Article Text

Abstract
Objectives Biologics are rapidly emerging as an effective vision saving addition to systemic uveitis therapy. The aim of this multicentre retrospective study is to review the outcomes of a large group of patients treated with adalimumab.
Methods A retrospective chart review of patients with refractory non-infectious, active uveitis treated with adalimumab was conducted. The main outcome measures were ability to reduce prednisolone dose, ability to control uveitis, final visual acuity and time to treatment failure.
Results Forty-six patients with uveitis, treated with adalimumab were included in the study. The most common anatomical uveitis phenotype was panuveitis (n=17, 37.0%). The most common diagnosis was idiopathic uveitis (n=19, 41.3%). At their latest review (mean: 4.46 years; median 4.40 years), 35 (76.1%) patients were able to discontinue corticosteroids, 11 (23.9%) patients were able to taper to <7.5 mg/day and only 1 (2.2%) patient required 10 mg of prednisone. The mean visual acuity at the latest follow-up of the worse eye was logarithm of the minimum angle of resolution (logMAR) 0.42 (SD 0.72), while the mean visual acuity of the better eye was logMAR 0.19 (SD 0.34). Of the 89 eyes, 21 (23.6%) eyes improved by at least 2 lines, 5 eyes (5.6%) deteriorated by ≥2 lines while vision was unchanged in the remaining 63 (70.8%) eyes. The time to recurrence was 1 in 12.47 person-years for adalimumab, with a 17.4% (8 patient) relapse rate. There were no serious adverse events.
Conclusions This study highlights the efficacy of adalimumab in patients with vision-threatening non-infectious uveitis, preserving vision and allowing reduction of corticosteroid dose.
- vision
- inflammation
- immunology
- drugs
Data availability statement
Data are available on reasonable request. All clinical data can be found in the record sections of Sydney Eye Hospital, St. Vincent’s Hospital Sydney and Royal Hobart Hospital.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Adalimumab has been used to treat severe or recalcitrant uveitis with good outcomes. The VISUAL 1, 2 and 3 studies provided evidence for the safety and efficacy of adalimumab over corticosteroid therapy, in patients with non-anterior, non-infectious uveitis.
What are the new findings?
This study provides real-world clinical data supporting the treatment efficacy and safety of adalimumab for the treatment of patients with severe vision-threatening uveitis. Important findings from this study include: the number of relapses was reduced; the number of patients losing vision was reduced with stable or improved vision in the long term in the majority of patients; prednisolone was ceased or reduced to safe levels in most patients and there was a decreased use of additional immunosuppressive drugs. There was a non-statistically trend towards the early introduction of adalimumab, increasing the time to uveitis relapse.
How might these results change the focus of research or clinical practice?
This study highlights the effectiveness of adalimumab in sight-threatening non-infectious uveitis and suggests benefit in early commencement of biological therapy. Based on the data in this study, adding adalimumab therapy allows reduction of corticosteroid dose to a safe dose (<7.5 mg) or to cease corticosteroids; the use of second-line conventional immunosuppressive drugs and adalimumab to maintain uveitis remission, followed by dose reduction and cessation the conventional second-line drug; maintenance of long-term uveitis remission with adalimumab.
Introduction
Uveitis is a generic term for a collection of more than 30 different phenotypes of intraocular inflammation centred on the uveal tract.1 There is a broad range of systemic inflammatory disorders associated with uveitis including: sarcoidosis, Behcet’s disease, Vogt-Koyanagi-Harada disease, spondyloarthritis. Important infectious causes of uveitis include the herpesviridae, Toxoplasma gondii, Mycobacterium tuberculosis and Treponema pallidum. In approximately 50% of cases, a specific aetiology is not identifiable following extensive workup and is termed undifferentiated (‘idiopathic’).2 As the anatomical location, clinical course and aetiology of the uveitides vary widely, an individualised management approach is essential.
Over the past 15 years, the Standardisation of Uveitis Nomenclature (SUN) research group has developed classification criteria for the 25 clinical phenotypes of uveitis based on anatomic classification, severity gradings of inflammation and definitions for uveitis activity using a super majority Delphi approach with a large group of 76 international uveitis experts.3 This has standardised data recording in uveitis.
