Article Text

Abstract
Objective The primary aim was to determine endocannabinoid (EC) concentrations of 2-arachidonoylglycerol (2-AG), oleoylethanolamine (OEA), palmitoylethanolamine (PEA) and anandamide (AEA) in the aqueous humour of patients, and to investigate any differences in gender and diabetic or ocular disease status.
Methods and Analysis Adult participants (age >18 years) listed for a routine cataract surgery were recruited. For patients with diabetes, results from their most recent retinopathy grading were recorded. A sample of aqueous humour was removed from the anterior chamber of the patients and snap-frozen in liquid nitrogen. Levels of 2-AG, PEA, OEA and AEA were measured by liquid chromatography-tandem mass spectrometry.
Results Aqueous humour samples were taken from 93 patients (female:male=58:35), with a mean age±SD of 72.7±9.5 years. Following gender-specific analysis, the mean aqueous concentration of AEA in female patients without diabetes was significantly higher than in female patients with diabetes (0.20±0.03 nM vs 0.07±0.02 nM, p=0.001). Among female patients with diabetes, the aqueous concentration of 2-AG was higher in those with diabetic retinopathy compared with those with no retinopathy (0.30+0.16 nM vs 0.04±0.01 nM, p=0.0025). The aqueous level of the sum of EC was higher in those with ocular comorbidity (2.49±0.73 vs 1.44±0.17, p=0.0002).
Conclusion There were gender, diabetes status and comorbidity differences in aqueous humour EC levels. Since EC receptors are present in ocular tissues, including the retina (neurons, glia and endothelial cells), differential levels of ECs in the aqueous humour of patients with and without diabetes may provide a novel therapeutic target for diabetic retinopathy.
- drugs
- experimental & laboratory
- retina
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Components of the endocannabinoid system are widely present in the eyes and play a role in the endogenous signalling pathway in both the anterior and posterior eye.
Their presence in the aqueous humour of patients with diabetes compared with patients without diabetes and whether its level is associated with active neovascularisation in people with diabetic eye disease are not known.
What are the new findings?
We report different ocular concentrations of selective endocannabinoids according to diabetes, retinopathy and gender status.
Findings from this study could form a basis to explore endocannabinoids as a therapeutic target for treatment of diabetic eye disease.
How might these results change the focus of research or clinical practice?
This study forms the basis for future studies to investigate the role of endocannabinoid signalling or related compounds in the pathogenesis of diabetic eye disease.
Studies on endocannabinoids should report on gender, diabetes status and use of cyclo-oxygenase-2 inhibitors.
Background
Sight-threatening diabetic retinopathy (STDR) from non-resolving vitreous haemorrhage, tractional retinal detachment and diabetic maculopathy is associated with retinal capillary occlusion and breakdown of the retinal inner blood–retinal barrier.1 It is the leading cause of blindness among individuals aged 20–74 years in the UK,2 with nearly all patients with type 1 diabetes and >60% of patients with type 2 diabetes having some form of retinopathy by the first decade of diabetes.3 4 Vascular endothelial growth factor (VEGF) and other inflammatory mediators induced by hyperglycaemia and ischaemia are instrumental in developing diabetic retinopathy,2 5 6 and intravitreal anti-VEGF biologics, steroid implants and retinal laser photocoagulation remain the mainstay of treatment.7 However, as many patients remain visually impaired, further knowledge of novel substances or growth factors associated with ischaemia-induced angiogenesis is important as we seek novel therapeutic strategies to treat and prevent STDR.
