 12 men (35.3%); most were indigenous Africans (52.9%) with mean age and SD of 20.24±1.95 years. Variation of refractive measurements were mainly stigmatic (spherical), and variation of NETRA measurements decreased after cycloplegia. The pre-cycloplegia NETRA measurements (and their means) for the right and left eyes were more negative (myopic) in power than the post-cycloplegia NETRA measurements and means. On average, eyes were approximately 1.25 D more myopic with the NETRA without cycloplegia. With cycloplegia, NETRA results were in closer agreement with non-cycloplegic SR for the same eyes.
Conclusion NETRA validity to SR, even in the absence of cycloplegia, suggests the instrument may be useful in geographical regions where self-refractions might be potentially helpful in addressing limitations in eye and vision care.
- optics and refraction
- telemedicine
- public health
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Investigations with the NETRA (Near Eye Tool for Refractive Assessment) are limited in number and not too much is known about its validity with either non-cycloplegic or cycloplegic subjective refractions (SR). The manufacturers claim that the instrument does not necessarily require cycloplegia. Previous studies with the NETRA sometimes used methods for analysis of refractive state that were incomplete or unsatisfactory.
What are the new findings?
The NETRA with cycloplegia provides measurements that are in closer agreement to that of non-cycloplegic SR suggesting that cycloplegia would indeed be advisable and especially for younger individuals where ocular accommodation is more active. Nonetheless, even in the absence of cycloplegia, NETRA results are often in good agreement with non-cycloplegic SR.
How might these results change the focus of research or clinical practice?
With advances in the fourth industrial revolution (4IR), self-refractions and automated refractions will become increasingly important in provision of eye care and refractive compensations. This is particularly relevant in less-developed or resource-poor regions of the world. The results here may encourage further research into automated or self-refraction towards rapidly and progressively ameliorating uncompensated refractive errors and vision impairment globally.
Introduction
Scientists at the Massachusetts Institute of Technology and the company EyeNetra (USA) created the NETRA (Near Eye Tool for Refractive Assessment), a smartphone-based refractive tool that requires minimal training and which incorporates both objective and subjective refractive techniques for self-evaluation of refractive error.1 2 With the NETRA and a smartphone, the lasers and high-resolution sensors found in conventional table-mounted autorefractors are replaced by user-interaction procedures (via alignment of Vernier lines) for subjective self-refractions. Since the pixel-resolution of modern smartphone displays are closer to that of optical sensors such as Shack-Hartmann wave-front sensors, hardware applications can use smartphone screens to achieve accuracy comparable to table-mounted autorefractors.3 4
The NETRA (see figure 1A) is a binocular device with 6 D optical lenses to limit ocular accommodation prior to measurement, adjustment knobs for centration and alignment and an Android application within a high-resolution LCD smartphone.5 The NETRA creates programmable depth perception by using the smartphone display as a light source for an inverse Shack-Hartmann technique with a pinhole mask positioned over the smartphone display to negate the effects of eye-lens aberrations and to create sharp images on the retinal plane (figure 1B).1–3 5 The NETRA also makes use of the principles of Vernier acuity as an indicator of errors of focus as the maximum Vernier acuity threshold of the eye is about 5–10 times greater (more sensitive) than standard (Snellen) visual acuity. This enhances user-accuracy and the method can be applied even with low resolution devices.6 7 With the NETRA, the user aligns red and green Vernier lines oriented at various angles (figure 1Ci,Cii). and the software application (in the smartphone) computes the refractive errors for both eyes simultaneously with an inverse Shack-Hartmann wavefront sensor to measure the wave aberration function (basically the shape of the aberrated wavefront) of the eye’s optical system (figure 1D).1–3 5–7