Acute anterior uveitis (AAU) is by far the most common clinical phenotype of uveitis4 and episodes are readily controlled with topical corticosteroid therapy in about 90% of patients. Around 50% of patients with AAU are human leucocyte antigen-B27 positive and up to 70% of such patients have an associated spondyloarthropathy, most frequently ankylosing spondylitis.5 Antitumour necrosis factor alpha (TNF-α) directed monoclonal antibody therapy such as adalimumab therapy typically eliminates recurrences of AAU and results in long-term remission of the uveitis.6
Non-infectious intermediate, posterior and pan-uveitis involve the posterior segment of the eye, behave differently and have a broad range of uveitis severity.7 Although far less frequent than AAU, these phenotypes are frequently vision-threatening, typically requiring systemic corticosteroid in the acute phase, and additional immunosuppressive therapy for long-term control of the uveitis to preserve vision, minimise disease complications and minimise treatment side effects.
Despite the heterogeneous nature of uveitis, there have been a number of well-designed studies providing clinical guidance in the management of uveitis.8 The Multicentre Uveitis Steroid Treatment (MUST) trial was a multicentre, partially masked, randomised controlled study, documenting superiority of ‘treat to target’ systemic immunosuppressive therapy over steroid intravitreal implant monotherapy, in the management of vision-threatening non-anterior, non-infectious uveitis.9 The First-line Antimetabolites as Steroid-sparing Treatment was a randomised controlled trial, double-blind, head-to-head comparison between mycophenolate and methotrexate, concluding that mycophenolate mofetil is not superior to methotrexate in controlling inflammation among individuals with non-infectious uveitis.10 The VISUAL 1, 2 and 3 studies were multicentre, double-masked, randomised clinical trials providing evidence for the safety and efficacy of adalimumab over corticosteroid therapy, in patients with non-anterior, non-infectious uveitis.11–13
The Systemic Immunosuppressive Therapy for Eye disease (SITE) studies, a large retrospective case series of ~15 000 patients with uveitis treated over 20 years, reports that conventional systemic immunosuppressive therapy did not result in higher mortality, compared with non-exposed persons, as had been earlier feared.14 Subgroup analysis of the SITE cohort identified that 5% of the intermediate uveitis (IU) patients had multiple sclerosis. This finding informs current clinical practice that requires baseline neuroimaging to exclude demyelinating disease prior to adalimumab use in patients with IU, as there are reports of adalimumab precipitating demyelinating diseases.15 A study from Sydney has shown an increased risk of non-melanoma skin cancers and non-Hodgkin’s lymphoma in patients with uveitis treated with systemic immunosuppressive therapy.16
These studies provide a solid framework for our current approach to systemic therapy for non-infectious uveitis. Systemic corticosteroids provide rapid control of severe uveitis. Although it remains the most effective therapy for severe uveitis, the many well-recognised potential complications, such as osteoporosis, preclude its long-term use. The aim in patients requiring ongoing systemic therapy is durable steroid free remission or, at a minimum, reduction to a daily dose of <7.5 mg/day of prednisolone.17 Steroid-sparing immunosuppressive therapy is required to achieve this in the majority of patients, most frequently initially with conventional drugs such as methotrexate or mycophenolate.18 The presence of associated systemic diseases may modify and guide the choice of immunosuppressant.19
With increasing recognition of anti-TNF biologics as an effective therapy in the management of vision-threatening uveitis, adalimumab is becoming a preferred second-line drug over conventional steroid-sparing agents.20 Although there are five available anti-TNF biologics, most data and clinical experience in patients with uveitis has been gained using adalimumab and infliximab.21 Salvage therapy for patients who are poor or non-responders to anti-TNFs is most commonly tocilizumab, other anti-TNF biologics and occasionally rituximab.22 The use of adalimumab as steroid-sparing systemic therapy was supported and received level A recommendation in recently published guidelines for the treatment of non-infectious uveitis provided by the fundamentals of care for uveitis initiative.21
Before commencing anti-TNF therapy, appropriate screening of patients for latent infections, left ventricular dysfunction and demyelinating disease is essential to minimise risks. Multidisciplinary team management produces the best ocular outcomes, management of comorbidities and minimisation of complications.23
The current multicentre study aimed to collect real-world data regarding the safety and effectiveness of adalimumab to treat vision-threatening non-infectious uveitis and investigate the utility of early commencement of adalimumab.
