Article Text

Abstract
Objective To conduct a systematic review to identify and critically appraise clinical practice guidelines on the assessment, diagnosis and management of childhood glaucoma.
Methods and analysis A systematic literature search of databases and professional websites for clinical practice guidelines published on eye conditions between 2010 and April 2020 in English was conducted. Identified guidelines were screened for relevance to childhood glaucoma and exclusion criteria applied. Guidelines that passed the screening and quality appraisal with the Appraisal of Guidelines for Research and Evaluation II (AGREE II) tool and, if they achieved a mean score of ≥45 and ≥3 on subsets of 9 and 5 AGREE II items, respectively, were selected for inclusion and data extracted using a standardised form.
Results Following screening and critical appraisal, three guidelines were included for data extraction. None of the three guidelines was specifically developed for childhood glaucoma. A consistent recommendation was that children should undergo some form of eye screening examination or a comprehensive eye assessment to detect paediatric eye disease. Children at high risk of childhood glaucoma should undergo additional screening. One clinical practice guideline recommended interventions for childhood glaucoma consisting of tube surgery and topical beta-blockers or carbonic anhydrase inhibitors. Recommended interventions for childhood glaucoma were based on low-quality to moderate-quality evidence or expert opinion.
Conclusion Based on our selection criteria, we did not identify any high-quality clinical practice guidelines specifically targeted at childhood glaucoma. This is compounded by the lack of high-quality evidence on childhood glaucoma.
- glaucoma
- child health (paediatrics)
Data availability statement
Data are available on reasonable request. Templates and data used in this study are available upon reasonable request to the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Childhood glaucoma is a rare, but devastating, eye condition among children, which requires often lifelong management and treatment.
What are the new findings?
Clinical practice guidelines specifically targeting childhood glaucoma are scarce.
This systematic review identified only three guidelines, none of which was specific to childhood glaucoma.
How might these results change the focus of research or clinical practice?
This systematic review will inform a Package of Eye Care Interventions developed by WHO.
There is need for a high-quality clinical practice guideline for childhood glaucoma.
Introduction
Childhood glaucoma is a rare eye condition with estimated incidence of 2.29 per 100 000 people below 20 years of age in the USA to 5.41 per 100 000 live births in the UK.1 2 A higher incidence has been reported in Asian populations.1 3–5 Childhood glaucoma is an important cause of vision loss and is estimated to be responsible for 10% and 3% of childhood blindness in African regions and the USA, respectively.6 Childhood glaucoma is not a single disease entity and may arise secondary to one or more underlying congenital anatomical defects, genetic alterations, neoplastic, infectious, inflammatory or postsurgical causes. The Childhood Glaucoma Research Network defines childhood glaucoma as intraocular pressure (IOP)-related ocular damage and classifies it into primary and secondary types.7 Primary childhood glaucoma includes primary congenital glaucoma (PCG) and juvenile open angle glaucoma. Secondary childhood glaucoma includes glaucoma associated with non-acquired ocular anomalies (eg, Axenfeld Rieger anomaly), non-acquired systemic diseases (eg, Down syndrome), acquired conditions (eg, uveitis) and previous cataract surgery.7
Despite several available options for management of childhood glaucoma, the prognosis is often suboptimal. People with childhood glaucoma have a reduced quality of life8 and visual acuity is often poor with approximately 25% of children with PCG meeting the WHO’s definition of blindness in one Indian cohort.9 10 As the disease and its management essentially requires lifelong monitoring, there is also a significant impact on the caregiver quality of life, indicating that evidence-based interventions are required at a multitude of levels to optimise patient outcomes.11
Childhood glaucoma has been identified as a priority eye condition for inclusion in the WHO’s Package of Eye Care Interventions (PECI). The PECI is being developed in response to a recommendation from the World Report on Vision to imbed eye care into Universal Healthcare Coverage. The PECI will be an evidence-based tool that aims to improve access to, and the provision of, eye care by assisting Member States, particularly low-income and middle-income nations, with the planning, budgeting and integration of eye care interventions.12 For example, in the context of childhood glaucoma, the PECI will provide recommendations on cost-effective, evidence-based interventions and the resources required to implement these interventions. Stage 2 of the PECI is a systematic review of clinical practice guidelines (CPGs) to identify recommended, evidence-based interventions for priority eye conditions. Later stages of the PECI development include the review and selection of recommended interventions for inclusion in the PECI by a panel of experts from low-resource, middle-resource and high-resource settings, identification of required resources and peer review of the package.12
This systematic literature review aims to identify CPGs for childhood glaucoma and extract data to support the development of the WHO PECI.
