Article Text

Abstract
Aims: To assess the longitudinal changes in biometric parameters and associated factors in young myopic children aged 7–9 years followed prospectively in Singapore.
Methods: Children aged 7–9 years from three Singapore schools were invited to participate in the SCORM (Singapore Cohort study Of the Risk factors for Myopia) study. Yearly eye examinations involving biometry measures were performed in the schools. Only myopic children (n = 543) with 3 year follow up data were included in this analysis.
Results: The 3 year increases in axial length, anterior chamber depth, lens thickness, vitreous chamber depth, and corneal curvature were 0.89 mm, −0.02 mm, −0.01 mm, 0.92 mm, and 0.01 mm, respectively. Children who were younger, female, and who had a parental history of myopia were more likely to have greater increases in axial length. After adjustment for school, age, sex, race, parental myopia and reading in books per week, the age (p<0.001), sex (p = 0.012), and parental myopia (p = 0.027) remained significantly associated with the 3 year change in axial length. Reading in books per week, however, was not associated with axial length change. Children with faster rates of progression of myopia had greater increases in axial length (Pearson correlation coefficient (r) = −0.69) and vitreous chamber depth (r = −0.83).
Conclusions: The 3 year change in axial length of Singapore children aged 7–9 years at baseline was high and greater in younger children, females, and children with a parental history of myopia. Myopia progression was driven largely by vitreous chamber depth increase.
- CLEERE study, Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error study
- COMET, Correction of Myopia Evaluation Trial
- SCORM study, Singapore Cohort study Of the Risk factors for Myopia study
- axial length
- epidemiology
- biometry
- Singapore
- vitreous chamber depth
- children
- CLEERE study, Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error study
- COMET, Correction of Myopia Evaluation Trial
- SCORM study, Singapore Cohort study Of the Risk factors for Myopia study
- axial length
- epidemiology
- biometry
- Singapore
- vitreous chamber depth
- children
Statistics from Altmetric.com
- CLEERE study, Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error study
- COMET, Correction of Myopia Evaluation Trial
- SCORM study, Singapore Cohort study Of the Risk factors for Myopia study
- axial length
- epidemiology
- biometry
- Singapore
- vitreous chamber depth
- children
- CLEERE study, Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error study
- COMET, Correction of Myopia Evaluation Trial
- SCORM study, Singapore Cohort study Of the Risk factors for Myopia study
- axial length
- epidemiology
- biometry
- Singapore
- vitreous chamber depth
- children
The reported rates of myopia progression (−0.70 dioptres (D) per year in Singapore children and −0.63 D per year in Hong Kong children) among myopic children in east Asian countries are among the highest in the world.1,2 The knowledge of changes in biometric patterns in myopic children will enable a better understanding of stimuli influencing growth patterns and continued shifts in refraction. Most previous studies have evaluated biometry parameters at one point of time in cross sectional studies.3,4 Changes in biometry parameters were documented in the Correction of Myopia Evaluation Trial (COMET) of 469 children aged 6–11 years with myopia between −1.25 and −4.5 D: the increase in axial length was 0.75 mm in the single vision lens group (n = 234) over a 3 year period.5 There are few reports describing the risk factors for changes in biometric parameters, although from cross sectional analysis of 2583 school aged children in the Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) study, boys and older children had longer axial lengths.6
There are few community based or school based longitudinal data describing risk factors influencing changes in biometry parameters in myopic children. We aimed to evaluate the pattern of biometry parameter changes and associated factors in young myopic children aged 7–9 years followed prospectively for 3 years in Singapore.