Methods
A retrospective medical record chart review was conducted at Sydney Eye Hospital, Save Sight Institute Sydney, St Vincent’s Clinic Sydney and Royal Hobart Hospital for a period of 10 years (2011–2020) of all uveitis patients given adalimumab with a minimum follow-up of 6 months. Members of the same multiconsultant uveitis team manage patients across each of these locations. All patients were comanaged by a multidisciplinary team (MDT) comprising ophthalmologists and rheumatologists or clinical immunologists. When clinically indicated, other medical specialties such as infectious diseases and respiratory medicine specialist physicians formed part of the working MDT.
The medical records were reviewed for demographics, clinical diagnoses, clinical course, prior local and systemic therapies, response to therapy and side effects of immunosuppression type. Inflammatory status of each eye at baseline was classified as ‘active’ (based on the clinical findings of at least one active inflammatory chorioretinal or retinal vascular lesion, anterior chamber cell grade of 1+ or higher or vitreous haze grade of 1+ or higher, according to the SUN Working Group and adapted National Eye Institute criteria3 or ‘inactive’ (corresponding to eyes without active inflammatory chorioretinal or retinal vascular lesions as well as an anterior chamber cell grade and vitreous haze grade of 0.5+ or less). All patients had active uveitis at time of adalimumab commencement.
The outcome variables included: corticosteroid-sparing effect, level of intraocular inflammation, visual acuity and time to treatment failure. These data were collected at initiation of adalimumab and reviewed for end points such as oral prednisone dose <7.5 mg, cessation of prednisone or occurrence of treatment failure. Corticosteroid-sparing success was defined as the reduction of the prednisolone dose to ≤7.5 mg/day. Anterior chamber cell count and vitreous haze were graded clinically as described above. Best-corrected visual acuity (BCVA) was converted to logarithm of the minimum angle of resolution (logMAR) for analysis.24 Time to treatment failure was a composite endpoint as defined in the VISUAL-1 and VISUAL-2 studies and was defined as the presence of at least one of the following criteria: new active inflammatory chorioretinal or retinal vascular lesions relative to baseline; a two-step increase in anterior chamber cell grade relative to the last visit; a two-step increase in vitreous haze grade relative to the last visit or a worsening BCVA by two Snellen lines relative to the previous best recorded acuity, anterior chamber cell grade that did not improve to 0.5+ or lower or vitreous haze grade that did not improve to 0.5+ or lower by week 6 were additional treatment failure criteria.11 Adalimumab was administered with a loading dose of 80 mg, followed by a maintenance dose of 40 mg subcutaneously every 2 weeks. An attempt was made to taper corticosteroids if clinically appropriate. Reasons for treatment failure were noted.
Data were analysed using Microsoft Excel 365. Categorical variables were designated as percentages. Continuous variables were designated as means or medians. Incidence rates for clinical events were calculated at time points of interest in a per-eye or per-person analysis depending on the relevant outcome. Time to treatment failure outcomes were assessed with Kaplan-Meier survival analysis using the prespecified treatment failure criteria. Total number of first treatment failure events was divided by the total time contributed by the active and inactive eyes in years to give a failure rate in eye-years of follow-up.
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
Forty-six patients with uveitis, treated with adalimumab were included in the study. Forty-three patients (93.5%) had bilateral ocular involvement with 89 involved eyes. There were 26 (56.5%) male patients and 20 (43.5%) female patients. The most common anatomical diagnosis was panuveitis (n=17, 37.0%), followed by anterior uveitis (n=12, 26.1%), posterior uveitis (n=10, 21.7%) and IU (n=7, 15.2%), respectively. The most common diagnosis was undifferentiated (n=18, 39.1%) (see table 1). The mean age at diagnosis was 37.67 years (SD=15.59).
Clinical diagnosis of patients
Eight (17.4%) patients had a treatment failure while on treatment with adalimumab. The mean time to treatment failure was 459.9 days. The total follow-up period of the 46 patients was 110.4 years making the time to treatment failure, 1 in 12.47 person-years. The median time to failure was 310.1 days (44.3 weeks) with a range of 119–1435 days (17.0–205.0 weeks). The mean follow-up from initial diagnosis is 1629.2 days (4.46 years) and median follow-up is 1629.5 days (4.40 years), with a minimum follow-up period of 6 months. Kaplan-Meier plot of the time to treatment failure is detailed in figure 1.