Endocannabinoids are naturally produced chemicals which are known to exhibit neuroprotective and anti-inflammatory effects in models of central nervous system (CNS) and retinal degenerations.8 9 The endocannabinoids anandamide (AEA) and 2-arachidonoylglycerol (2-AG) are found throughout the eye, with the exception of the lens,10 and bind to cannabinoid 1 receptor (CB1) and cannabinoid 2 receptor (CB2). CB1 is expressed in the ciliary body, trabecular meshwork, Schlemm’s canal and retina,11 while CB2 is present in the retina and may contribute to normal visual function.12 The structurally related compounds N-oleoylethanolamine (OEA) and N-palmitoylethanolamine (PEA) are also widely distributed in the CNS and periphery, but do not have affinity for CB1 and CB2 receptors and are thus termed endocannabinoid-like compounds. They are, however, ligands for several non-cannabinoid receptor targets of endocannabinoid localised to the eye, including peroxisome proliferator-activated receptor,13 transient receptor potential type vanilloid 1 receptor14, the G protein-coupled receptors GPR18, a cannabinoid-related receptor that is activated by N-arachidonoyl glycine,15 and GRP55 found in rod photoreceptors.12
The presence of these components supports a potential role for the ocular endocannabinoid system (ECS) in the endogenous signalling of both the anterior and posterior segments of the eye. Indeed, endocannabinoid levels have been shown to be enhanced in many ocular pathologies, including diabetic retinopathy,16 age-related macular degeneration16 and glaucoma.17 In diabetic retinopathy, tissue 2-AG was increased in the iris, and AEA increased in the retina, ciliary body and cornea.16 Similarly, AEA was increased in age-related macular degeneration in the retina, choroid, ciliary body and cornea.17 No previous studies have examined the levels of endocannabinoid in the aqueous humour of patients with diabetes compared with patients without diabetes, and whether levels are associated with STDR. Further, in view of previous studies implying that gender and diabetes may affect endocannabinoid concentrations,18–23 we investigated any differences of aqueous endocannabinoid concentration between gender.
Methods
We conducted a single-centre, cross-sectional pilot study to investigate the levels of endocannabinoid and endocannabinoid-like compounds in the aqueous humour of patients undergoing routine cataract surgery. The primary objective was to quantify levels of endocannabinoid (2-AG, AEA, OEA and PEA) and compare them in patients with or without diabetes and to look for differences in gender. Adult participants (age >18 years) were recruited from Royal Derby Hospital cataract clinics. For patients with diabetes, results from their most recent diabetic retinopathy grading were recorded and graded according to the English Diabetic Eye Screening Criteria: no retinopathy (R0), background retinopathy (R1), preproliferative retinopathy (R2), proliferative retinopathy (R3) and maculopathy (M1). Patients with diabetic maculopathy, preproliferative or stable treated proliferative diabetic retinopathy were commenced on nepafenac drops, a non-steroid anti-inflammatory drug, on the day prior to surgery to reduce the risk of pseudophakic macular oedema. Aqueous humour samples were obtained through a paracentesis at the start of the operation using a 27 Rycroft cannula on a 1 mL syringe (BD), decanted into a labelled 1.0 mL CryoPure vial (Sarstedt), snap-frozen in liquid nitrogen and stored in a −80°C freezer prior to analysis. Labelling was anonymised in accordance with the Human Tissue Authority guidance. No adverse events were reported from the procedure.
Laboratory analysis
The extraction, purification and quantification of endocannabinoids from ocular fluid were performed using a method modified from an established procedure for analysis of endocannabinoids in plasma and mammalian tissues.18–22 Internal standards 30 µL of 2-AG-d8 (5 µM) and 15 µL of AEA-d8 (28 µM) were added to each sample prior to extraction. The analytical Liquid chromatography-mass spectrometrymass spectrometry (LC-MS/MS) method used was not an isotope dilution method and hence does not require an isotopically labelled internal standard for each analyte. Since the chemical structures of AEA, OEA and PEA are very similar, the use of the single internal standard (AEA) is justified. Ethyl acetate:hexane (650 L 9:1 v/v) was added to each sample and vortexed for 10 min. Samples were then centrifuged (13 000 rpm, 10 min, 4°C). The upper organic layer was removed, and where present the extraction of the aqueous layer was repeated, pooling the supernatants for drying. Samples were reconstituted in 50 µL acetonitrile by vigorous vortexing, and endocannabinoids were quantified against a series of extracted standards. A modular Exion LC series (Sciex, Warrington, UK) ultra High Performance Liquid Chromatography (uHPLC) system with a Waters UPLC BEH C18 1.7 µm (2.1×150 mm) column held at 60°C was used with an injection volume of 5 µL and a gradient elution flow rate of 0.45 mL/min. Mobile phase A was water with 1 g/L ammonium acetate and 0.1% formic acid, and mobile phase B was acetonitrile with 1 g/L ammonium acetate and 0.1% formic acid premixed in 10% water. The QTRAP 6500+ mass spectrometer (Sciex) was used with positive ion electrospray detection in multiple reaction monitoring (MRM) mode. Precursor and product ions monitored were as follows: 2-AG (379.1/287.2), AEA (348.1/62.0), OEA (326.2/62.0), PEA (300.2/62.0), 2-AG-d8 (387.2/294.2) and AEA-d8 (356.2/63.1).