Methods
This systematic review of CPGs was conducted in compliance with the methodology outlined in the introductory PECI paper.12 A CPG was defined according to the Institute of Medicine definition: ‘statements that include recommendations, intended to optimise patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options’.13 Exclusion criteria for each stage of screening are provided in table 1.
Exclusion criteria for screening of CPGs
Systematic literature search
A systematic literature search for CPGs was conducted on 9 March 2020 in the following academic databases: MEDLINE, Embase, CINAHL and Global Index Medicus. In addition, a search of guideline databases and the websites of several optometry and ophthalmology associations were also undertaken for CPGs that met the inclusion criteria. The search terms and filters were adapted according to the search options in the specific guideline databases and websites. Guidelines were limited to publication in the last 10 years and published in English. The full search strategy and list of databases and websites searched are presented in online supplemental appendix 1.
Supplemental material
Title and abstract screening
Title and abstracts of the records identified in the searches were screened independently by two authors (GL, SS) using the semi-automated AbstrackR software.14 The following exclusion criteria were applied: the document was not a CPG, the guideline was not published in the last 10 years, the guideline was not in English or the guideline was not developed for a priority eye condition for PECI. Discrepancies were resolved by a representative from WHO (SK) and Cochrane Eyes and Vision (CEV; JRE).
Full-text screening
CPGs identified as potentially relevant to childhood glaucoma based on title and abstract screening underwent independent full-text screening by two authors (GL, ST). Broadly, guideline relevant to paediatric populations, glaucoma or some combination of the two were selected for full-text screening and we opted to be inclusive to avoid missing eligible guidelines. CPGs were excluded if they were deemed not relevant to childhood glaucoma, did not list the affiliations of all authors, did not declare potential conflicts of interest or there were significant conflicts of interest present. Potentially significant conflicts of interest included scenarios such as a large proportion of authors having relevant conflicts of interest, the first or senior author having a direct, proprietary conflict of interest or a lack of a description for managing relevant conflicts of interest, when present. Where it was unclear whether there was a significant conflict of interest, the full-text screening team was encouraged to consult with a third (SK) and fourth author (JRE) from WHO and CEV, respectively. Other discrepancies were resolved through discussion between the two authors (GL and ST) or, in the event a consensus could not be reached, by discussion with the aforementioned third and fourth authors (SK and JRE).
Quality appraisal
The selected CPGs underwent independent quality appraisal by two authors (GL, ST) using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) tool.15 The AGREE II tool contains 23 items relating to 6 quality domains: scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability and editorial independence. Based on a consensus finding process prior to this review,16 we only used a subset of AGREE II items to appraise CPGs, specifically items 4, 7, 8, 10, 12, 13, 15, 22 and 23 (item names provided in table 2). These items are in the domains of stakeholder involvement, rigour of development, clarity of presentation and editorial independence and were recommended for use by the WHO Guideline Review Committee Secretariat, as they were deemed most relevant to the development of packages of care. To be eligible for inclusion, the average result for items 4, 7, 8, 12 and 22 had to be ≥3, and the average sum score of items 4, 7, 8, 10, 12, 13, 15, 22 and 23 had to be >45.
Details and AGREE II ratings of clinical practice guidelines that met eligibility criteria
Final guideline selection
To facilitate timely development of the PECI, a maximum of five CPGs were able to be selected for data extraction. Where more than five CPGs were eligible, guidelines were to be selected according to the following criteria: quality, publication date and comprehensiveness (ie, applicability to different settings).
