Article Text

Abstract
Objective To determine the characteristics of children who were likely to progress rapidly and gain the greatest benefit from orthokeratology (ortho-k) treatment.
Methods and analysis The files of 113 children who participated in two myopia control studies and wore either ortho-k lenses (n=62) or single-vision spectacles (SVS) (n=51) were reviewed. Baseline cycloplegic subjective refraction, central corneal thickness, axial length, keratometry, intraocular pressure, corneal biomechanical properties and 24-month axial length data were retrieved and analysed.
Results Multivariate analysis showed that there was significant negative correlation between axial elongation and baseline age and corneal hysteresis (p<0.05) in the SVS group. In the ortho-k group, only baseline age was significantly and negatively associated with axial elongation (p<0.01).
Conclusion Corneal biomechanical properties and baseline age can predict the rate of axial elongation in myopic children. It may be beneficial for younger myopic children with low corneal hysteresis to commence ortho-k treatment as early as possible.
- myopia
- cornea
- orthokeratology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
Corneal biomechanical properties are related to axial length.
From the results of cross-sectional studies, lower corneal hysteresis is associated with longer axial length.
What are the new findings?
In our retrospective study, a negative correlation between axial elongation and baseline corneal hysteresis (CH) was revealed in single-vision spectacle (SVS) group.
A significant difference in corneal biomechanical properties was observed between slow and fast progressing subgroups in the SVS group, suggesting lower CH and corneal resistant factor may be a risk factor for axial elongation.
How might these results change the focus of research or clinical practice?
Corneal biomechanical properties could be used as a screening parameter to identify fast progressors, who may gain the greatest benefit from orthokeratology treatment.
Introduction
Myopia is of particular concern due to its dramatic increase in prevalence worldwide.1 In Hong Kong, a study investigating myopia prevalence among 2883 primary schoolchildren between late 2005 and early 2010 reported that the prevalence of myopia was 18.3% and 61.5% at age 6 and 12, respectively, and that the prevalence of myopia higher than −6.00 D was 1.8%.2 The prevalence was much higher than the 9% reported at age 7–8 a decade ago.3 Flitcroft suggested that the relatively low incidence of myopia at or before 6 years of age compared with that of older children was due to a secondary failure of the emmetropisation mechanisms.4
The association of ocular diseases with myopia is well recognised, with the OR of glaucoma increasing from 2.3 for low myopia to 3.3 for moderate-to-high myopia (≥−3.00 D).5 A meta-analysis of seven cross-sectional studies and one case–control study showed that myopia was associated with both nuclear and posterior subcapsular cataracts.6 A study in Singapore reported strong association between myopia >−6.00 D and retinal changes, for example, staphyloma, chorioretinal atrophy and temporal peripapillary atrophy.7
Since myopia can increase lifetime risk of ocular disease, which may lead to blindness, many studies have been conducted to investigate interventions to control myopia progression, one of which is orthokeratology (ortho-k). Ortho-k has been shown to be effective in slowing axial elongation (AE) by 36%–63% compared with subjects wearing single-vision spectacles (SVS).8–14 The variation in the level of myopia control reported by various studies may be attributable to differences in ages and refraction of the subjects recruited, resulting in differences in baseline characteristics. Mutti et al 15 investigated the differences in characteristics between children who remained emmetropic and those who later developed myopia and suggested that longer axial length (AL), higher negative refractive error and higher relative hyperopic peripheral refractive error were associated with a faster rate of myopia progression.
Corneal biomechanical properties may also influence myopia progression. Roberts et al 16 studied differences in corneal biomechanical properties between myopic and hyperopic eyes and reported there was a significant difference in corneal hysteresis (CH), corneal resistance factor (CRF) and several parameters derived from the waveform signal. CH and CRF are specific outputs from the Ocular Response Analyzer (ORA; Reichert Ophthalmic Instruments, Buffalo, New York, USA). CH refers to the ability of the corneal tissue to dissipate energy, and CRF refers to an indicator of the overall resistance of the cornea.17 18 A higher CH and CRF implies a better ability to resist from deformation by pressure. Although associations between AL and corneal biomechanical properties have been reported in children and adults,19–23 to our knowledge, there are no published studies comparing the effect of ocular biomechanical properties on AE in myopic children wearing ortho-k lenses and SVS. This study aimed to address this gap and investigate the differences and association with AE in baseline age and ocular characteristics. The ocular characteristics of subjects demonstrating fast and slow progression were also compared for both the ortho-k and SVS wearers.