Patient involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Statistical analysis
Normality assumption was tested and rejected using the D’Agostino-Pearson omnibus test and outliers were detected. We therefore compared endocannabinoid levels between treatment groups using Mann-Whitney ‘t’-test or one-way analysis of variance, and differences between groups were considered to be significant at p<0.05 after correcting for multiple comparisons. Statistical analyses were performed with GraphPad Prism V.8.3 (GraphPad Software, San Diego, California).
Results
Aqueous humour samples were taken from 93 patients (female:male=58:35), with a mean age±SD of 72.7±9.5 years (table 1), of whom 32 had diabetes (female:male=20:12). Ocular comorbidity was present in 19 patients (8 macular degeneration, 5 glaucoma, 2 iritis, 2 retinal vein occlusions, 2 treated retinal detachments). All four endocannabinoids were identified in the aqueous humour samples, and the mean concentration±SEM (nM) of AEA, 2-AG, OEA and PEA were 0.11±0.01, 0.07±0.01, 0.16±0.02 and 0.92±0.08, respectively, after adjusting for statistical outliers. Table 2 describes the endocannabinoid levels according to diabetes, gender and ocular comorbidity status.
Baseline characteristics
Aqueous endocannabinoid levels
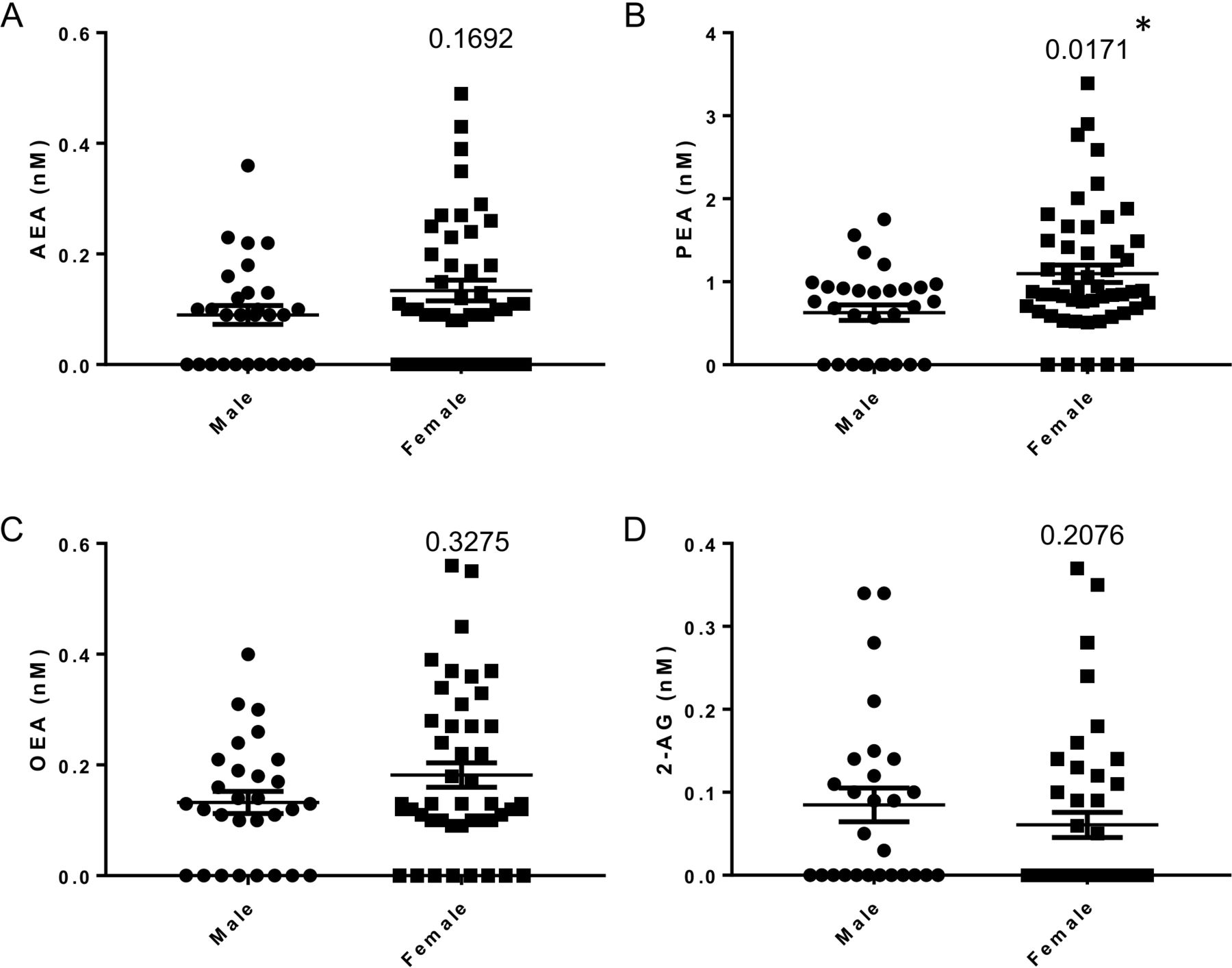
The sum of all endocannabinoids was significantly higher in women than in men (1.77±0.20 nM vs 1.00±0.15 nM, p=0.0298), which was largely driven by the significantly higher levels of PEA in women compared with men (1.1±0.10 nM vs 0.63±0.09 nM, p=0.0171) (figure 1A-D).