Data extraction
Data were extracted from the selected CPGs using a standardised form that recorded information on the recommendation (type of recommendation, dosage, target group, etc), the strength of recommendation and the quality of the evidence used to inform the recommendation by the guideline development group. Data were tabulated and organised according to intervention type: screening, assessment, prevention, promotion or treatment.
Recommended eye care interventions for childhood glaucoma were extracted from CPGs by one author (GL or ST) and independently checked by a second author (GL or ST). The process was repeated for all the guidelines until agreement on the recommended eye care interventions was reached.
Results
Screening, appraisal and selection of guidelines
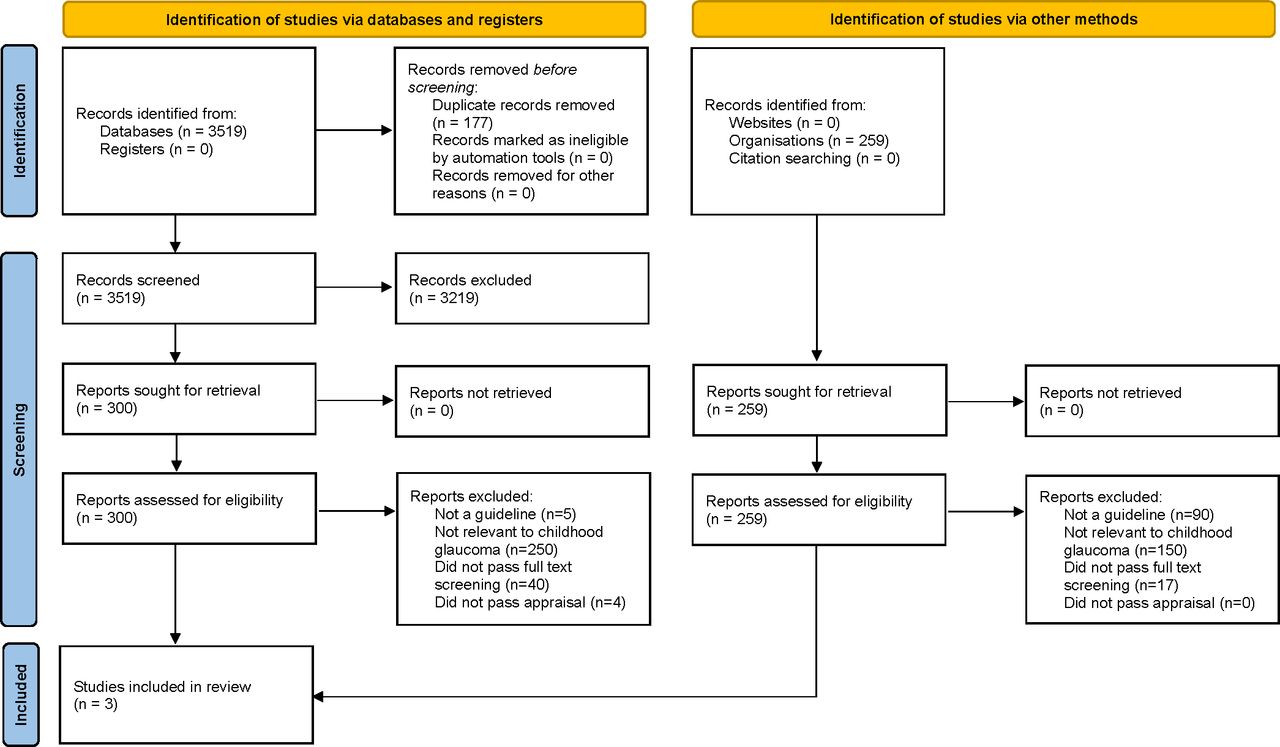
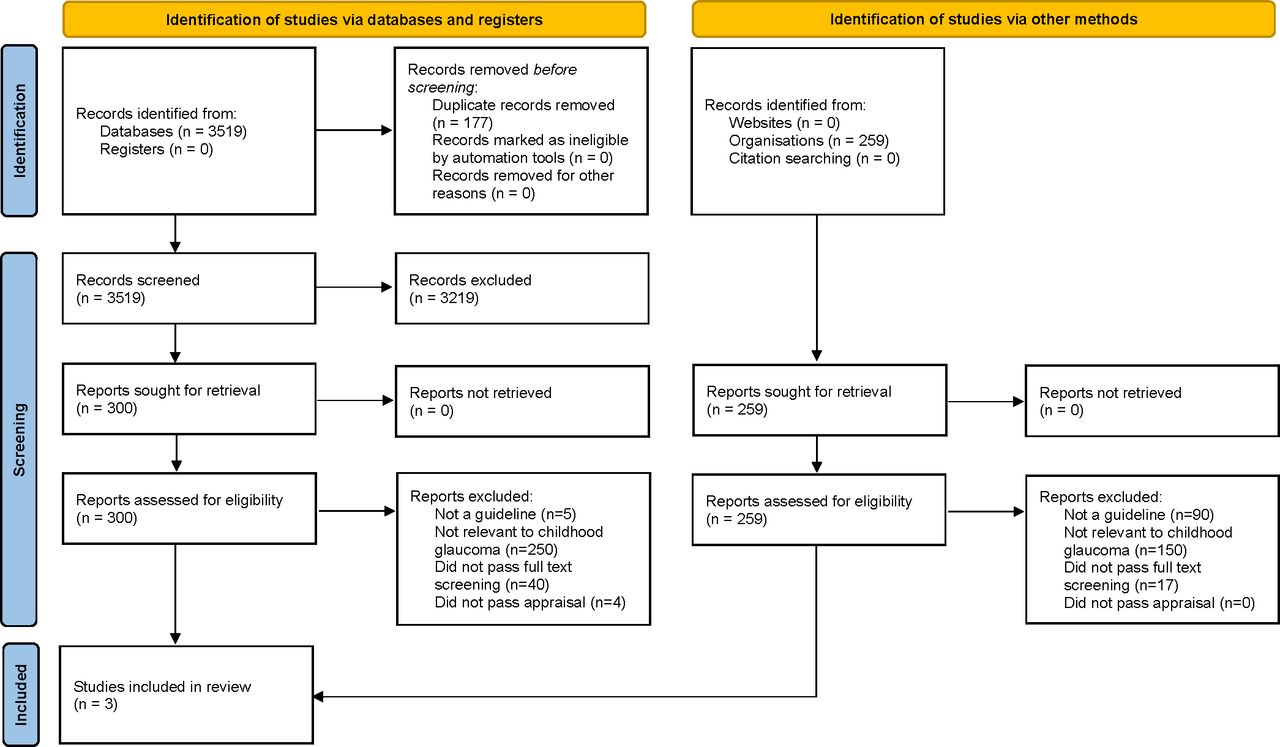
The results of the selection process are reported in figure 1. After the initial title and abstract screening, 68 reports were identified as potentially relevant to childhood glaucoma. On review of the full-text report, 29 of these guidelines were deemed not relevant to childhood glaucoma, 27 did not report either potential conflicts of interest or affiliations of authors, 1 had significant conflicts of interest among authors and 5 did not meet the criteria of a CPG on full-text review, leaving 6 CPGs for the AGREE II appraisal.
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart summarising the results of the literature review to identify clinical practice guidelines for childhood glaucoma.
The results of the AGREE II appraisal are shown in table 2. There was very good overall agreement between the two raters (one-way intraclass correlation=0.83). After the AGREE II appraisal, three of the six CPGs were excluded: one due to the average score of the two researchers for items 4, 7, 8, 12 or 22 being <3 and two CPGs were excluded due to the sum of the average score of the two researchers for all items being <45. Of the three CPGs that were excluded during the AGREE II appraisal, one was aimed at addressing the side effects of glaucoma therapy while the remaining two were CPGs aimed at all types of glaucoma. These excluded guidelines performed most poorly in areas relating to reporting of systematic review methods and methods for formulating recommendations.