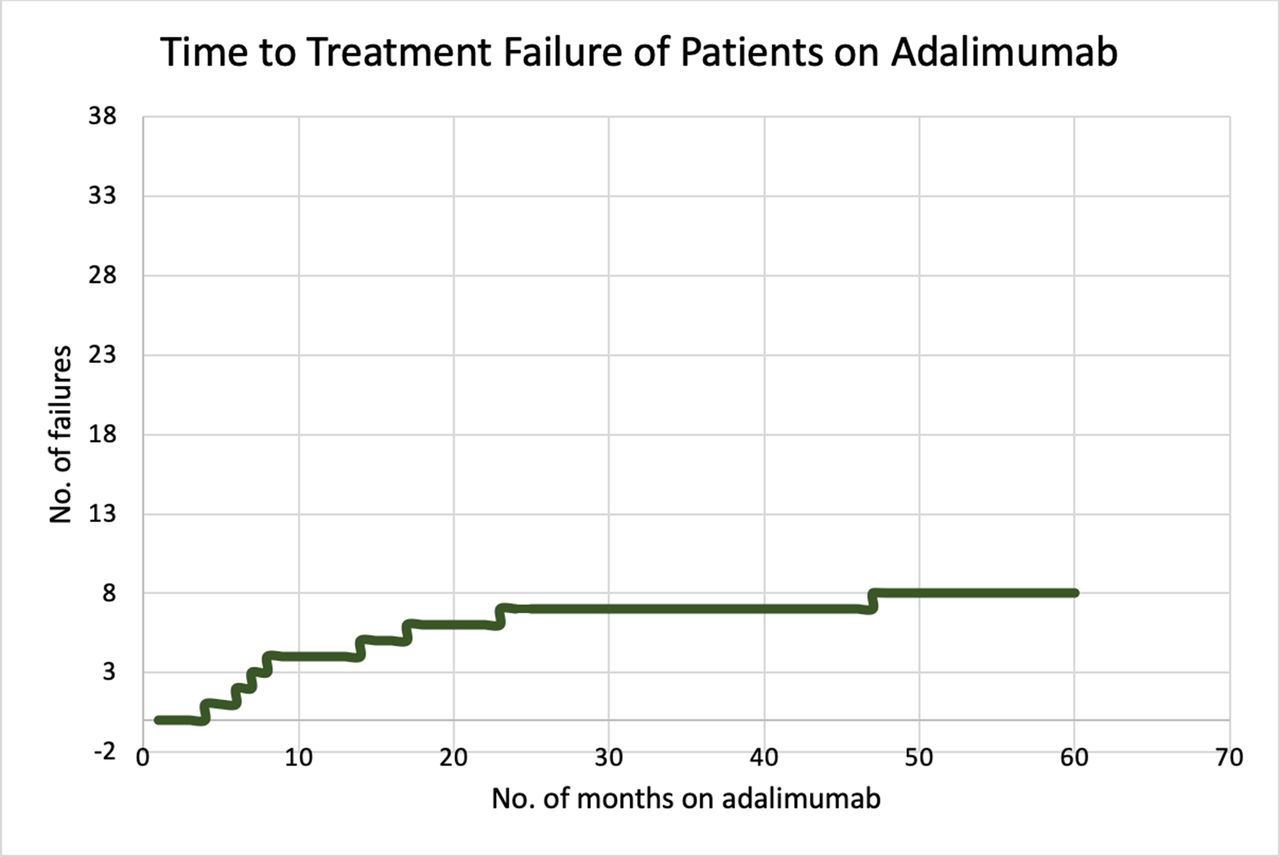
Kaplan-Meier plot of the rate and time to treatment failure of patients on adalimumab.
The mean visual acuity at baseline of the worse eye was logMAR 0.60 with an SD of 0.73, while the mean visual acuity of the better eye was logMAR 0.14 with an SD of 0.26. Only the affected eye is used for those with unilateral disease. The average time to start immunosuppression from diagnosis was 230.5 days (SD=530.0) for the 39 patients who received traditional immunosuppression therapy. The average time to start biological therapy from diagnosis was 747.6 days (SD=784.6). The indications for biological treatment (figure 2) included: uncontrolled inflammation in 22 (47.8%) patients, acute vision threatening disease in 16 (34.8%) patients, requiring prolonged high doses of prednisone to control inflammation in 4 (8.7%) patients, intolerance and undesirable side effects from immunosuppressants in 3 (6.5 %) patients and systemic disease requiring immunosuppression in 1 (2.2%) patient. The mean visual acuity at the start of the adalimumab of the worse eye was logMAR 0.52 with an SD of 0.68, while the mean visual acuity of the better eye was logMAR 0.19 with an SD of 0.34. Of the 89 eyes, 17 (19.1%) eyes improved by at least 2 lines, 21 eyes (23.6%) worsened by at least 2 lines while the remaining, 51 (57.3%) eyes had similar vision at baseline. The mean visual acuity at the latest follow-up (range 1–5 years) of the worse eye was logMAR 0.42 with an SD of 0.72, while the mean visual acuity of the better eye was logMAR 0.17 with an SD of 0.32. Of the 89 involved eyes, 21 (23.6%) eyes improved by at least 2 lines, 5 eyes (5.6%) worsened by at least 2 lines while the rest, 63 (70.8%) eyes had similar vision from the start of adalimumab (see table 2 for visual outcomes).