Ocular concentration of endocannabinoids (AEA (A), PEA (B), OEA (C) and 2-AG (D)) in male and female patients. Data are presented as scatterplots and analysed by Mann-Whitney non-parametric analysis. 2-AG, 2-arachidonoylglycerol; AEA, anandamide; OEA, oleoylethanolamine; PEA, palmitoylethanolamine. (*) Significant value
When comparing patients with or without diabetes, aqueous concentrations of AEA were non-significantly lower in those with diabetes compared with those without diabetes (0.07±0.02 nM vs 0.13±0.02 nM, p=0.098) (figure 2A), while the mean concentration of 2-AG was non-significantly higher in patients with diabetes compared with those without diabetes (0.08±0.02 nM vs 0.05±0.01 nM, p=0.067) (figure 2D). The mean aqueous concentrations of PEA and OEA were similar between patients with and without diabetes (figure 2B,C). Comparisons between patients with and without ocular comorbidity showed a similar trend, with concentrations of 2-AG observed to be non-significantly higher in patients with ocular comorbidity (0.17±0.03 nM vs 0.25±0.14 nM, p=0.067) and concentrations of AEA shown to be non-significantly higher in patients with ocular comorbidity (0.13±0.03 nM vs 0.07±0.11 nM, p=0.0853) (figure 3). The aqueous level of the sum of endocannabinoids was higher in those with ocular comorbidity (2.49±0.73 vs 1.44±0.17, p=0.0002) (table 2).

Ocular concentration of endocannabinoids (AEA (A), PEA (B), OEA (C) and 2-AG (D)) with and without diabetes. Data are presented as scatterplots and analysed by Mann-Whitney non-parametric analysis. 2-AG, 2-arachidonoylglycerol; AEA, anandamide; OEA, oleoylethanolamine; PEA, palmitoylethanolamine.