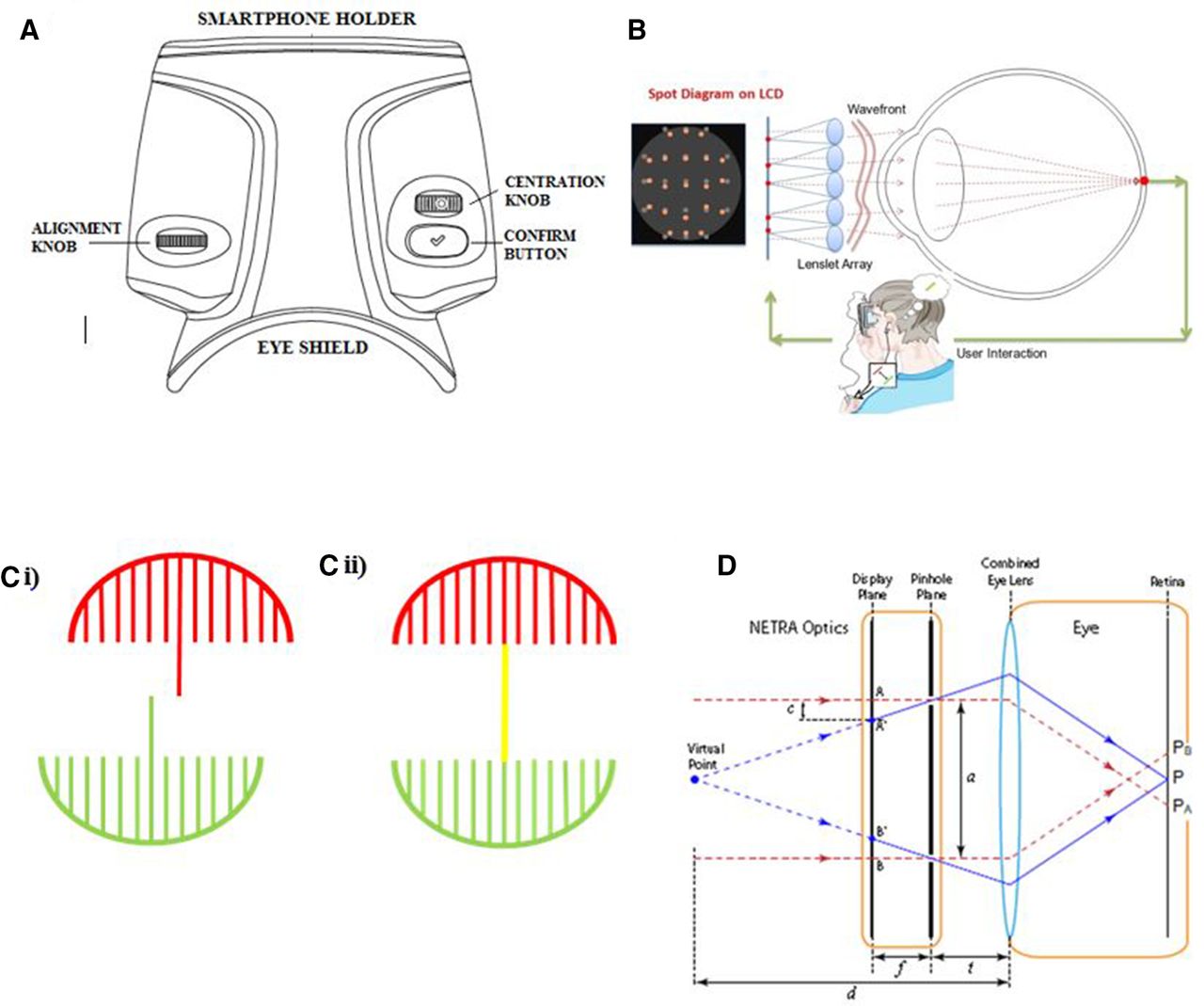
(A) The NETRA (Near Eye Tool for Refractive Assessment) device consists of a plastic-moulded binocular fixation system, with centration and alignment knobs, a confirmation of alignment button and an Android application that operates on the Samsung Galaxy S4 smartphone. The fixation system houses a microlens (pinhole) array and positive-powered optical lenses (to relax ocular accommodation) placed in front of the smartphone LCD display. In part (B), an illustration shows an inverse of the Shack-Hartmann technique whereby the NETRA replaces the sensor (in a wavefront aberrometer) with a LCD display on a smartphone and asks the subject to align Vernier lines seen on the smartphone screen. The NETRA target as seen by a user is shown in part (Ci). The interactive software displays two umbrellas on the phone screen and the handles of the umbrellas are aligned by the participant (Cii). When alignment occurs, the user confirms by pressing the appropriate button on the device. Part (D) is an illustration of the NETRA setup in a schematic eye (optical system). An emmetropic eye converges parallel rays onto point P on the retina. A myopic eye focuses light at a point before the retina, delivering two points (PA and PB) to the retina. By moving focuses A and B closer to each other on the show plane, the resulting rays focus at point P on the retina. The amount of shift required from A to Aˈ and B to Bˈ is used in the NETRA to calculate the refractive error. The quantity t is the distance from the pinhole array to the eye, while a is the spacing between the pinholes, f is the distance between the pinhole array and the LCD display plane and d is the distance of the virtual point from the eye. (Figure used with permission from Pamplona VF. Interactive Measurements and Tailored Displays for Optical Aberrations of the Human Eye. Doctoral thesis. Porto Alegre: The Federal University of Rio Grande do Sul, Brazil, 2012.).
This mobile and relatively inexpensive handheld refractive tool (NETRA) is potentially advantageous in rural eye clinics or where resources such as electricity may not be consistently available. However, previous studies3 7–14 investigating its validity to SR suggest that the NETRA lacks some degree of accuracy in determining refractive errors without the aid of cycloplegia. Thus cyclopentolate hydrochloride 1% was used here and this drug is regarded as the topical cycloplegic agent of choice in infants, children and adults since it is generally safe with a relatively rapid onset on action and is cost effective to the practitioner while producing an adequate depth of cycloplegia.15 16 In addition to these factors, this drug has a shorter recovery period as compared with more potent pharmaceutical agents such as atropine, and the concentration of 1% was adequate but safe for the purpose required with minimal side effects.17 While initial side effects of cyclopentolate hydrochloride, such as transient stinging and tearing are relatively common, cycloplegic agents can elevate IOP due to the gathering of the iris into the anterior chamber when the pupil dilates.18
Research aims
The primary aim of this study was to investigate the validity of the NETRA in measuring refractive errors with and without cycloplegia to identify its ability to provide true measures of ametropia (errors of refraction) when compared with the criterion-standard (ie, here non-cycloplegic subjective refraction (SR)). The data were analysed using appropriate multivariate statistical methods for dioptric power to provide a thorough and greater understanding of the NETRA for more effective utilisation of the procedure in both clinical and research situations.