METHODS
The Singapore Cohort Of the Risk factors for Myopia (SCORM) study was launched in three schools in Singapore and the methodology has been described in previous publications.1,7,8,9,10 In brief, all eligible children (n = 2819) aged 7–9 years in grades 1–3 were invited to participate. There were 1979 children who agreed to participate (participation rate = 70.2%): 665 myopic (spherical equivalent (SE) at least −0.5 dioptres) children and 1314 non-myopic children at baseline. Annual eye examinations were conducted in the schools (baseline, follow up visits 1, 2, and 3). This investigation includes those children who were myopic at baseline (n = 543) and who had 3 year follow up data. Informed written consent was obtained after the nature of the study was explained to the parents. The tenets of the Declaration of Helsinki were observed and approval from the Singapore Eye Research Institute ethics committee was granted.
Questionnaire
At baseline, information about demographic data and risk factors was obtained from a parent administered questionnaire. Parental history of myopia was determined by asking whether the parents wore contact lenses or spectacles to see far distances. Information on near work activity was obtained by asking about the number of books read per week. We also asked about the number of hours of reading per day, computer use, video use, and television watching on weekdays and weekends.
Yearly eye examinations
Contact ultrasound biometry measures were performed using one of two biometry machines (Echoscan model US-800; Nidek Co, Ltd, Tokyo, Japan; probe frequency of 10 mHz), after one drop of 0.5% oxybuprocaine (proparacaine) hydrochloride (Alcaine: Alcon-Couvreur) was administered. The average of six values was taken only if the standard deviation (SD) of the six measurements was less than 0.12 mm. If the SD of the six measurements was 0.12 mm or more, the data were not included and the measurements were repeated until SD was less than 0.12 mm. Cycloplegia was induced in each eye by the instillation of three drops of 1% cyclopentolate hydrochloride (Cyclogyl: Alcon-Couvreur) 5 minutes apart. At least 30 minutes after the last drop, five consecutive refraction and keratometry readings were obtained using one of two calibrated autokeratorefractometers (model RK5; Canon, Inc Ltd, Tochigiken, Japan).
Statistical methods
Spherical equivalent was defined as sphere plus half cylinder. Because the axial length data (Pearson correlation coefficient (r) = 0.91) from the right and left eyes were similar, only the results from the right eye were presented. The 3 year change in biometry parameters was defined as the biometry parameter at the baseline examination subtracted from the final examination among myopic children with 3 year follow up data. Multiple linear regression models were constructed with the 3 year change in biometry parameter as the dependent variable and the possible risk factors as covariates. The following interactions were evaluated: reading in books per week and parental myopia, as well as near work in hours per day and parental myopia. Repeated measures analysis of variance models were constructed with yearly change in biometry parameters or SE as the dependent variables to evaluate the time trends in biometry changes over the years. Statistical analyses were conducted using Stata version 7.0.11
RESULTS
Myopic children with 3 year follow up data (n = 543) and without follow up data for 3 years (n = 122) were similar by age (p = 0.43), sex (p = 0.25), race (p = 0.66), and baseline refraction (p = 0.96). There were 184 children aged 7 years, 159 children aged 8 years, and 200 children aged 9 years at baseline. The study consists of 285 boys and 258 girls and there were 446 Chinese, 58 Malays, and 39 Indians. The mean baseline axial length was 24.03 mm (range 20.17–27.22) and mean final axial length was 24.92 mm (range 22.33–28.21).
The increases in axial length and vitreous chamber depth were smallest in the third year of the study compared with the increases in the first and second years (both p values <0.001) (table 1). The anterior chamber depth decreases were larger at the end of the third year (p<0.001). The progression of myopia was fastest in the first year (mean = −0.88 D per year) and slowest in the third year (mean = −0.48 D per year; p<0.001). There were no significant trends in changes in lens thickness (p = 0.68) or corneal curvature (p = 0.33) over the 3 years.