Ocular concentration of endocannabinoids (AEA, PEA, OEA and 2-AG) according to ocular comorbidity. 2-AG, 2-arachidonoylglycerol; AEA, anandamide; OEA, oleoylethanolamine; PEA, palmitoylethanolamine.
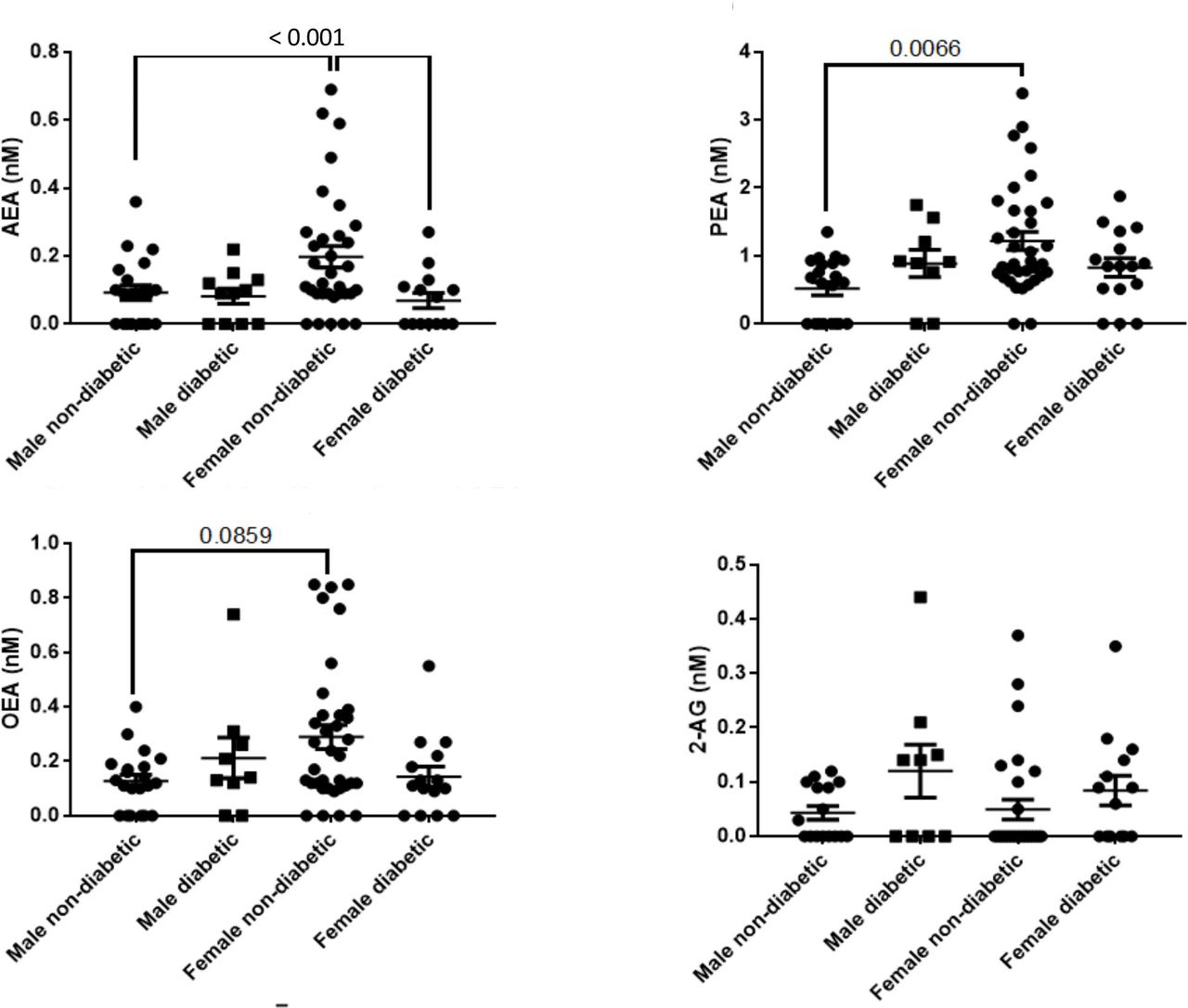
Following gender-specific analysis, the aqueous concentration of AEA in women was significantly lower in patients with diabetes compared with patients without diabetes (0.07±0.02 nM vs 0.20±0.03 nM, p<0.001) (figure 4), and the mean aqueous PEA in women without diabetes was significantly higher than in men without diabetes (1.22±0.14 nM vs 0.83±0.14 nM, p=0.0001). Among women with diabetes, the aqueous concentration of 2-AG was higher in those with diabetic retinopathy compared with those with no retinopathy (0.30±0.16 nM vs 0.05±0.02 nM, p=0.0025) (table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ocular concentration of endocannabinoids (AEA, PEA, OEA and 2-AG) according to gender and diabetes status. 2-AG, 2-arachidonoylglycerol; AEA, anandamide; OEA, oleoylethanolamine; PEA, palmitoylethanolamine.