Methods
Study design and setting
The study used a prospective observational and quantitative design in a university setting.
Participants and sampling
The research sample19 was 279 individuals of ages 9–63 years but for this specific paper a subsample was used that consisted of 34 participants of both genders and any ethnic group, but mainly undergraduate optometry students. (Results for the whole sample and for a presbyopic sample are included elsewhere19 and in other publications under preparation.) For the sample of 34 participants, 22 women (64.7%) and 12 men (35.3%) participated, and they were predominantly of indigenous African descent (52.9%). The age range was from 18 to 25 years with mean age and SD of 20.24±1.95 years, and the median age and IQR were 19±3 years. (quartile deviation=½IQR=1.5 years.) Exclusion criteria included the presence of any systemic or ocular pathology known to interfere with NETRA performance as well as any participants where the use of the cycloplegic agent might not be advisable. Since the NETRA software application computes refractive errors from ‒12 D to 5.50 D for the spherical component, and 0 D to ‒7 D for the cylindrical component, participants with refractive states outside the NETRA range were excluded from the study. Refractive states for both eyes of all participants were measured with the NETRA and with standard clinical methods for SR.
Participant involvement
Participants were not directly involved in the study design. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. Written informed consent for involvement in the study and for the use of data in research publications and presentations were obtained from all participants and were conditional that anonymity of participants was maintained.
Measurements
Non-cycloplegic SR were determined for both eyes of all participants. The NETRA was used to obtain two measurements (test and retest) per eye per participant without cycloplegia, and thereafter NETRA measurements for all eyes were obtained after the administration of the cycloplegic agent (cyclopentolate hydrochloride 1%). Depending on the degree of iris pigmentation, one or two drops (for darker irises) of cyclopentolate hydrochloride 1% were instilled 5 min apart into both eyes of each participant. Preliminary tests to assess the suitability of using the cycloplegic agent such as intraocular pressure, axial anterior chamber depth and anterior chamber angle measurements were conducted on participants prior to the instillation of the drug.
Data analyses
Measurements of refractive state in clinical notation, namely FS FC×A (or S C×A) for sphere, cylinder and axis respectively, were transformed to dioptric power matrices (Fi) and thereafter quantities such as means and variances were determined.20–31 Where applicable, power vectors32 and their coefficients M, J0 and J45 are also included for readers familiar with this notation for dioptric power. Refractive measurements were investigated using three-dimensional stereo-pair scatter plots with comets to understand the spread of the measurements as well as their agreement or similarity.
Hypothesis tests27 33 for equality of variances and covariances of the test and retest measurements for the NETRA samples, both before and after cycloplegia, were found to be statistically similar; thus, for each eye corresponding test and retest measurements were averaged for all further analyses. Hypothesis tests were also applied to understand validity of the NETRA against non-cycloplegic SR and Bland-Altman plots and confidence limits34 35 for dioptric power and indices such as coefficients of repeatability (CR) and intraclass correlation coefficients (ICC) were included.
Results
Stereo-pair scatter plots with comets
After transformation from clinical to dioptric power notation,29 refractive error (and its behaviour or variation over time) can be graphically represented using stereo-pair scatter plots where the symmetric dioptric power matrices are points in a three-dimensional (3D) Euclidean space, known as symmetric dioptric power space (SDPS).29 By plotting refractive error as points on a set of three mutually orthogonal axes in a Euclidean 3-space, a binocular and stereoscopic or three-dimensional scatter plot of SDPS is produced. To obtain the stereo-percept, the two halves of the scatter plot must be fused by allowing the eyes to converge or diverge respectively into either an eso-position or an exo-position relative to the plane of the page and stereo-pair. For stereo-pairs in this paper, an exo-posture (fixation to an imaginary point behind the plane of the paper) should be used by readers to create the 3D percept of the plots concerned. (The reverse posture can be used but then some explanations in the text might differ.) In figure 2, each data point in the stereo-pair scatter plot represents the refractive error on a set of three axes; the stigmatic (FII=MI) axis which represents stigmatic or spherical powers, the ortho-antistigmatic (FJJ=J0J) axis which is an axis of Jackson Cross Cylinders (JCC) with principal meridians being vertical (90°) and horizontal (180°), and the oblique-antistigmatic (FKK=J45K) axis, which represents JCC with principal meridians being oblique (45° and 135°). So, a single power in SDPS is represented with matrices that include a stigmatic or spherical power (matrix) and two antistigmatic (or JCC) powers (or matrices). The coefficients FI, FJ and FK are equivalent to the nomenclature M, J0 and J45 as used by Thibos et al31 and the basis matrices I, J and K are, respectively, the 2×2 identity matrix

 and
and  .
.
The word antistigmatic is a synonym for JCC and in terms of symmetric power matrices any refractive state or dioptric power is represented with a stigmatic power (a 2×2 matrix, FI) and two antistigmatic (also 2×2 matrices, FJ and Fk) or JCC powers and F=FI+FJ+Fk. So, figure 2 represents part of an infinite linear space where every point is a 2×2 matrix, Fi where the subscript i=1, 2, …, ∞.