Methods
All the data were retrieved from two previous studies, ROMIO8 and TO-SEE.9 All control subjects were corrected by spherical SVS made of CR39 material with refractive index of 1.56 (Hong Kong Optical Lens, Hong Kong, China). All ortho-k subjects were fitted with spherical (ROMIO)8 or toric (TO-SEE)9 Menicon Z Night lenses (NKL Contactlenzen, Emmen, The Netherlands). Lens prescription was aided by a computer program provided by the lens manufacturers in both studies. Full refractive correction was provided for all subjects and the habitual prescription was updated if the monocular visual acuity was worse than 0.18 (logarithm of the minimum angle of resolution (logMAR)) (Snellen 6/9) or residual myopia/astigmatism exceeded 0.50 D at any visit after stabilisation of treatment. Measurements were repeated every 6 months for 2 years after the baseline visit. Table 1 shows a summary of the inclusion and exclusion criteria of ROMIO and TO-SEE studies.8 9
Inclusion and exclusion criteria of ROMIO and TO-SEE studies8 9
Baseline data (cycloplegic subjective refraction, central corneal thickness (CCT), AL, keratometry, intraocular pressure (IOP) and corneal biomechanical properties) and 24-month AL data were retrieved and analysed. The refractive examination was conducted according to standard clinical protocol which resulted in the maximum plus lens without detriment to the visual acuity steps. Binocular balancing with prism dissociation was also performed to ensure maximum visual acuity could be achieved. CCT and keratometry were measured using the Pentacam (V.1.12, Oculus, Arlington, Washington, USA). AL was measured with partial coherence laser interferometry (IOL Master; Carl Zeiss, Oberkochen, Germany). Goldmann-correlated intraocular pressure (IOPg), corneal compensated intraocular pressure (IOPcc) and corneal biomechanical properties were measured with the ORA (V.2.00, Reichert Ophthalmic Instruments). Valid ORA data were defined as those with a waveform score ≥4.0. The average of four valid ORA data readings was used in data analyses. To further analyse the association between AE and ocular characteristics, ocular characteristics of two subgroups (10 subjects with the fastest (control: 0.91≤AE≤ 1.15 mm ; Ortho-k: 0.58≤AE≤ 0.87 mm) and 10 subjects with the slowest (control: 0.18≤AE≤ 0.43 mm ; Ortho-k: −0.26≤AE≤ 0.07 mm) AE in each group of subjects) were compared.
Treatment of data
SPSS V.22.0 (IBM) was used to perform statistical analysis. The data from ROMIO8 and TO-SEE9 were combined since the protocol of data collection, study period and most inclusion criteria, except for high astigmatism power for TO-SEE study, was the same. The data sets followed a normal distribution (Kolmogorov-Smirnov tests, p>0.05), hence parametric tests were used for analyses. Fisher’s exact probability test was performed to test the sex difference between ortho-k and SVS groups. Other differences in the baseline characteristics between the ortho-k and SVS subjects were tested using unpaired t-tests. Since AE was significantly slower8 9 in subjects undergoing ortho-k than those wearing SVS, ortho-k and SVS groups were analysed separately. Stepwise multiple linear regression was used to analyse the effect of AE over 24 months in ortho-k and SVS groups. To identify potential differences in ocular characteristics between fast and slow progressors, subgroup analysis was also performed: one-way analysis of variance (ANOVA) (or one-way analysis of covariance (ANCOVA), where indicated) was used to compare the ocular characteristics of 10 subjects with the fastest and 10 subjects with the slowest AE over 2 years in the two groups of subjects. Except for refractive cylinder (Shapiro-Wilk tests, p<0.001), all the data from the subgroups followed normal distribution (Shapiro-Wilk tests, p>0.05). Post-hoc tests with Bonferroni correction were performed if significant differences were found.
Results
In total, 113 (ortho-k: 62, SVS: 51) of 136 (ortho-k: 72, SVS: 64) subjects had valid ORA data. Table 2 presents the initial age and ocular characteristics of these 113 subjects.