Aqueous endocannabinoid concentrations by severity of retinopathy
Discussion
While endocannabinoids receptors have been shown to be expressed in various tissues of the eye, this study investigated aqueous concentrations of endocannabinoids in individuals with or without diabetes. We observed differences in the aqueous concentrations among individuals undergoing routine cataract surgery according to gender and diabetes status. In women without diabetes, higher levels of aqueous PEA and the sum of endocannabinoid were found compared with men without diabetes, and AEA was lower in women with diabetes compared with those without diabetes. The levels of AEA and OEA were lowest in women with diabetes with more significant retinopathy. When comparisons were made by severity of retinopathy, aqueous 2-AG levels were greatest in women with retinopathy, lower in men with no retinopathy and lowest in patients without diabetes. Diabetes status and ocular comorbidity suggested trends in lower aqueous levels of AEA. While the underlying cause and role of the differences in ocular concentration of these endocannabinoids remain speculative, we contend that this observation supports the need for further studies to investigate the potential role of ECS in the pathogenesis of diabetic retinopathy.
In the whole group, prior to gender stratification, we observed the aqueous concentration of 2-AG was slightly higher in patients with diabetes compared with those without diabetes, while the concentration of AEA was slightly lower in those with diabetes compared with those without diabetes, with PEA and OEA similar between patients with and without diabetes. A similar observation was noted when comparing those with and without ocular comorbidity. However, following gender stratification, the aqueous concentrations of AEA in women without diabetes were significantly higher than in both men and women without diabetes, with higher PEA and sum of endocannabinoid in women without diabetes compared with men without diabetes. Men without diabetes had the lowest values for each endocannabinoid, which were higher in men with diabetes. Our observation of the reduced aqueous AEA concentrations in diabetes is in contrast to a previous study which showed increased tissue levels of AEA in the retina, ciliary body and cornea.16 The reason for this is unclear, but the higher levels in women without diabetes may have produced this paradox and the gender of the samples was not specified. It is not known if non-steroidal anti-inflammatory drugs provided periprocedure may play some role in influencing the results as endocannabinoids are metabolised by cyclo-oxygenase 2 (COX-2).24 The ethanolamides AEA, OEA and PEA are hydrolysed by fatty acid amide hydrolase, which is inhibited by COX-2 inhibitors, and 2-AG is oxidised by COX-2 to active metabolites. COX-2 is increased in human diabetic and ischaemic retina as well as in retinal astrocytes of animal models of proliferative retinopathy and in cell lines grown under hypoxic conditions.25 Prostanoids are angiogenic and induce VEGF-A, and COX-2 inhibition can reduce angiogenesis26; therefore, the use of nepafenac drops preoperatively may have had an influence on both proinflammatory and anti-inflammatory mediators. 2-AG, which has a different metabolic pathway, was increased in more severe retinopathy in women, which compares with previous findings.16 A trial of nepafenac drops in patients without diabetes prior to cataract surgery would be informative.