Yearly changes in biometry and refractive error
The overall 3 year cumulative progression of myopia was −2.03 D. The 3 year increases in axial length, anterior chamber depth, lens thickness, vitreous chamber depth, and corneal curvature were 0.89 mm, −0.02 mm, −0.01 mm, 0.92 mm, and 0.01 mm, respectively, in myopic children aged 7–9 years (table 2). The axial length (p<0.001) and vitreous chamber depth (p<0.001) increases were less marked in children who were older at baseline. The 3 year increase in axial length (0.94 mm versus 0.85 mm; p = 0.037) and vitreous chamber depth were greater in females compared with males (0.98 mm versus 0.88 mm; p = 0.007). Although Chinese children did not have greater 3 year axial length increases (p = 0.15), the vitreous chamber depth increases were greater (0.95 mm versus 0.82 mm; p = 0.01), and the lens was more likely to become thinner (−0.01 mm versus 0.03 mm; p = 0.02), compared with non-Chinese children. The 3 year axial length increases were greatest in children with two myopic parents (0.95 mm), followed by one (0.93 mm) and no myopic parents (0.77 mm) (p for trend = 0.005). The 3 year vitreous chamber depth increases for children with two, one, and no myopic parents were 0.98 mm, 0.95 mm, and 0.82 mm, respectively (p for trend <0.001). Reading in books per week, reading in hours per day, age of onset of myopia, and baseline refractive error, however, were not significantly associated with any biometric parameter change.
Three year cumulative changes in axial length, anterior chamber depth, lens thickness, vitreous chamber depth, and corneal curvature
In the final multiple linear regression model with 3 year axial length change as the dependent variable and school, age, sex, ethnicity, parental myopia, and reading as the covariates (table 3), children aged 8 and 9 years had increases in 3 year axial length that were 0.23 mm and 0.45 mm smaller compared with 7 year old children, respectively. Females had greater 3 year axial length increases (0.11 mm) compared with males. Children with parental myopia had greater 3 year axial length increases compared with children with no parental myopia