We ultimately selected three CPGs17–19 for the data extraction phase. The extracted recommendations are shown in table 3. Two of the three included guidelines were published in the USA and related to the ocular assessment of children and infants and thus were not directly aimed at detection and management of childhood glaucoma. These two CPGs had the highest overall AGREE II scores. The remaining selected CPG was published in Australia in 2010 and was aimed at diagnosis and management of glaucoma at all ages and only a small part of the CPG was dedicated to childhood glaucoma. Therefore, we did not identify a CPG that specifically targeted childhood glaucoma.
Extracted assessment or intervention recommendations from eligible CPGs
Guideline recommendations
Of the recommendations extracted, strongly recommended interventions largely related to the assessment of infants and children to detect eye conditions such as childhood glaucoma, as well as the assessment of IOP in the diagnosis and management of glaucoma. Screening of first-degree relatives of those with glaucoma, including those with genetic syndromes that are highly associated with childhood glaucoma, was also strongly recommended.
Tube surgery was strongly recommended for long-term IOP control in patients at high risk of trabeculectomy failure (such as in childhood glaucoma) and in glaucoma following cataract surgery. Although not formally recommended, tube surgery was noted to be an appropriate first-line treatment for some secondary causes of childhood glaucoma. Topical beta-blockers and carbonic anhydrase inhibitors were recommended with intermediate strength for the management of childhood glaucoma, although these therapies should be used with caution due to the potential for adverse events and the quality of evidence was noted to be low. Surveillance of patients on long-term steroid medication including assessment of the optic nerve head, anterior chamber and visual field was recommended with weak or intermediate strength. These recommendations, however, were targeted at all individuals with glaucoma or at risk of glaucoma and were not specific to childhood glaucoma.
The quality of evidence used for formulating recommendations varied considerably. Recommendations relating to the screening or examination of children to detect paediatric eye disease or certain ocular assessments for the diagnosis of glaucoma were generally of moderate-quality or good-quality evidence, with some exceptions. There was only low-quality evidence to support the use of topical IOP-lowering medication for the treatment of childhood glaucoma. Interestingly there was deemed to be moderate-quality evidence for the use of tube surgery; however, this recommendation was for the use of tube surgery where trabeculectomy is likely to fail including, but not limited to, some childhood glaucomas.17 Thus, this recommendation could also be based on evidence of the effectiveness of tube surgery in adult populations.
Discussion
The findings of this systematic review demonstrate that there is a lack of high-quality CPGs aimed at childhood glaucoma. The evidence to formulate recommendations for childhood glaucoma varied substantially, with recommendations related to interventions for the treatment of childhood glaucoma generally of lower-quality evidence compared with recommendations for assessments to detect childhood glaucoma (and other paediatric eye disease). In 2013, The World Glaucoma Association (WGA) formulated consensus guidelines that define childhood glaucoma and bring a more uniform set of terminology to the childhood glaucoma landscape.7 While extremely valuable for the field, the WGA consensus document did not pass the PECI inclusion criteria as no formal systematic review was conducted. Our review indicates much work still needs to be done to develop strong evidence to inform the development of CPGs.
The number of randomised controlled trials (RCTs) for childhood glaucoma has seen only a marginal increase in the last decade. A recent Cochrane review identified 16 RCTs or quasi-RCTs comparing various surgical interventions for PCG; however, these studies variously compared 9 different surgical interventions and generally had low sample size, making it difficult to draw definite conclusions.20 It is also important to address the lack of long-term data on the outcomes of these interventions as childhood glaucoma has potentially lifelong consequences. Measurement of quality of life metrics in future studies with a medium-term to long-term follow-up would be of use.