Visual outcomes of patients
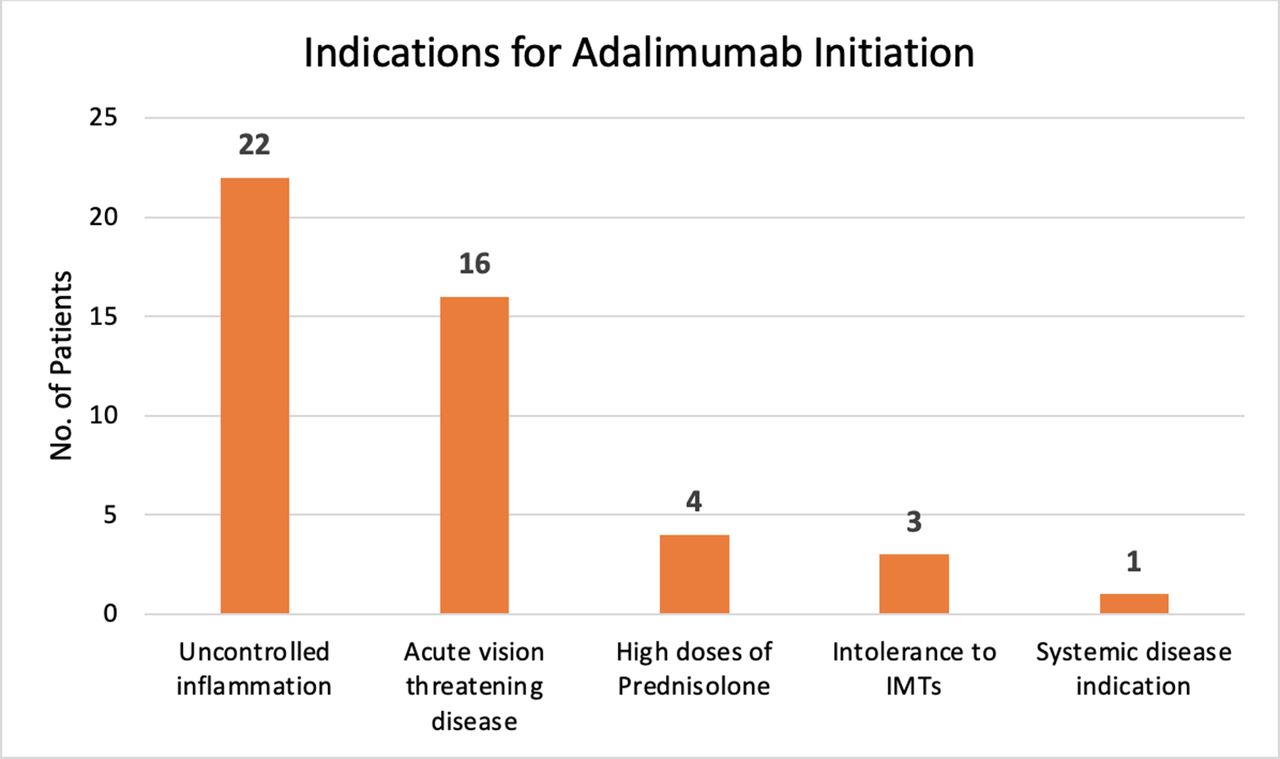
Reasons for adalimumab initiation.