Baseline age and ocular characteristics of subjects
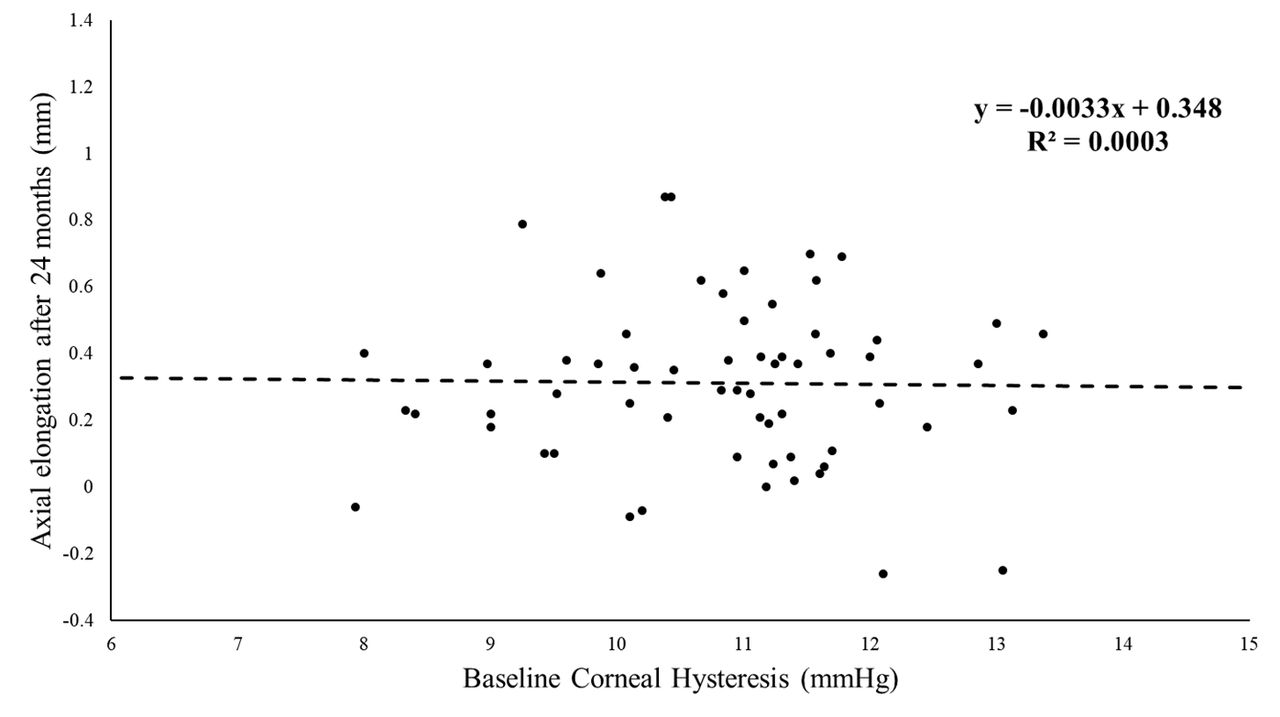
There were no significant differences in the demographic data between the two groups of subjects (p>0.05), or between males/females (unpaired t-test, p>0.05). AE over 24 months was significantly associated with initial age (adjusted R2=0.085, F1,60 = 6.672, standardised beta=−0.316, p=0.012) but not with initial AL, corneal curvature, CCT, IOPg, IOPcc, CRF or CH of the subjects in the ortho-k group (partial r: −0.240 to 0.091, p>0.05). However, in the SVS group, AE was significantly associated with initial age (standardised beta=−0.327, p=0.015) and CH (standardised beta=−0.316, p=0.018) (adjusted R2=0.236, F2,48 = 8.741, p=0.001), but not with initial AL, corneal curvature, CCT, IOPg, IOPcc or CRF (partial r: −0.191 to 0.084, p>0.05). Figure 1 and 2 present the plot of the association between CH and AE after 24 months in SVS and ortho-k group, respectively.
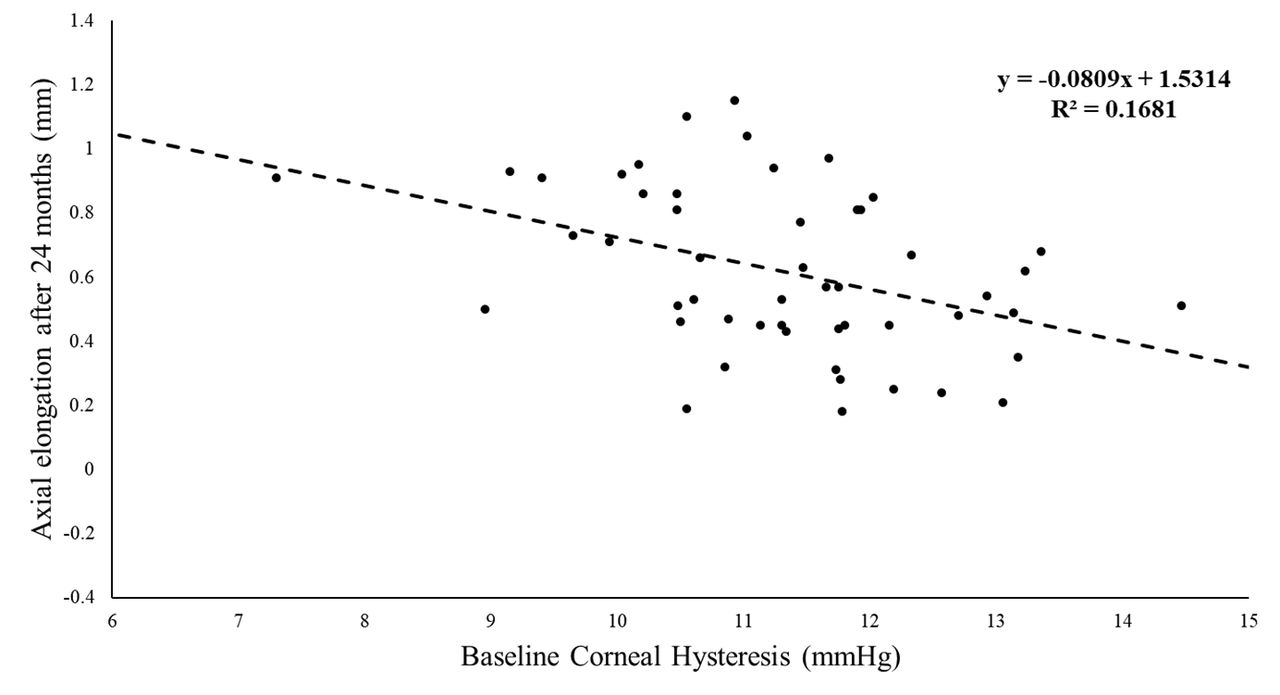
Association between corneal hysteresis and axial elongation in single-vision spectacle group (n=51).
{kind=link}
{kind=link}
Association between corneal hysteresis and axial elongation in ortho-k group (n=62).
Baseline data of the 40 subjects with the fastest and slowest AE in the two study groups are presented in table 3.
Baseline age and ocular characteristics of 10 subjects with the fastest and 10 subjects with the slowest axial elongation (AE) after 24 months of monitoring
AE differed among the four subgroups (one-way ANOVA, p<0.001). The AE was significantly lower in the ortho-k subjects compared with the SVS subjects in both subgroups (p<0.001).
There were significant differences in baseline age among the four subgroups (one-way ANOVA, p<0.05). Post-hoc tests showed that the rapid progressing subgroups were about 1.5–1.7 years younger than those in the slow progressing subgroups for both ortho-k and SVS groups (p<0.05). There was no significant difference in age between the ortho-k and SVS subjects in the fast progressing (p>0.99) and slow progressing subgroups (p>0.99). After controlling for age, there were significant differences in CH and CRF among the four subgroups (one-way ANCOVAs, p<0.05). Post-hoc tests revealed that a significant difference in CH and CRF existed between the fast and slow progressing subgroups in the SVS subjects (p<0.05), but not between the ortho-k subjects (p>0.99).
