Article Text

Abstract
This review assesses different clinical aspects of the various known drug-induced corneal deposits, based on the corneal layer involved (epithelium, stroma and/or endothelium), and based on the drug class. The most well-known condition caused by drug deposits is vortex keratopathy, or corneal verticillata, which is a whorl-like opacity in the corneal epithelium. Vortex keratopathy is commonly caused by certain cationic amphiphilic drugs such as amiodarone, antimalarials, suramin, tamoxifen, chlorpromazine and non-steroidal anti-inflammatory drugs. These deposits usually occur once a certain dose of the drug is reached. Most cases present with mild to moderate symptoms with minimal visual impairment. Most of these deposits resolve automatically, after months to years of drug cessation. Notably, other drug classes can cause deposits in all three layers of the cornea. Chlorpromazine, gold, rifabutin, indomethacin and tyrosine kinase inhibitors can cause stromal deposits, with reduced visual acuity when the anterior stroma is involved. Chlorpromazine and rifabutin can also cause deposits in the endothelial layer of the cornea. Regardless of the type of corneal deposit, local therapies such as topical lubricants or corticosteroids may help improve symptoms. Drug cessation or modification can also be helpful but should be weighed against the systemic risks of the underlying disease.
- cornea
- drugs
- ocular surface
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Many drugs are known to cause ophthalmologic side effects. Often, certain drugs affect specific anatomical structures of the eye. For example, hydroxychloroquine accumulates in the retinal pigment epithelium and causes a dose-related maculopathy.1 Drugs can also lead to deposits in the cornea. Iatrogenic drug-induced deposits are often asymptomatic but lead to visible opacities that often target specific layers or regions of the cornea. While medications can reach the cornea through the tears, the aqueous humour, or the perilimbic vasculature, the pathophysiology and mechanisms leading to layer-specific deposits are not well understood. Some deposits are well-described in the literature, while others are barely mentioned in case reports. Raizman et al have discussed in a review drug-induced epithelial changes.2 Our review collates and describes the various known drug-related deposits affecting the three layers of the cornea (epithelium, endothelium and stroma), providing an overview categorised by corneal layer and further details by drug class. This is analogous to the current classification of corneal dystrophies, another important cause of corneal deposits.3 To help the reader rapidly identify possible causative aetiologies to various deposit location and morphology, table 1 summarises the drug-induced deposits by corneal layer along with common differential diagnoses. As it may be difficult to recognise certain deposits visually, the medical and drug anamnesis plays an important role in determining the proper diagnosis.
Differential diagnosis of corneal deposits, by layer85–88
Corneal layers overview
Epithelial deposits
Some of the most commonly recognised drug-related corneal deposits produce a vortex keratopathy, or corneal verticillata, a whorl-like opacity in the corneal epithelium. This pattern is generally caused by cationic amphiphilic drugs, following the natural centripetal migration pattern of the corneal epithelium from limbus to centre. The differential diagnosis of vortex keratopathy is briefly reviewed in table 2. Epithelial deposits may be due to drug accumulation or drug interference with epithelial metabolism/homeostasis.
(A) Differential diagnosis of vortex keratopathy and (B) grading system of amiodarone-induced corneal deposits as described by Orlando et al
Many corneal epithelial keratopathies are related to lysosome dysfunction due to exogenous or endogenous causes. Exogenous causes involve certain drugs which cause lysosomal dysfunction leading to the accumulation of excess phospholipids in all of the corneal layers and adjacent structures.4 Cationic-amphiphilic drugs can easily enter lysosomes in the basal epithelial layer of the cornea where they bind to cellular lipids, leading to medication-lipid complexes that are resistant to enzymatic degradation and therefore accumulate as deposits in the cornea.4 Amiodarone inhibits lysosomal phospholipase A2, leaving the inner membrane of the cell susceptible degradation by proteases.5 Another drug, suramin, inhibits the enzyme iduronate sulfatase, which is required for lysosomal degradation and thus leads to accumulation of glycosaminoglycans.6
Endogenous causes of vortex keratopathy include lysosomal storage diseases. For example, sphingolipidoses are rare inherited disorders of complex lipids (gangliosides and sphingomyelin) that involve the cornea in three conditions: Fabry’s disease (angiokeratoma corporis diffusum), multiple sulfatase deficiency and generalised gangliosidosis. Fabry’s disease, an X linked recessive genetic disorder, causes atypical corneal whorls in addition to progressive nephropathy and peripheral neuropathy leading to painful extremity dysesthesias. Female carriers may, however, present with only corneal findings.