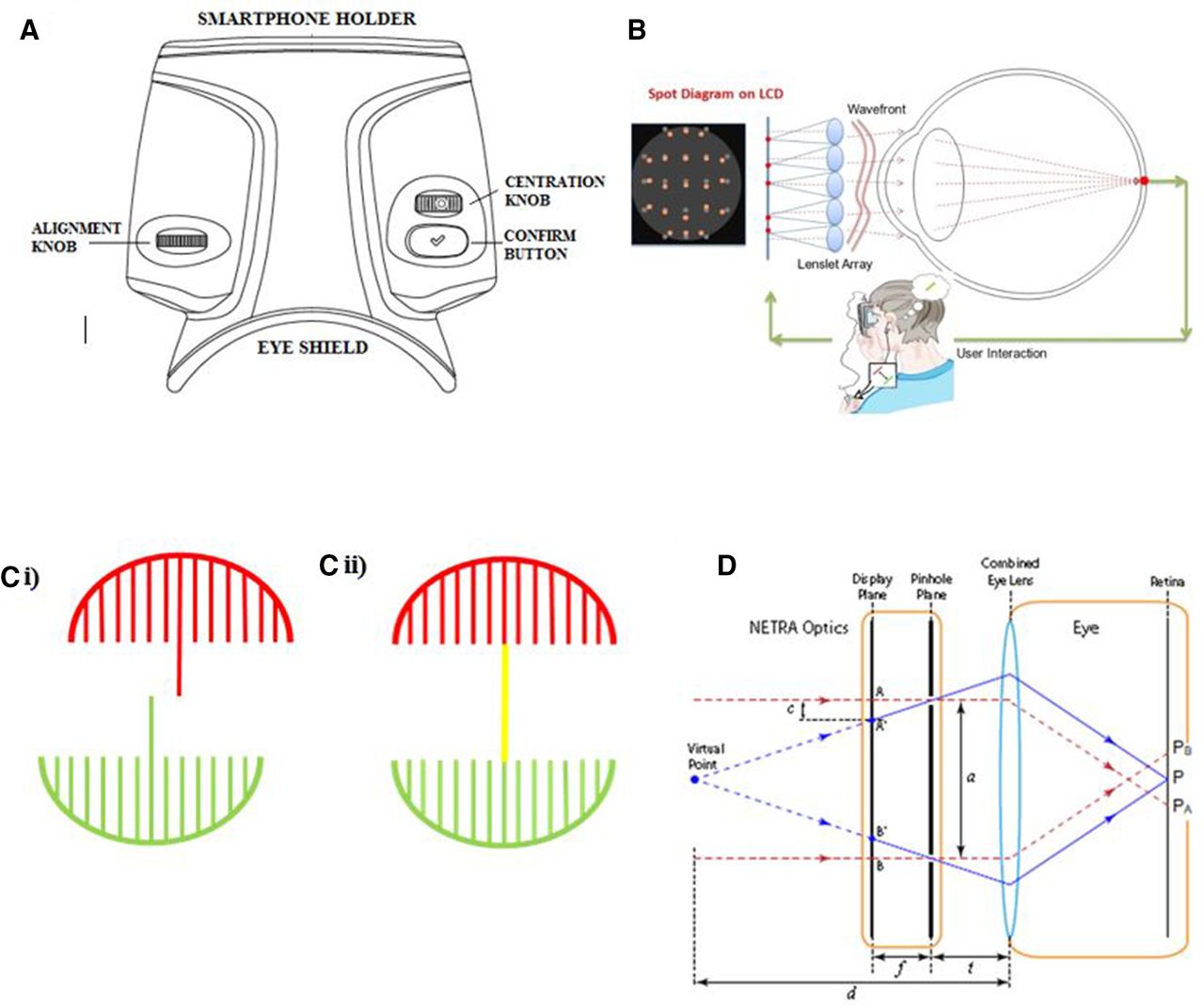
Stereo-pair scatter plots with comets for 34 participants joining non-cycloplegic subjective refraction (SR) and NETRA (Near Eye Tool for Refractive Assessment) measurements before cycloplegia (blue comets) and SR and NETRA measurements after cycloplegia (magenta comets) for 34 right (A and C) and left eyes (B and D). Each comet represents a single eye and consists of a dot and a line segment with dots representing either NETRA before or after cycloplegia and the ends of comets representing the corresponding non-cycloplegic SR. A single dot or point indicates that measurements were identical for the two methods for the eye concerned, whereas the longer the comet the greater the dissimilarity of measurements for the eye concerned. For all plots, the axis lengths in clinical terms are 7 D with 1 D tick intervals (or 7I D, 7J and 7K with tick intervals of 1I, 1J and 1K D). The origin is at O D (the 2×2 null matrix or emmetropia). Readers should allow their eyes to diverge to an imaginary point behind the page when observing each of the stereo-pairs in the figure. This results in a third plot appearing between the two halves of each stereo-pair and this central plot will have a three-dimensional appearance that is essential for properly evaluating aspects like position and direction of the comets, and hence illustrating the need for stereo-pairs.
