Article Text

Abstract
Purpose To determine whether there was a change in the resistance pattern of bacteria isolated from cases of conjunctivitis following the introduction of over-the-counter availability of chloramphenicol in 2005.
Design and setting Retrospective review of laboratory records for adult patients with suspected bacterial conjunctivitis between 2001 and 2012 attending the Royal Liverpool University Hospital.
Participants Patients with suspected bacterial conjunctivitis. Organisms were identified by standard laboratory methods. Scanty growth and normal flora were considered as a negative result. For positive results, susceptibility testing was undertaken as per British Society for Antimicrobial Chemotherapy guidelines.
Main outcome measures Prevalence of groups of bacteria associated with acute conjunctivitis and their resistance to chloramphenicol, ciprofloxacin, gentamicin, and methicillin.
Results A total of 8209 conjunctival swabs were reviewed; 1300 (15.8%) were considered positive, of which 977 (75.2%) and 323 (24.8%) bacteria were identified as Gram positive and Gram negative, respectively. Staphylococcus aureus was the most prevalent organism identified. Resistance of all bacterial isolates to chloramphenicol was 8.4% varying from 3.0% to 16.4% while that for ciprofloxacin and gentamicin was 16.4% and 14.0%, respectively. Methicillin resistance among S. aureus was 8.3%.
Conclusion Resistance to chloramphenicol has remained stable since being made available over the counter. Among Gram-positive bacteria, the most prevalent causative agent of bacterial conjunctivitis, chloramphenicol sensitivity remains high.
- conjunctivitis chloramphenicol resistance
- MRSA
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Bacterial conjunctivitis is common and often treated empirically with topical antimicrobials. Inappropriate use of antimicrobials has led to increased bacterial resistance.
What are the new findings?
Among Gram-positive bacteria, the most prevalent cause of bacterial conjunctivitis, chloramphenicol sensitivity remains high.
How might these results change the focus of research or clinical practice?
Topical chloramphenicol remains a suitable first-line treatment for bacterial conjunctivitis.
Background
Acute infective conjunctivitis is an inflammation of the conjunctiva secondary to a bacterial or viral infection. It is a common condition with bacterial conjunctivitis having an estimated incidence of 135 per 10 000 in the USA.1 In severe cases, it may result in conjunctival scarring and secondary damage to the ocular surface. A meta-analysis2 concluded that while bacterial conjunctivitis is often self-limiting, antimicrobial use is associated with improved rates of clinical and microbiological remission. Inappropriate use of antimicrobials, however, is associated with increased bacterial resistance, and in recent years there has been a global drive to reduce the prescribing of antimicrobials. While prescribing chloramphenicol for conjunctivitis among general practitioners in the UK has fallen,3 its use has increased several fold since 2005, when it became the first antibiotic available over the counter.4 Surveillance of causative organisms and resistance susceptibility patterns are important in guiding antimicrobial selection. While large studies in the USA5 6have investigated trends in bacterial resistance to antimicrobials over the last decade, these have limited application in the UK as chloramphenicol, an antibiotic very commonly used in the UK, is not used in the USA due to the rare purported association between topically administered chloramphenicol and aplastic anaemia. A review of its use in the UK concluded that topical chloramphenicol was not a significant risk factor for inducing dose-related bone marrow toxicity.7 To determine resistance patterns of bacteria isolated from cases of conjunctivitis to commonly prescribed antimicrobials, laboratory reports of patients presenting with suspected acute conjunctivitis were reviewed. The prevalence of the organisms causing acute bacterial conjunctivitis and their sensitivities to chloramphenicol and other commonly used topical antimicrobials were examined between 2001 and 2012.
Methods
Laboratory records for all bacterial swabs taken from adult patients with suspected bacterial conjunctivitis presenting to the Royal Liverpool University Hospital, UK, between 2001 and 2012 were reviewed.