Gender differences in circulating endocannabinoid have previously been reported.19 23 While the reason for gender differences seen in circulating endocannabinoid, and now in ocular endocannabinoid, is unknown, it is thought to be due to the interaction between sex hormones and the ECS. Previous studies have shown that oestrogen modulates the endocannabinoid activity.27 28 Thus, future studies to determine the role of endocannabinoid-based therapy in modulating the pathogenesis of diabetic retinopathy should include gender stratification. Unfortunately, we did not have clinical information on the levels of sex hormones, or any documentation of use of hormone replacement therapy or oral contraceptive pills.
The aetiological role of ECS in the pathogenesis of diabetic retinopathy is unclear. A previous study has reported the beneficial effects of CB1 receptor inhibition or genetic deletion27 in the development of diabetic retinopathy. In addition, CB1 receptor inhibition was shown to limit the vascular inflammation and cell death in a mouse model of diabetic retinopathy and in human retinal cell line exposed to high glucose,29 and attenuates hyperglycaemia-induced apoptosis in retinal pigment epithelial cells.30 Since diabetic nephropathy shares some pathogenic features of diabetic retinopathy which characterised diabetic microvascular diseases, it is important to note that the CB1 receptor is overexpressed by renal podocytes in animal models in both type 1 and type 2 diabetes.31 32 In contrast to our observation in the present study, reduction of 2-AG, which acts on both CB1 and CB2, was observed in the renal cortex from mice with early streptozotocin (STZ)-induced diabetes, and podocyte CB2 receptor expression is markedly downregulated in human biopsies from patients with advanced diabetic nephropathy.33 These previous data on diabetic nephropathy indicate that the protective CB2 receptor signalling is impaired while the detrimental CB1 receptor signalling is enhanced in diabetic microvascular diseases. It is likely that both hyperglycaemia and hypertension are important drivers of these changes since alterations as in cultured podocytes exposed to high glucose, were shown to increase CB1 receptor expression,34 while mechanical stress, mimicking glomerular capillary hypertension, downregulates CB2 receptors.33 35 By extrapolation, these differences may have an impact on the endocannabinoid ocular fluid concentration observed in the present study.
Some limitations to our study which may affect the interpretation of our study should be acknowledged. First, we do not have detailed metabolic and clinical parameters of study participants, such as haemoglobin A1c levels, 24-hour blood pressure levels, duration of diabetes, or concurrent glucose-lowering and blood pressure-lowering therapies. The latter is also relevant since therapies which reduce activation of the renin angiotensin system have been shown to attenuate diabetic retinopathy progression.36 Furthermore, active maculopathy and proliferative retinopathy must be controlled prior to cataract surgery, and all patients with diabetic maculopathy, preproliferative or stable treated proliferative diabetic retinopathy were commenced on the anti-inflammatory nepafenac drops a day before surgery to reduce the risk of pseudophakic macular oedema. The potential effects of these routine presurgery protocols to reduce inflammation on the ocular concentration of endocannabinoid are not known. A further limitation is the relatively small number of patients and the unbalanced higher number of female patients, which limit our full interpretation of the observed ocular endocannabinoid levels as well as stratification of patients according to degree of diabetic retinopathy and gender status. Nonetheless, we believe that the current study adds to the available literature regarding the role of endocannabinoid fluid in the pathogenesis of diabetic retinopathy. While previous intervention studies with CB1 receptor antagonists have been performed in animal models of diabetic nephropathy,31 34 37 we believe evidence derived from this study as well as from others should form a basis for future studies to investigate the effects of modulating the ECS in models of diabetic retinopathy.
References
Footnotes
Contributors PR, SO’S and II: conceived the study, drafted the study proposal and applied for grant to support the analysis of the study. PR: undertook sample collection. DB and CO: analysed the ocular fluid sample for endocannabinoid concentration. All authors contributed to the writing of the manuscript and agreed on the final draft.
Funding The study was partly funded by seed grant funding from the National Eye Research Centre (grant number SAC034).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was provided by the NRES North East York (REC reference number: 15/NE/0031). Informed consent was obtained.
Provenance and peer review Not commissioned; externally peer reviewed.