For the three samples (non-cycloplegic SRs, NETRA before cycloplegia and the NETRA after cycloplegia), variance is mainly along the stigmatic (FII=MI) axis of the graph indicating mainly spherical variation, with most points (representing the individual measurements) clustering around the stigmatic axis and close to the origin but also spreading to some extent down the negative stigmatic (FII) axis. Table 1 contains the sample means, variances and covariances for the six samples.
The clinical means (units, D, D, °), vector notation30–32  means in dioptres (D), vector notation variances29 and covariances29 in squared dioptres (D2) for the NETRA and subjective refraction samples for the 34 right and corresponding 34 left eyes. Vector t refers to the notation of Thibos et al.31 (All vectors use superscript T to indicate the transpose.)
means in dioptres (D), vector notation variances29 and covariances29 in squared dioptres (D2) for the NETRA and subjective refraction samples for the 34 right and corresponding 34 left eyes. Vector t refers to the notation of Thibos et al.31 (All vectors use superscript T to indicate the transpose.)
In table 1, clinical means for the SR and NETRA after cycloplegia are very similar for the right and left eyes. This is less true for the situation before cycloplegia and thus, as anticipated, ocular accommodation and cycloplegia has an influence on the NETRA measurements for both the right and the left eyes. The clinical means became less myopic after cycloplegia and this affirms the hypothesis whereby accommodation is influenced by a near fixation target in instruments such as the NETRA; however once ocular accommodation is controlled with cycloplegia, the NETRA results align more closely with non-cycloplegic SR.
All samples in table 1 display mostly stigmatic or spherical variation, that is, SII is larger than the antistigmatic variances (SJJ and SKK). The covariances (SJI, SKI and SKJ) are generally small and almost zero thereby suggesting little or no linear relationships between variances for the three coefficients of power (FI, FJ and FK) involved. This is slightly less true for SJI for the NETRA after cycloplegia for the right eyes, but even there the value furthest from zero is –0.24 D2 (see the last column and covariances in parentheses in table 1 for the NETRA after cycloplegia: OD). After cycloplegia, there is a decrease in stigmatic variation (right eyes: from 4.98 to 3.36 D2; left eyes: from 5.22 to 3.77 D2) for the samples concerned.
In figure 2, stereo-pair comets for all participants (N=34) for both the right and left eyes compare the changes in refractive state between pairs of measurements per eye such as non-cycloplegic SR and NETRA before or after cycloplegia. In figure 2, most comets (blue) for the SR and NETRA before cycloplegia for both the right and left eyes are longer suggesting greater variation and dissimilarity in SR and NETRA measurements per eye concerned. The comets mostly point upwards along the stigmatic (FII) axis indicating that the measurements are more myopic for the NETRA in comparison with corresponding non-cycloplegic SR. Therefore, these comets suggest that the NETRA is sensitive to variation in ocular accommodation in these young adult participants.
The SR and NETRA after cycloplegia samples for both the right and left eyes in figure 2 (magenta comets) produce very short comets (and sometimes comets are almost single points) and although a few measurements are more dissimilar with slightly longer comets, in general, greater similarity between measurements occurs when ocular accommodation is more effectively controlled by cycloplegia.
Bland-Altman plots
The Bland-Altman plots (figures 3 and 4) for the right and left eyes of 34 participants graphically illustrate the agreement between the NETRA before cycloplegia and corresponding non-cycloplegic SR (figure 3) and the NETRA after cycloplegia and non-cycloplegic SR (figure 4). Table 2 contains the descriptive statistics for figures 3 and 4. When comparing the agreement between SR and NETRA before cycloplegia (figure 3), and SR and NETRA after cycloplegia for the right eyes (figure 4), it can be seen the mean stigmatic differences ( ) for the two samples were smaller after cycloplegia (figure 4; 0.01 D vs 1.17 D in table 2), and the 95% limits of agreement (LoA) ranges were smaller and closer to the mean stigmatic differences, that is, (-1.16; 1.14 D) versus (-2.10; 4.37 D) in table 2, suggesting variation decreased and agreement became stronger once ocular accommodation was temporarily paralysed through cycloplegia.
) for the two samples were smaller after cycloplegia (figure 4; 0.01 D vs 1.17 D in table 2), and the 95% limits of agreement (LoA) ranges were smaller and closer to the mean stigmatic differences, that is, (-1.16; 1.14 D) versus (-2.10; 4.37 D) in table 2, suggesting variation decreased and agreement became stronger once ocular accommodation was temporarily paralysed through cycloplegia.

Bland-Altman plots of means versus differences for NETRA (Near Eye Tool for Refractive Assessment) before cycloplegia and non-cycloplegic subjective refraction (SR) for 34 right (first column) and left eyes (second column). (Each eye is indicated with a black dot or marker.) Parts (A) and (B) are the Bland-Altman plots for the stigmatic (FI) coefficients, part (C) and (D) the ortho-antistigmatic (FJ) coefficients and part (E) and (F) the oblique-antistigmatic (Fk) coefficients of power, respectively, for the right and left eyes. Note the differences in scales in the different parts.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bland-Altman plots of means versus differences for NETRA (Near Eye Tool for Refractive Assessment) after cycloplegia and subjective refraction (SR) for 34 right (first column) and left eyes (second column). Parts (A) and (B) are the Bland-Altman plots for the stigmatic (FI=M) coefficients, part (C) and (D) the ortho-antistigmatic (FJ=J0) coefficients and part (E) and (F) the oblique-antistigmatic (Fk=J45) coefficients of power, respectively, for the right and left eyes. Note the differences in scales in the different parts.