Prednisone dose could be reduced in all patients on biological therapy (figure 3). Forty-five (97.8%) patients were able to either stop prednisolone (34 patients, 73.9%) or reduce their dose to 7.5 mg or less per day (11 patients, 23.9%) over the time of follow-up. One (2.2%) patient required 10 mg prednisolone daily, adalimumab and mycophenolate for control of uveitis. At commencement of adalimumab, 19 (41.3%) patients were on a prednisolone dose greater than 7.5 mg per day, 10 (21.7%) started with a dose of 7.5 mg per day or lower, while 17 (37.0%) were not on prednisone at the commencement of adalimumab therapy. The mean time from start of adalimumab to cessation of prednisone for those who were taking prednisone at onset was 444.4 days (SD 348.3).

{kind=link}
{kind=link}
{kind=link}
Prednisone dose in patients on adalimumab and/or concurrent conventional immunosuppressive agents.
Thirty-four (73.9%) patients managed with adalimumab were concurrently treated with conventional steroid sparing immunosuppressive therapy (IMT), such as methotrexate, mycophenolate or azathioprine, at the start of biological therapy. Twenty-seven (58.7%) patients remained on immunosuppressive agents and adalimumab at the latest review. Adalimumab therapy allowed seven (15.2%) patients to stop their conventional agents; three (6.5%) patients stopped conventional agents prior to starting adalimumab. Nine (19.6%) patients started adalimumab as a first-line agent without using conventional steroid-sparing agents. The prednisolone dose, use of steroid-sparing agents and adalimumab therapy are detailed in figure 3.
In this study, the length of time between diagnosis and commencement of adalimumab was shorter if diagnosed in 2016 or later, compared with diagnosis prior to 2016 (p<0.001) (2016 or later: mean=287.6, SD 278.7; prior to 2016: mean=1207.7 days, SD 854.5). This highlights that once the unit had easier access to adalimumab in 2016, and increasing experience using it, therapy was escalated more rapidly to include adalimumab.
There were five (10.9%) patients who required glaucoma surgery to control elevated intraocular pressure or glaucoma. These surgeries had been performed prior to starting biological therapy. Twelve (26.1%) patients required cataract surgery, including three patients who also had undergone glaucoma surgery. One (2.2%) patient required bilateral vitrectomy, one eye for vitreous haemorrhage and the other eye for tractional detachment. One (2.2%) other patient required a diagnostic vitrectomy to exclude intraocular infection. Seven (15.2%) patients required intravitreal corticosteroids in addition to systemic and topical steroids to control macular oedema during the time course of the study. Two additional (4.3%) patients required orbital floor steroid local therapy for the management of macular oedema. Two patients (4.3%) developed secondary inflammatory choroidal neovascularisation and two (4.3%) additional patient developed branch retinal vein occlusion. These three patients were successfully treated with intravitreal anti-vascular endothelial growth factor therapy.
Discussion
This study provides real-world clinical data supporting the treatment efficacy and safety of adalimumab as well as data regarding the optimum time to add adalimumab therapy to the treatment of patients with severe vision-threatening uveitis. Important findings from this study include: the number of relapses was reduced; the number of patients losing vision was reduced with stable or improved vision in the long term in the majority of patients; prednisolone was ceased or reduced to safe levels in all but one patient and there was a decreased use of additional immunosuppressive drugs. There was a non-statistically trend towards the early introduction of adalimumab, increasing the time to uveitis relapse. Importantly, there were no major adverse events.
The time to treatment failure was 1 in 12.47 person-years and the median time to failure was 44.3 weeks in this study. This is consistent with results of the VISUAL-1 study (24 weeks). We attribute the longer median time to failure to the concomitant administration of IMTs. The VISUAL-1 study demonstrated the efficacy of adalimumab when combined with oral corticosteroids in comparison to corticosteroid monotherapy. In the VISUAL-1 study, patients in the adalimumab group were significantly less likely to have treatment failure than those in the placebo group across all four study outcomes.25 26
The current study highlights that vision was stabilised in the vast majority of patients. 23.6% of eyes worsened by at least two lines from the time of presentation until starting biologics, while only 5.7% of eyes worsened after starting adalimumab therapy. 57.3% retained similar vision from baseline up to starting adalimumab and 71.3% from starting adalimumab to the latest follow-up. Although the patient numbers in the current study are small, given the other clinical trial and case series data previously reported, this study provides further data that supports, the earlier patients are commenced on adalimumab therapy, the more likely that vision will not be lost and that the risk of other structural ocular complications will be reduced, as was demonstrated in the VISUAL-3 study.27
In the present study, prior to adalimumab therapy, nearly 50% of the patients had uncontrolled uveitis despite systemic immunosuppressive therapy and nearly 10% required too high a maintenance dose of corticosteroids. This is consistent with the current literature.14 19 With adalimumab therapy, more than 95% of patients in the current study were subsequently able to taper their corticosteroid dose to less than 7.5 mg, only one patient required a dose of 10 mg. It is likely that starting biological therapy earlier will decrease significantly the need for other second-line immunosuppressive therapy.