Stromal deposits
Many drugs can cause deposits in the corneal stroma, such as chlorpromazine, gold, rifabutin, indomethacin and tyrosine kinase inhibitors (TKIs) such as vandetanib. Medications enter the corneal stroma via the aqueous humour, limbal vasculature and tear film. Stromal deposits can be pigmented, crystalline or refractile.7 Antipsychotic phenothazines, particularly chlorpromazine, cause a dose-related light-induced deposition in the corneal stroma. Deposits begin as brown opacities in the posterior stroma, Descemet membrane and endothelium8; the anterior stroma is not involved unless high doses are administered. Some patients develop a reduced visual acuity. Clofazimine, a drug used for the treatment of leprosy, psoriasis, pyoderma gangrenosum and discoid lupus, causes crystalline deposition in the conjunctiva and anterior corneal stroma. Deposits resolve with treatment discontinuation.9 Finally, isotretinoin, a drug used mainly for the treatment of acne, has been shown to cause corneal opacities in the superficial stroma in 5.1% of patients.10 These changes do not interfere with visual acuity and typically resolve within 2–10 months of drug cessation, although some deposits may persist longer in some patients.11
Endothelial deposits
Although most drug-related corneal deposits occur either in the epithelium or stroma, some drugs such as chlorpromazine and rifabutin have been shown to cause deposition in the endothelium. Endothelial deposits are best diagnosed with retroillumination. Chlorpromazine causes granular white-grey opacities diffusely distributed along the entire corneal endothelium.12 Rifabutin deposits are stellate and refractile, initially affecting the periphery then extending to the central cornea; they can persist as a golden hue and progress despite drug cessation.7 In most cases, endothelial deposits are asymptomatic, but they can persist after drug cessation, and are sometimes accompanied by retinal dysfunction.
Drug classes overview
Cationic-amphiphilic drugs
Antimalarial drugs
Antimalarial drugs such as chloroquine, hydroxychloroquine, quinacrine, tafenoquine and amodiaquine are known to cause epithelial corneal deposits.13 Some of these medications are also used in the treatment of rheumatoid arthritis and lupus. Clinical presentation of antimalarial-induced corneal deposits typically occurs from 2 weeks to a few months of starting the medication.14 Tafenoquine-induced vortex keratopathy occurs in 93% of users.15 These deposits can be asymptomatic or cause blurred vision or halos. Amodiaquine can result in corneal deposits known as lysosomal-like inclusions.16 Cessation of treatment can sometimes result in a progressive reversal of deposits, and therefore resolution of ocular symptoms.17 However, irreversible keratopathy despite drug cessation has been reported with amiodaquine and tafenoquine.14 Antimalarials can also induce visual loss secondary to a ‘bull’s eye’ maculopathy due to drug accumulation in the retinal pigment epithelium, leading to neurosensory retina degeneration and disruption of the outer retinal layer visible on optical coherence tomography (OCT).18 19