by 0.11 mm (p = 0.027), and for each increment increase in the number of myopic parents, the 3 year axial length increased by 0.05 mm, but this trend was only of borderline significance (p for trend = 0.082). In multivariate models adjusted for identical factors, 3 year vitreous chamber depth changes were also associated with age (p<0.001) and sex (p = 0.001). The 3 year vitreous chamber depth change was greater in children with one or two parents with myopia compared with no parents with myopia (p = 0.016); however, the association with the number of myopic parents (two versus one versus none) was only of borderline significance (p = 0.055). Three year change in lens thickness was associated with age (p<0.001) and race (p = 0.04) in multivariate modelling. There were no significant interactions between reading in books per week and parental myopia or near work in hours per day and parental myopia with the 3 year changes in any of the biometry parameters.
Multiple linear regression model of the factors associated with 3 year axial length change
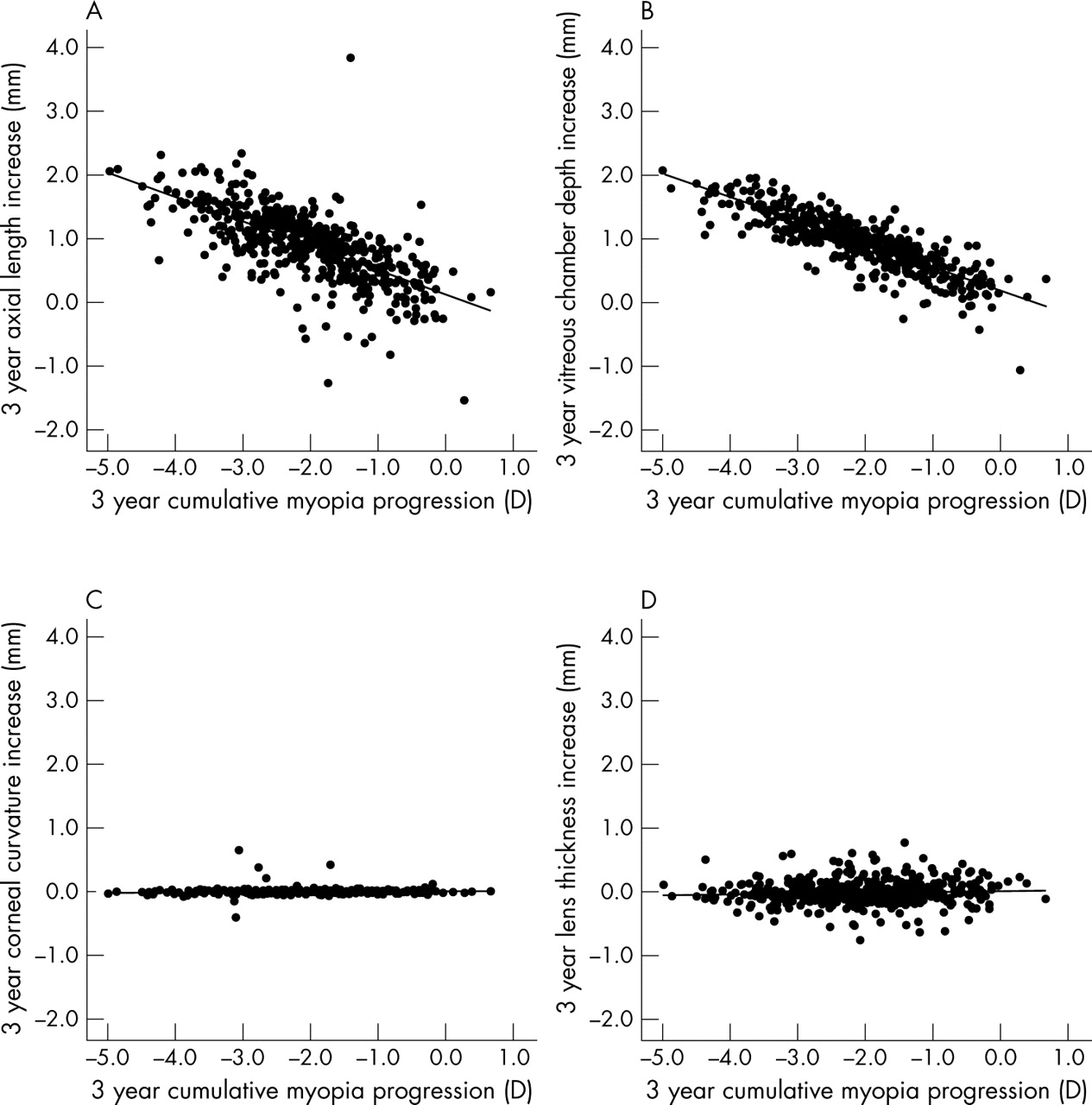
Children with faster rates of progression of myopia had greater increases in axial length (r = −0.69) and greater increases in vitreous chamber depth (r = −0.83) (fig 1). However, the rates of progression of myopia were not significantly correlated with the rates of change in corneal curvature, anterior chamber depth, or lens thickness in this myopic population.

{kind=link}
Scatter plots of the changes in the various biometry parameters and the progression of myopia. (A) Pearson r = −0.69, p = 0.001; (B) Pearson r = −0.83, p = 0.001; (C) Pearson r = 0.02, p = 0.65; (D) Pearson r = 0.06, p = 0.19.
DISCUSSION
In our study, the 3 year increases in axial length (mean = 0.89 mm) and vitreous chamber depth (0.92 mm) in Singapore children are high. In contrast, the 3 year changes in anterior chamber depth, lens thickness, and corneal curvature were minimal. Children who were young, female, and who had myopic parents were more likely to have greater axial length increases. No associations between near work activity and biometry parameter changes were found.