Discussion
The results of the current study showed that initial age was significantly associated with the AL elongation in both ortho-k and SVS groups. Subjects who were younger tended to progress faster than those who were older. This association has been previously reported24 and was in agreement with other reports on myopic children.25–27 Two previous studies conducted in Singapore reported that children with younger baseline age had faster myopia progression.26 27 Another study with ethnically diverse subjects also reported a similar result.25
In addition to initial age, CH was also associated with AE in the SVS group, but not in the ortho-k group. This association between AL and corneal biomechanical properties has been reported in several previous cross-sectional studies.19 21–23 28 Chang et al 22 reported that longer AL was associated with lower CH and CRF values in myopic children and there was a significant correlation between the difference of AL and CH between the two eyes of each subject. This might suggest that differences in corneal biomechanical properties may indicate generalised structural differences between eyes. Song et al 21 also demonstrated an association between AL and corneal biomechanical properties in secondary school children. Shen et al 28 investigated the corneal biomechanical properties of adults with high myopia and showed significantly lower CH. Both Del Buey et al 19 and Jiang et al 23 also reported that CH in high myopes was decreased compared with low and non-myopic subjects. However, these were cross-sectional studies and, although they showed that longer AL or higher myopia was associated with lower CH, they were not able to determine if low CH is a potential risk factor for AE. The current study suggests that in addition to initial age low CH may be a risk factor for AE in young myopic children not undergoing myopia control treatment.