Conjunctival samples were collected using cotton swabs from the inferior conjunctival fornix as per local protocol. Samples were inoculated onto chocolate agar, Columbia agar with 5% horse blood and MacConkey agar plates, and placed in a 5% CO2 incubator at 37° or in air at 37° (MacConkey agar plate). Plates were examined after 24 and 48 hours of incubation for the presence of pathogens associated with conjunctivitis. Organisms were identified by standard laboratory methods. A negative result was defined as either a scanty growth of bacteria or those that were considered as part of the ‘normal conjunctiva flora’ such as coagulase-negative staphylococci, diphtheroids and alpha-haemolytic streptococci. Because of the difficulty in distinguishing clinically between bacterial and viral conjunctivitis, samples were also often taken for viruses, in particular adenovirus and herpes simplex virus. Samples for viruses were analysed by real-time PCR.8 Data for viral isolates were only available from 2006 onwards.
Susceptibility testing was carried out as per British Society for Antimicrobial Chemotherapy (BSAC) guidelines,9 and BSAC templates were used to interpret zone inhibition diameters for the following antimicrobials: chloramphenicol, ciprofloxacin and gentamicin.
Analysis
The data are time series and are analysed using linear regression models. We investigated for a possible cycling changes in data via a polynomial component of second, third or fourth order. The order was chosen to maximize the adjusted coefficient of determination. The statistical significance of trend and cycles was judged at level 0.05.
Results
A total of 8209 conjunctival swab results were reviewed, of which 1300 (15.8%) were considered bacterial culture positive. The isolation rate by year ranged from 9.8% to 25.2%, and 977 (75.2%) and 323 (24.8%) of bacterial isolates were identified as Gram-positive and Gram-negative organisms, respectively (table 1). All organisms isolated have been listed in box 1. Between 2006 and 2011, 3293 viral conjunctival samples were collected. An adenovirus was identified in 707 of these, and 21 (2.97%) of which were also bacterial culture positive.
Bacterial isolates from adults with suspected bacterial conjunctivitis attending Royal Liverpool University Hospital (2001–2012) and their resistance to chloramphenicol