Descriptive statistics for the Bland-Altman plots34 35 in figures 3 and 4 including the means  mean differences
mean differences  , SDs, SEs, 95% lower limits of agreement (LLoA), 95% upper limits of agreement (ULoA), coefficients of repeatability (CR) and intraclass correlation coefficients (ICC) for 34 right and left eyes of adults for the stigmatic (FI=M), ortho-antistigmatic (FJ=J0) and oblique-antistigmatic (Fk= J45) coefficients of power. Pearson’s correlation coefficients (r) for the means and differences and corresponding p values in parentheses are included as they are a little difficult to read in figures 3 and 4. (For significance at a 95% level, p<0.05 was applied.)
, SDs, SEs, 95% lower limits of agreement (LLoA), 95% upper limits of agreement (ULoA), coefficients of repeatability (CR) and intraclass correlation coefficients (ICC) for 34 right and left eyes of adults for the stigmatic (FI=M), ortho-antistigmatic (FJ=J0) and oblique-antistigmatic (Fk= J45) coefficients of power. Pearson’s correlation coefficients (r) for the means and differences and corresponding p values in parentheses are included as they are a little difficult to read in figures 3 and 4. (For significance at a 95% level, p<0.05 was applied.)
Possible outliers are however present for stigmatic coefficients (FI=M) of power (figure 3A,B)as a few points can be seen outside the 95% CIs34 for the upper and lower LoA. For the remaining antistigmatic coefficients of power in figures 3 and 4, most points are located relatively close the mean differences ( ) and within the 95% LoA that generally span narrow intervals, therefore, as mentioned, the variability of the differences between measurements is mostly stigmatic (spherical) and of small magnitude.
) and within the 95% LoA that generally span narrow intervals, therefore, as mentioned, the variability of the differences between measurements is mostly stigmatic (spherical) and of small magnitude.
In table 2, irrespective of laterality, CR for SR and NETRA before cycloplegia and also SR and NETRA after cycloplegia, for ortho-antistigmatic and oblique-antistigmatic coefficients were close to zero indicating that differences between measurements were minor and the antistigmatic components of the samples were repeatable and in good agreement.
The CR for the stigmatic coefficients for right and left eyes for the NETRA before cycloplegia and SR (right eyes, 3.96; left eye, 3.88) were much larger when compared with the CR for the stigmatic coefficients for the NETRA after cycloplegia and SR and the decrease in CR (right eyes, 1.14; left eyes, 1.37) suggesting that the presence of ocular accommodation may have influenced these results.
Lastly, ICC takes on values between 0 (representing unreliability) and 1 (indicating perfect reliability) and the ICC in table 2 ranged from 0.20 to 0.95 for both right and left eyes suggesting differing levels of consistency and agreement between measurements, and this could again be largely due to active ocular accommodation and possibly outliers in some instances. The ICC for the stigmatic coefficients increased (from ≈0.54 to ≈0.94) after cycloplegia indicating a stronger correlation between SR and the NETRA once ocular accommodation is better controlled.
The Bland-Altman plots also include Pearson’s correlation coefficients (and corresponding p values) for the specific means and differences. The stigmatic (parts A and B in figures 3 and 4) and ortho-antistigmatic (parts C and D in figures 3 and 4) coefficients for both right and left eyes show weak negative correlations. The oblique-antistigmatic coefficients for both eyes (E and F) show strong negative correlations between means and differences. Outliers should be considered important here in terms of understanding and interpreting these coefficients.
Hypothesis tests
Tests on variances, covariances and where necessary means were all conducted at a 95% confidence level under the assumption of normality of populations from which the samples were obtained.27 The null hypothesis (H0) implied equality of variances and covariances, or of equality of means for multiple and paired comparisons. H0 was rejected if the sample statistic exceeded the critical values. Tests of hypotheses for the equality of the variance–covariance matrices and means of paired comparisons were used to compare the NETRA before cycloplegia and non-cycloplegic SR and the NETRA after cycloplegia and non-cycloplegic SR. The null hypothesis (H0) respectively refers to equality of variances and covariances, or of mean refractive errors and was rejected if the test statistic exceeded the critical value of  =12.592 for the variances and covariances or
=12.592 for the variances and covariances or  =2.76 for means respectively. Since the variances and covariances for both comparisons (SR vs NETRA before cycloplegia and SR vs NETRA after cycloplegia) were unequal (test statistics, u=46.976 and u=30.855, respectively, for the first comparison and u=45.782 and u=31.083, respectively, for the second one) at a 95% level of confidence, all null hypotheses for equality of variances and covariances were rejected and in such cases tests for the means would not be performed as they are based on the assumption of equality of variances and covariances for the two samples under comparison.