Hysteresis is a physical property referred to the ability to dampen pressure changes. A lower CH value may imply a poor ability to resist the stretch in response to distending IOP stress.29 The corneal hysteresis might reflect the constitution of its extracellular matrix (ECM), which could be hypothesised to be related to the ECM composition of posterior ocular tissues.30 IOP had shown to be one mechanical factor that could lead to AE.31 32 Elevations in IOP had shown to be associated with AE of the eye.33–36 Many daily life activities including eye rubbing,37 forced eyelid closure38 and isometric exercises,39 can increase IOP within a short period of time. The relatively poor ability to resist the ocular deformation by sudden increase in IOP for subjects with low CH could be the reason to explain the negative association of CH and AE. In the ortho-k group, only initial age was associated with AE. This result is in agreement with previous studies, which reported that younger ortho-k wearers tended to progress faster.40 41 The mechanism leading to slowing down of AE by use of ortho-k is still unclear. It has been suggested that ortho-k increases myopic peripheral defocus42 which may lead to retardation of myopia progression. The amount of induced peripheral defocus varies individually, and it may not be associated with CH of individual subjects. This may help to explain why the effect of baseline CH was masked in the ortho-k group.
To further investigate the relationship between AL and ocular characteristics, baseline characteristics between 10 subjects with the fastest (fast progressor) and 10 subjects with the slowest (slow progressor) AE over 2 years in the two treatment groups were also compared. In addition to initial age, a significant difference in corneal biomechanical properties between fast and slow progressors in the SVS group was observed. CH and CRF were significantly higher in the slow progressors. The reproducibility and repeatability of the ORA were documented by published literatures in adults and children.43 44 The reported intra-examiner reliability ranged from 0.78 to 0.93 (good to excellent).43 The reported mean±SD test–retest differences of children in CH and CRF were 0.36±1.14 mm Hg and 0.18±1.04 mm Hg, respectively, in spectacle group and −0.06±0.75 and 0.06±0.77 mm Hg, respectively, in ortho-k group.44 These results showed that the 84% (mean+1 SD) of subjects would expect to exhibit retest changes of corneal biomechanical properties of <1.5 mm Hg in spectacle group and 0.83 mm Hg in ortho-k group. The mean differences of CH and CRF, between fast and slow progressors, in SVS group, which yielded statistically significance, were 1.75 and 1.91 mm Hg, respectively. In other words, on the basis of probability, such differences would more than likely represent a genuine difference rather than measurement noise.
Their initial AL, corneal curvature and CCT, which were previously reported as factors likely to affect CH and CRF measurements,45 46 were matched in this study. Age was also reported to be a factor affecting CH, and a significant difference of baseline age between the subgroups was also observed in the current study. Kida et al 47 concluded there was an inverse relationship between age and CH in adults, and noted a similar association for CRF. However, Kirwan et al 48 did not find any significant correlation between age and CH. In the current study, even after controlling for initial age, CH and CRF remained significantly lower in the fast progressors in the SVS group, but this difference was not observed in the ortho-k group. The mean AE of the fast progressors in the SVS group was 0.98 mm after 24 months. If the rate of progression remained the same, it could be predicted that these subjects would most likely suffer from moderate to high myopia in later life. In the previous reports, CH was lower in moderate to high myopia subjects.19 23 28 This result was indirectly in agreement with previous reports and provided further evidence that low CH may be a risk factor of myopia progression. The stepwise multiple linear regression model revealed that CH was associated with AE after 24 months in SVS group, but not in the ortho-k group.
From the result, patients, especially those with low CH, should benefit from commencing ortho-k treatment as early as possible, to minimise the risk of myopia progression. Further longitudinal work, with larger sample sizes, would be required to confirm the role of CH and CRF in myopia progression and to determine the cut-off of CH and CRF points in order to determine the risk of myopia progression.
Conclusion
Subjects having slower myopia progression were significantly older than those with fast progression, irrespective of their form of refractive correction (SVS or ortho-k). In addition, significant differences in CH and CRF were observed between slow and fast progressing subgroups in the SVS group, suggesting lower CH and CRF may be a risk factor for AE.
Acknowledgments
The authors thank Dr Maureen Boost for her advice in the preparation of the manuscript.
References
Footnotes
Contributors CP planned the current study. WK and CSW analysed the data and interpreted the results. WK wrote the first draft of the paper. CP, CSW, WJS and OJB reviewed the manuscript.
Funding This study was supported by the Research Residency Scheme from The School of Optometry, The Hong Kong Polytechnic University and a Collaborative Research Agreement (ZG3Z) between The Hong Kong Polytechnic University and Menicon Co Ltd., Japan, which supports a PhD student (W.K). The two previous studies were supported by a Collaborative Research Agreements between PolyU and Menicon Co Ltd., Japan (ZG13 and ZG30: ROMIO and TO-SEE studies).
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Ethics approval Both studies were approved by the Departmental Research Committee of the School of Optometry of The Hong Kong Polytechnic University and conducted in accordance with the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.