The results of this review indicate that there is a consensus on the need for children to have an eye examination, conducted by either an eye care professional or as part of a screening programme, to detect paediatric eye diseases. However, these recommendations were not specifically targeted at childhood glaucoma. Limited long-term trends have shown that screening programmes such as the retinopathy of prematurity programme, now mandatory in several countries, may reduce the burden of disease and potential blindness.21 22 As childhood glaucoma can constitute a multitude of ocular and systemic conditions, early examination of asymptomatic children in the population could potentially increase the chances of early detection and management of these conditions. However, the low incidence of childhood glaucoma means that many children would need to be examined (approximately 20 000–33 000) to detect a single case of childhood glaucoma and, from a public health perspective, the costs may not outweigh the benefits. A potential alternative to lower the cost and optimise delivery of these annual screenings would be to combine these visits with vaccination programmes or other currently implemented programmes.23 It is also important to consider who will perform childhood eye screening or assessments. The two guidelines on paediatric eye evaluations from the USA recommends that primary care providers perform a basic eye screen of newborns and infants,18 24 whereas it may be more appropriate for children at high risk of childhood glaucoma to be examined by an ophthalmologist in a secondary or tertiary care setting.
Tube surgery was strongly recommended by the Australian CPG for long-term IOP control of all glaucoma, including some childhood glaucomas. The remaining recommendations for management of childhood glaucoma made in this CPG were of weak or intermediate strength and generally had only low-quality evidence or were based on expert opinion. Furthermore, this Australian CPG was published 10 years ago and, based on the exclusion criteria for this review, is nearly out-of-date. Some recent evidence indicates that the IOP-lowering response to antiglaucoma drugs is often lower in children and thus surgical management is necessary.18 It is also important to note that serious side effects can occur in children due to difference in drug pharmacodynamics and pharmacokinetics in children as compared with adults. Use of low-dose preparations, gel-based formulations, punctal occlusion during administration and frequent follow-ups can improve outcomes.25 Notable interventions for which formal recommendations (for or against) were not made include trabeculotomy, goniotomy and topical brimonidine eye drops. These interventions were briefly and informally discussed within the Australian guidelines, but as no formal recommendation was made, did not meet the criteria for data extraction. The Australian guideline informally recommended against the use of alpha-2 agonists, such as brimonidine, in children <7 years of age due to side effects and informally suggested goniotomy or trabeculotomy as potential interventions for PCG. The absence of a formal recommendation for trabeculotomy or goniotomy may reflect uncertainty in the evidence for these interventions at the time, despite their current widespread use in clinical practice and recommended use for PCG in the WGA consensus guidelines.7
Childhood glaucoma is a rare, but devastating, disease. There is generally a lack of high-quality evidence to inform the management of childhood glaucoma and there are few recent, targeted CPGs. CPGs are uniquely situated to be able to combine evidence from a systematic search of the scientific literature and the opinion and experience of experts in the field. The latter is particularly important in childhood glaucoma, where the evidence is relatively sparse. The WGA consensus guidelines were an important step in providing guidance on the best-practice management of childhood glaucoma. However, there is need for a high-quality CPG, incorporating both expert consensus and a systematic search of the literature. Limitations to this study include the inclusion of only CGPs written in English in the last 10 years, which have limited the CGPs identified.
Conclusion
We identified three high-quality CPGs relevant to childhood glaucoma in this systematic review; however, none was specifically targeted at childhood glaucoma. There is a considerable lack of evidence-based guidelines to direct management of childhood glaucoma. A coordinated effort is needed to address this lack of quality data with standardised disease terminology and management strategies to improve outcomes for children with childhood glaucoma.
Data availability statement
Data are available on reasonable request. Templates and data used in this study are available upon reasonable request to the authors.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
GL and ST are joint first authors.
Correction notice This article has been corrected since it first published. Author 'Sare Safi' affiliation has been updated.
Contributors IG conducted the initial literature search. GL and SS conducted title and abstract screening. GL and ST conducted full-text screening, quality appraisal and data extraction. SK and JRE were involved in the conception and design of the study. All authors critically reviewed the manuscript and approved its submission. GL acts as guarantor for the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.