=2.76 for means respectively. Since the variances and covariances for both comparisons (SR vs NETRA before cycloplegia and SR vs NETRA after cycloplegia) were unequal (test statistics, u=46.976 and u=30.855, respectively, for the first comparison and u=45.782 and u=31.083, respectively, for the second one) at a 95% level of confidence, all null hypotheses for equality of variances and covariances were rejected and in such cases tests for the means would not be performed as they are based on the assumption of equality of variances and covariances for the two samples under comparison.
Although visually and clinically, certain paired samples may have been similar, statistically the results did not necessarily agree. Therefore, clinical and statistical analysis needs to be done in combination to make proper deductions on agreement. Another reason for the possible rejection of the null hypothesis could be that hypothesis tests on variances and covariances are more sensitive to departures of normality,27 which occurred for all the samples concerned. Outliers in some samples may also be important and the sample sizes (N=34) were relatively small.
Discussion
Stereo-pair scatter plots with comets illustrated that the NETRA before cycloplegia samples for both right and left eyes (and their means in table 1) were more negative in power than for non-cycloplegic SR. However, the comets and their means for the NETRA after cycloplegia samples for both right and left eyes shifted closer to non-cycloplegic SR. Stereo-pair comets also showed that greater variation was found between NETRA before cycloplegia and SR affirming that ocular accommodation is influenced by a near-fixation target as in the NETRA, but as expected is better controlled with the use of a cycloplegic agent. See table 1 also for the variances and covariances where the stigmatic variances (SII) are all much larger (>3 D2) than the corresponding sample antistigmatic variances (SJJ and SKK) that are all <0.15 D2. In terms of M, J0 and J45 the variance for M is the same as that for SII and the two variances for J0 and J45 are likewise the same as for SJJ and SKK. Covariances between M, J0 and J45 similarly are the same as that for SIJ and SIK and SJK and in table 1 all the covariances were close to zero indicating the absence of linear relationships between variation in paired comparisons. Thus, variation in stigmatic power (SII=SM) is largely independent of variation in either of the antistigmatic powers. Variation in FJ and FK (or J0 and J45) are similarly not linearly related.
Bland-Altman plots, CR and ICC suggested that mainly stigmatic differences existed between the NETRA measurements before and after cycloplegia. For the right eye,  ±SD (of differences) were 1.17±1.64 D and for the left eye, 1.07±1.65 D. On average, eyes were approximately 1.25 D more myopic with the NETRA without cycloplegia. However, once ocular accommodation was temporarily paralysed with cycloplegia, the agreement between NETRA and non-cycloplegic SR became stronger, and the CR also decreased suggesting that the presence of accommodation likely influenced these results for the NETRA. Similarly, ICC for FI increased from ≈0.54 to ≈0.94 with cycloplegia. For the cycloplegic NETRA compared with SR, the
±SD (of differences) were 1.17±1.64 D and for the left eye, 1.07±1.65 D. On average, eyes were approximately 1.25 D more myopic with the NETRA without cycloplegia. However, once ocular accommodation was temporarily paralysed with cycloplegia, the agreement between NETRA and non-cycloplegic SR became stronger, and the CR also decreased suggesting that the presence of accommodation likely influenced these results for the NETRA. Similarly, ICC for FI increased from ≈0.54 to ≈0.94 with cycloplegia. For the cycloplegic NETRA compared with SR, the  for the right and left eyes are slightly different (0.01 D as compared with –0.1 D) and the presence of an outlying value (see figure 4B) could have resulted in this slight difference.
for the right and left eyes are slightly different (0.01 D as compared with –0.1 D) and the presence of an outlying value (see figure 4B) could have resulted in this slight difference.
Other studies3 7–14 comparing SR and the NETRA with and without cycloplegia found that the instrument measures cycloplegic refractions within 1 D of spherical difference from autorefraction and 0.5 D spherical difference from subjective refractions.3 This study found similar or small differences, namely 0.04 D and 0.09 D spherical equivalent differences from subjective refractions for right and left eyes, respectively. However, limitations to some of these studies included their small sample sizes as well as lack of diversity in terms of age, gender and ethnicity. Also, data from the studies treated refractive error univariately and used the nearest equivalent sphere (and sometimes less satisfactorily the spherical and cylindrical components were analysed in isolation, sometimes with cylinder axis ignored) and such methods of statistical analysis are less meaningful and less comprehensive towards understanding changes in refractive error, a quantity which is fundamentally multivariate (trivariate) in nature.
Instrument myopia occurs when a near target is viewed within an instrument (such as the NETRA and many autorefractors also) without the use of a cycloplegic, so the proximity of the perceived target stimulates proximal accommodation which leads to over-accommodation and more negative or myopic readings obtained.36–38 Sustained near visual targets can produce short-term myopic shifts in tonic accommodation.38 39 Accommodative convergence occurs in response to a stimulus of blurred vision, and proximal convergence occurs due to the awareness of the nearness of an object.39 Also, cycloplegic agents do not always completely prevent accommodation,40 41 and although cyclopentolate hydrochloride 1% generally produces adequate accommodative paralysis, residual accommodation,15 between 1 to 2.5 D could influence NETRA measurements.