Organisms identified from bacterial isolates from adults with suspected bacterial conjunctivitis attending Royal Liverpool University Hospital (2001–2012)
Haemolytic streptococcus
Haemophilus influenzae
Moraxella catarrhalis
Morganella morganii
Neisseria gonorrhoeae
Neisseria meningitidis
Pseudomonas sp.
Staphylococcus aureus
Streptococcus pneumoniae
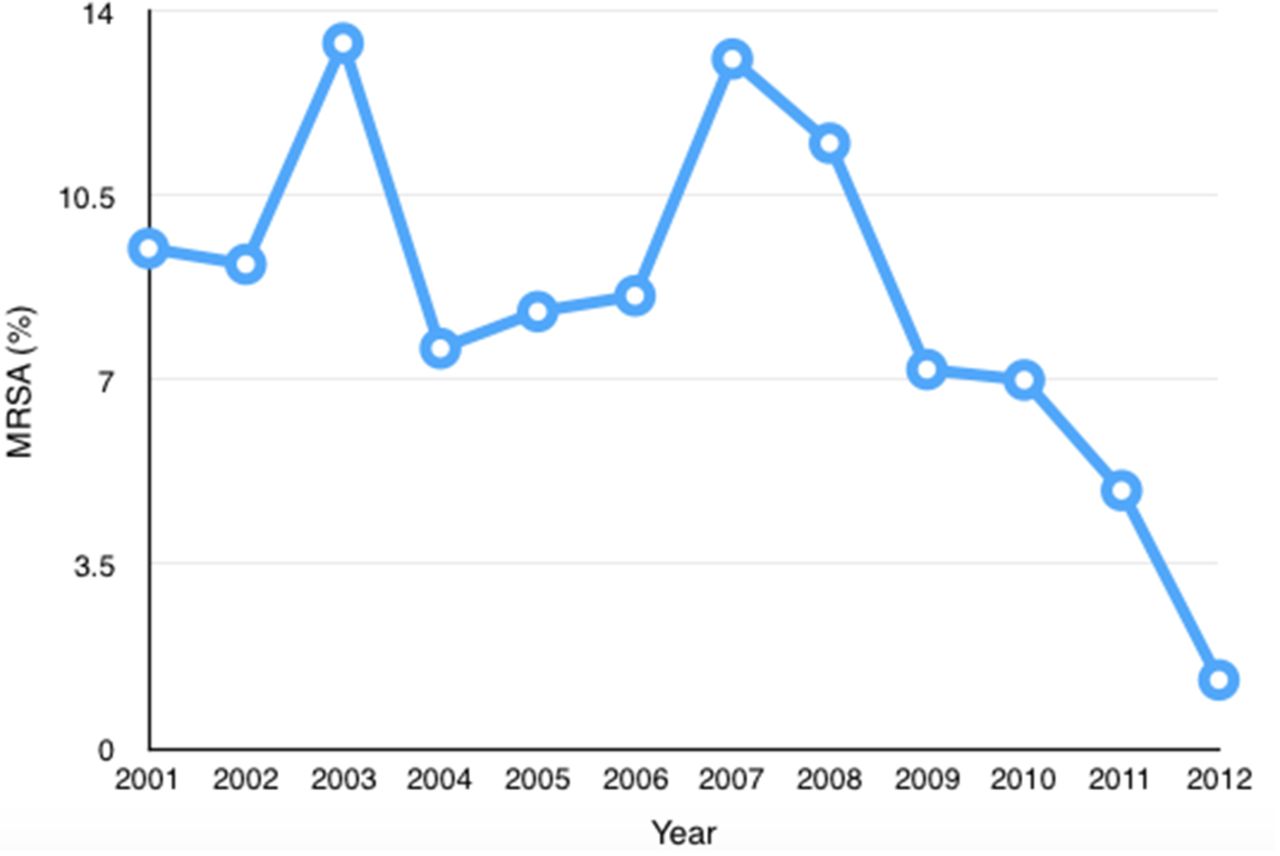
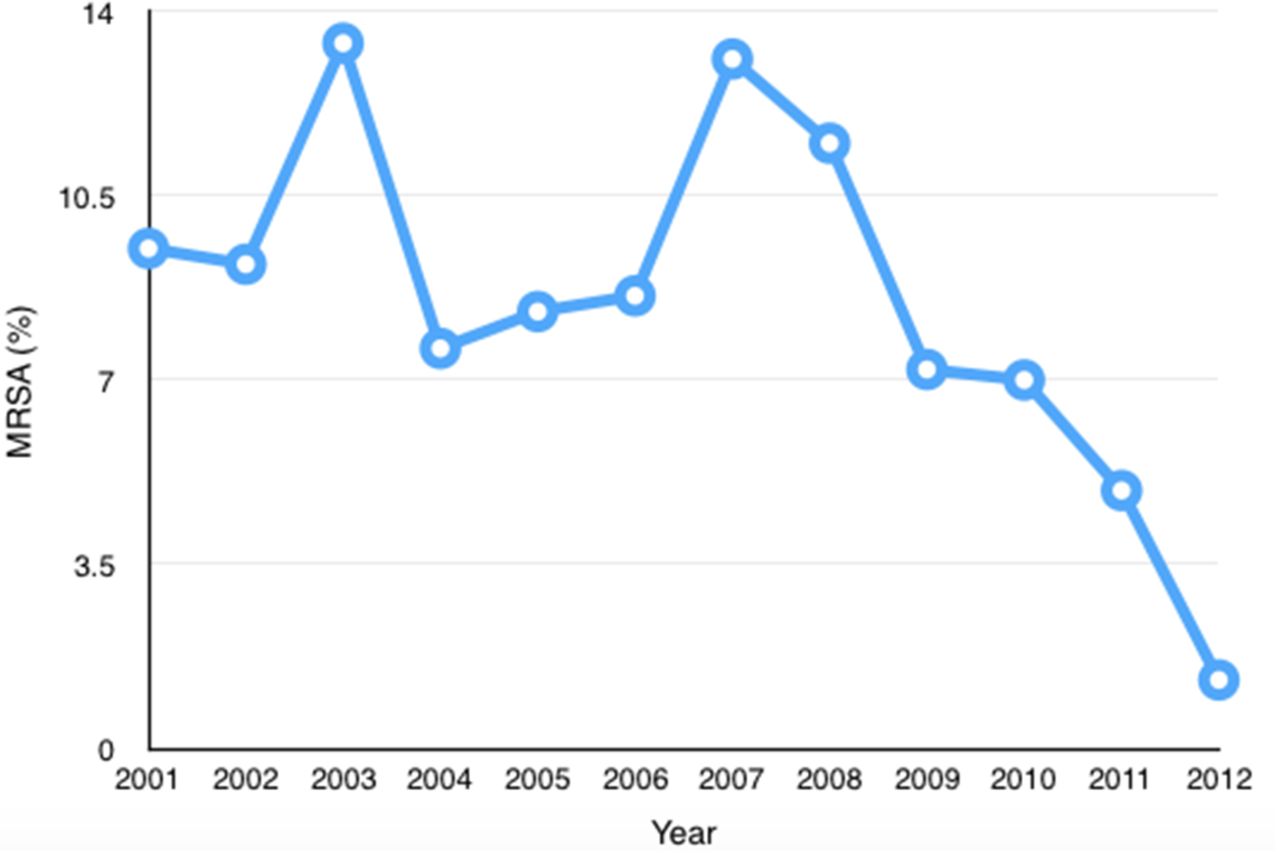
In bacterial culture-positive samples, resistance to chloramphenicol varied from 3.0% to 16.4% (table 1) and was predominantly among Gram-negative organisms. There was no significant change in resistance to chloramphenicol over the study period; in particular, there was no change after 2005. Resistance to ciprofloxacin and gentamicin over the period of 2001–2012 was found in 16.4% and 14.0% of isolates, respectively, predominantly among Gram-positive organisms (80.1% and 69.2%). There was no significant association between antimicrobial resistance and isolation rate for each year under study (p=0.58). There was a significant reduction in methicillin resistance among Staphylococcus aureus isolates (mean 8.3%, minimum 1.3%, maximum 13.4%, p=0.038) over the 12-year period (figure 1).
{kind=link}
Percentage of Staphylococcus aureus isolated resistant to methicillin
Discussion
Acute infective conjunctivitis is a common condition. Although cases of viral and bacterial conjunctivitis have some clinically distinguishing features, it is not always easy to differentiate them. It is not surprising, therefore, that in the majority of patients studied, the aetiological agent was an adenovirus. Although antibacterial agents would not be indicated in a viral conjunctivitis, because of the difficulty in distinguishing bacterial and viral causes, it is not unreasonable to prescribe broad-spectrum antimicrobials prior to obtaining culture results. It is of note, therefore, that while prescribing of chloramphenicol has fallen, its use has increased due to its availability over the counter.