The 3 year increase in axial length is high (0.89 mm), but similar to the single vision lens group of a Hong Kong study of myopic children aged 7–10.5 years (n = 133) enrolled in a trial evaluating progressive lenses, who showed similar increases in axial length (0.32 mm per year = 0.96 mm over 3 years).2 In the COMET trial, the rate of increase in axial length was slightly lower in myopic children aged 6–11 years in the single vision lens group: 0.75 mm over 3 years.5 In contrast, in a university study of 149 Norwegian engineering students (mean age of 20.6 years) across the refractive error range with a mean 3 year refractive change of −0.52 D, the 3 year change in axial length was 0.34 mm.12 Differences in the refractive error range, subject age limits, interethnic composition, and overall dropout rates, however, limit the conclusions from comparing the results of these studies.
Greater changes in axial length in younger children and females parallel the greater changes in refraction in the same age and sex patterns in this Singapore cohort.1 In our study, children who had one or two parents with myopia had greater increases in axial length change compared with children without any myopic parents. In a 24 year longitudinal study of 122 US children, the odds ratio of incident myopia for two myopic parents versus none was 5.09 (95% confidence interval (CI) 1.69 to 14.49).13 Previously, most epidemiological investigations have been cross sectional in nature.14,15 A cross sectional study of adults aged 17–45 years showed that if there were one or more highly myopic parent, the odds ratios of mild (SE −1.25 to −2.5 D), moderate (SE −3.75 to −4.75 D), and high myopia (SE at least −5.0 D) were 2.5, 3.7, and >5.5, respectively.14 In the Orinda Longitudinal study of 716 children aged 6–14 years, children with two myopic parents had more myopic refractive error compared with children with one or no myopic parents (p<0.01).15 Few studies, however, have evaluated the effect of parental history, a possible marker of shared common family environment or genetic susceptibility, on biometric parameter changes.
In the Finnish children’s study, reading was significantly (p = 0.003) associated with the progression of myopia.16 To our knowledge, there are few studies that have evaluated the effects of reading on the change in axial length. Reading in books per week was not associated with greater increases in axial length in our study. The initial cross sectional analysis of SCORM data showed that children who read more and who had myopic parents had larger axial lengths.17 The lack of any significant effects of lifestyle and familial risk factors on longitudinal changes on axial length change could perhaps be attributable to the narrow age range of the population, the rather young cohort, relatively short follow up, misclassification of near work activity, or to the possibility that the role of near work differs between myopia onset and myopia progression.
The rapid progression of myopia in our study is accompanied by elongation of the eye in the axial dimension. The posterior segment changes in severely myopic eyes include the stretching of the retina and the development of optic disc crescents and other pathological changes.18 In Singapore children, corneal power appears to have a minor role in the progression of myopia, consistent with the pattern found in other longitudinal studies.19,20 In a 2 year follow up study of 142 Hong Kong children aged 6–17 years with refractive error from −7.5 to +3.5 D, the myopic shifts in refractive error were driven by increases in axial length and vitreous chamber depth.21 Contrary to our findings, the flattening of the cornea (but only in the horizontal meridian) was associated with the progression of myopia in Hong Kong children. Lens thinning does not explain the shift of refractions towards the myopic direction, and among adult clinical microscopists, this effect is also minimal.22
The advantages of our study include the relatively large sample size, the low dropout rate, and the availability of longitudinal biometry parameters in a school based cohort in a myopia endemic country. The 3 year dropout rate was 18.4% and children who withdrew from the study were not significantly different from children who did not withdraw.
In summary, the 3 year increase in axial length is high (0.89 mm). Axial length changes are greatest in the first 2 years of the study and highest in younger children, females, and children with a parental history of myopia. Children who read more were not more likely to have greater changes in biometry parameters. The rate of progression of myopia was significantly associated with changes in vitreous chamber depth.
Acknowledgments
This study is supported by the National Medical Research Council Grant NMRC/0695/2002, Singapore. The authors thank Angela Cheng, Jacqui Ong, and Sister Peck for coordinating the SCORM study. We also thank Angela Cheng for assistance in statistical analysis.
REFERENCES
Footnotes
-
Competing interests: none declared
-
Ethical approval: Approval from the Singapore Eye Research Institute ethics committee was granted.