A proportion of patients (15.8%), in this study, on adalimumab required additional local corticosteroid therapy. This requirement is consistent with the MUST study, where we see 62% of patients in the systemic arm requiring local therapy to maintain control of their uveitis.9
There are no uveitis clinical trials to guide the use of conventional steroid sparing drugs in combination with adalimumab or other biologics. The results of the ADVISE trial, once complete, should provide useful data regarding this. At present, combination immunomodulatory therapy with corticosteroids, corticosteroid sparing drugs and/or biologics is common clinical practice. In the study reported here, there is a significant proportion of patients on conventional steroid-sparing agents together with adalimumab (58.7%). Patients requiring high-dose corticosteroid therapy at baseline were usually on coadministered conventional IMTs. Seven (15.2%) patients were able to cease conventional immunosuppressant while on adalimumab and had low dose or no prednisolone requirement.
The most common adverse events reported in adults and children reported on adalimumab is localised injection site reaction (including pain, erythema and rash). LaMattina and Goldstein26 summarised the common side effects seen with adalimumab from 13 studies. In the VISUAL-1 industry sponsored phase 3 trial, there was no significant difference between the rate of serious infections between the adalimumab and placebo groups. The VISUAL-3 data, which followed patients for 78 weeks, reported serious events as follows: 4.4 serious infections per 100 patient years, 1.6 malignancies per 100 patient years, 0.8 demyelinating disorders per 100 patient years and 0.5 adverse events leading to patient deaths per 100 patient years.28 In the current study, there were no significant adverse events in patients on biologics. Two (4.3%) patients developed a non-specific skin rash. Adalimumab was continued in each patient without consequence. Another patient developed recurrent respiratory infections from sarcoid related restrictive lung disease and secondary bronchiectasis. Adalimumab was continued, following consultation with respiratory medicine.
The relatively small sample size of the current study, its retrospective design and modest follow-up times limit the interpretation of the data and outcomes of adalimumab therapy. The safety profile may be underestimated if less severe side effects were not recorded in the patient records. The variable follow-up period and the lack of a comparative arm are further limitations of this study.
That said, this study highlights the effectiveness of adalimumab in sight-threatening non-infectious uveitis and suggests benefit in early commencement of biological therapy. Based on the data in this study, adding adalimumab therapy allows reduction of corticosteroid dose to a safe dose (<7.5 mg) or to cease corticosteroids; the use of second-line conventional immunosuppressive drugs and adalimumab to maintain uveitis remission, followed by dose reduction and cessation the conventional second-line drug; maintenance of long-term uveitis remission with adalimumab. It provides further data on the good visual outcomes, decreased ocular complications, robust corticosteroid sparing effect and reduction in other systemic immunosuppression that are possible with adalimumab therapy.
Data availability statement
Data are available on reasonable request. All clinical data can be found in the record sections of Sydney Eye Hospital, St. Vincent’s Hospital Sydney and Royal Hobart Hospital.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for the study was obtained from the Human Research Ethics Committee for New South Wales Health, South Eastern Sydney Local Health District (HREC ref noL51244 (LNR/15/POWH|432l)).
Acknowledgments
The authors acknowledge the staff of Sydney Eye Hospital, St Vincent’s Hospital Sydney and Royal Hobart Hospital for their assistance in collecting data.
References
Footnotes
TLTLS and VY contributed equally.
Contributors SZ and PJM conceived the idea for the manuscript. TLTLS, VY and JMF collected the clinical data from Sydney Eye Hospital, St Vincent’s Hospital Sydney and Royal Hobart Hospital. SZ, PJM, RS, CY, EEC and AS provided the clinical data for Sydney Eye Hospital patients. SZ, PJM and DW provided the clinical data for St Vincent’s Hospital Sydney. PJM, NV and DS provided the clinical data for the Royal Hobart Hospital patients. TLTTS and VY collated the data and drafted the initial manuscript with inputs from SZ and PJM. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.