According to Wang and Ciuffreda,41 depth of focus is the perceptual tolerance of the human eye to retinal defocus and blur, without incurring accommodation and depth of field is thus the projection of dioptric interval of the depth of focus. Provided the target remains within the depth of field in object space, its retinal image will remain within the depth of focus in image space and the target will be perceived as being clear and ocular accommodation will not be stimulated. It is possible that certain internal and external factors, such as luminance and pupil size may decrease a participant’s depth of focus, which in turn, might cause the NETRA target to be perceived as blurred thereby stimulating an accommodative response.
Convex positive lenses, as in the NETRA, before both eyes manipulates light to become parallel in an attempt to relax ocular accommodation. However, studies indicate that where such fogging lenses reduce visual acuity below approximately 6/30, some participants accommodation remains relaxed, while others increase accommodation.37 42 43 ,44 Also, one study indicated that sometimes (as with corrected ametropia) there was no significant change in mean accommodative response whether fogging lenses were introduced or not.43
This research supports the general application of hand-held devices to obtain measures of refractive state and recent studies19 45 using various devices based on wavefront aberrometry hold promise for self-refraction or automated refraction to address widespread unmet eye care needs in the elderly as well as others in many parts of the world.
Limitations and future directions
One limitation is that subjective refractions were not performed after the instillation of the cycloplegic agent but rather non-cycloplegic SR were determined. To avoid single-examiner bias where both non-cycloplegic SR and cycloplegic SR might be performed, only non-cycloplegic SR was used here. This decision was also made to simulate or mimic normal clinical practice where SR is more often performed without cycloplegia except where there are indications that cycloplegia might be helpful and safe. In some sense comparing the NETRA to both post-cycloplegia NETRA and non-cycloplegic SR gave indications as to how the NETRA might perform in providing possible refractive compensations (prescriptions) that might be given in usual clinical practice. However, SR after cycloplegia would have been useful and is recommended for future studies in this area.
Another limitation was the volume of the cycloplegic agent present in a clinical drop. Possible variations in drop volume per eye may have contributed to the level of cycloplegia achieved, which in turn could have had an impact on the residual accommodation present during testing. Some participants with darker irides had two drops while others had only one drop. In all cases, near point of accommodation (amplitude) were used to confirm paralysis of ocular accommodation.
The sample here was relatively small with younger participants only as ocular accommodation was an important element, but this investigation constituted part of a broader study19 with a larger sample and a greater age range where only some participants were randomly selected for this investigation with the NETRA, SR and cycloplegia. Given that the participants and their refractive states for the two methods were compared with themselves, the sample size was considered adequate for the purposes of this investigation. Larger studies, however, should be performed to further explore the influences of ocular accommodation and cycloplegia with the NETRA.
Some participants found the NETRA difficult to use although there was a brief pre-measurement training video to help them learn how to use the NETRA and its Vernier lines. It is also possible that there were learning effects in some or all participants in terms of using the NETRA from the non-cycloplegic to cycloplegic measurements and that may have influenced the data collected. Larger samples with a randomised order for the use of cycloplegia versus the non-use of cycloplegia might be helpful to reduce the impact of this issue in future studies.
Future studies should investigate NETRA refractive changes with other cycloplegic agents and altering the number of drops could be compared with to detect possible similarities or differences in relation to the drug chosen and dosage. Also, studies with some of the analytical methodology herein could include several examiners to investigate inter-reliability measurements for clinical refractive methods such as SR. Finally, diurnal variation with the NETRA and SR might be another rewarding topic for future investigation.
Conclusion
Clinically, the NETRA tends to over-minus refractions by approximately 1.25 D spherical difference from subjective refractions3 7–12 and this study also supports this finding. However, after cycloplegia, the NETRA sample produced similar results to the criterion-standard (non-cycloplegic SR). Thus, where ocular accommodation is well controlled with the use of a cycloplegic agent, NETRA results for refractive state will be similar to that for methods using distance targets such as SR. Thus, NETRA and SR validity is good even in the absence of cycloplegia but is improved with cycloplegia that mainly reduces spherical or stigmatic variance. The NETRA is a promising instrument for determination of refractive state through self-refraction and could play an important role towards improving overall access to eye care and avoiding unnecessary vision impairment due to uncompensated refractive state and especially so in less-developed regions of the world where ophthalmic professionals are sometimes unavailable or limited in numbers and where other concerns (such as affordability of eye care services and compensatory devices such as spectacles or contact lenses) may also be relevant.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study conformed to the tenets of the 2013 Declaration of Helsinki and was approved (HDC01-57-2016 and REC01-184-2016) by the Higher Degrees and Ethics Committees of the Faculty of Health Sciences, University of Johannesburg, South Africa.
Acknowledgments
To the participants who kindly provided their time during the data collection.
References
Footnotes
Twitter @nabzicakes
Contributors Conception and design: NH and AR. Data acquisition: NH. Analysis and interpretation: NH and AR. Writing: NH wrote and revised the initial manuscript as part of research towards her doctoral thesis with supervision by AR. Critical review, revisions and approval of the final manuscript for publication: AR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer We hereby declare that the views expressed in the submitted article are our own and not an official position of the institution.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.