In non-ocular infections, over and inappropriate use of antimicrobials has led to an increase in resistant organisms10 and the monitoring of antimicrobial susceptibility and resistance trends is therefore important. It is of interest, therefore, that over the study period there was no evidence of an increase in antimicrobial resistance to commonly prescribed topical antimicrobials. BSAC breakpoints used for susceptibility testing are derived for systemically delivered antimicrobials. Caution is, therefore, needed interpreting resistance patterns to topically applied agents. Although models for topical breakpoints for cases of keratitis are becoming available,11 there are currently no interpretative breakpoints for topical antimicrobials for cases of conjunctivitis.
Based on the systemic breakpoints, chloramphenicol resistance has remained stable since 2005 when chloramphenicol was made available over the counter. Among Gram-positive bacteria, chloramphenicol sensitivity remains high. Compared with many topical antibacterial agents, chloramphenicol has excellent intraocular penetration following topical application.12 Similar to that reported in studies from the USA,5 ,6 S. aureus was the most prevalent organism. The prevalence of methicillin-resistant S. aureus (MRSA) was, however, much lower than reported in Japan13 and USA5 ,6 and also significantly reduced over the time period of this study. A reduction of MRSA infections over this period of time has been demonstrated in other infections,14and this has been attributed to enhanced screening and decolonisation of patients with MRSA in recent years.
A limitation to this study was the low-positive isolation rate. Other papers have shown variable rates of positive isolates,15and one study had a similar isolation rate to this paper (15.8%).16 This difference might be explained by the inclusion of all bacteria isolated in some studies rather than pathogenic bacteria only. In addition, our isolation rate might be lower as bacterial swabs were taken from all patients with suspected conjunctivitis including those with viral conjunctivitis. Many patients present after they have already started topical antibiotic treatment, this may have reduced the positive isolation rate.
Although chloramphenicol remains a useful agent for bacterial conjunctivitis, in particular for cases of Gram-positive conjunctivitis, it should not be used if contact lens related or if Pseudomonas aeruginosa is suspected.17
Despite the ready availability of chloramphenicol over the counter during the last 7 years, there has been no increase in chloramphenicol resistance nor a change in the bacterial spectrum in this cohort of patients.