Amiodarone
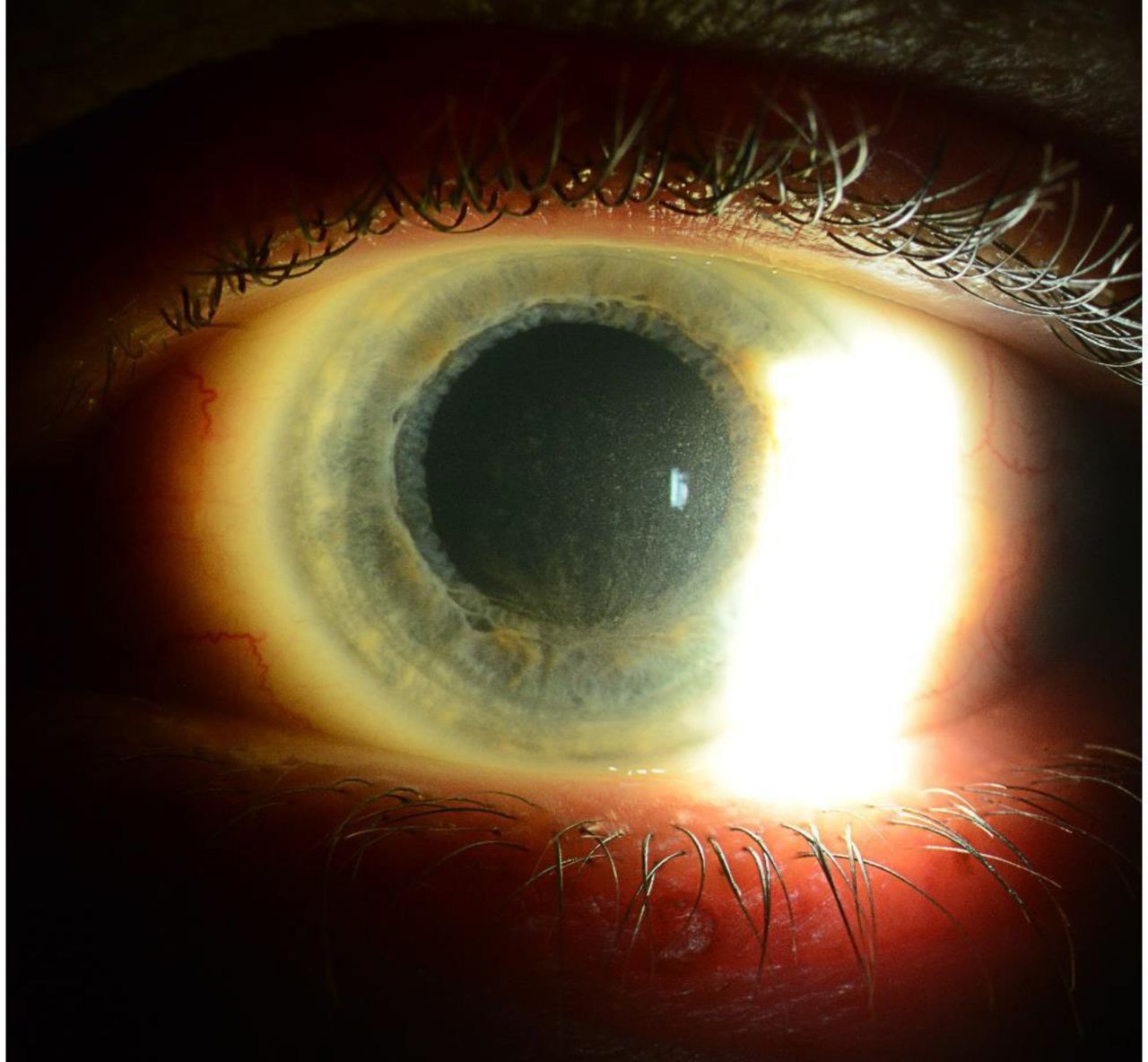
Amiodarone is the most widely used antiarrhythmic drug. Nearly all patients on this medication (98%) develop corneal epithelial changes at doses starting at 200–300 mg/day.20 21 Visual acuity is not typically impaired; however, patients may report photophobia, halos and irritation.20 Corneal changes start after 2 weeks to 1–4 months of treatment.22 The typical clinical finding is bilateral vortex keratopathy with brown to golden deposits (figure 1).22 The configuration of the deposits evolves as a factor of the duration of amiodarone therapy, as shown in the grading system proposed by Orlando et al (table 2B).23

Amiodarone-induced vortex keratopathy.
Keratopathy begins at the level of the inferior pupillary margin, forming collections which gradually become linear with time and finally progress to the well-known swirl of vortex-like patterns. Neither epithelial fluorescein staining nor corneal neovascularisation are seen.23 Although deposits are primarily present in the epithelium just anterior to Bowman layer on confocal microscopy,23 the keratopathy does involve all layers of the cornea. Usually, the keratopathy is bilateral and symmetric but can start in one eye before the other. While no loss of visual acuity and no subjective ocular symptoms were noted in most series, a possible link between amiodarone and optic neuropathy has been described.24 25 Unilateral or bilateral optic disc oedema, decreased visual acuity and sometimes acute vision loss characterise the optic neuropathy.24 Amiodarone-induced retinopathy has been described in a case report.26
Corneal deposits are reversible within 3–20 months after stopping amiodarone use.27 Since the corneal deposits are rarely symptomatic, treatment is not typically discontinued for this reason. However, the presence of optic neuropathy may merit drug cessation and, in such cases, cardiology should be consulted prior to any medication change.
Suramin
Suramin is used as both an antitumour and antiparasitic agent. Approximately 33% of patients on high doses of suramin develop vortex keratopathy.6 In a series of six patients who were given high-dose suramin for adrenocortical carcinoma, corneal deposits were symmetrical and bilateral28; one patient out of six developed anterior lens epithelium opacities, two patients reported foreign-body sensation and visual acuity impairment and the others were asymptomatic.28 Vortex keratopathy, punctate keratopathy and peripheral epithelial erosion are the main corneal epithelial toxicities noted. In another series of 27 patients treated with suramin for metastatic prostate cancer, five patients (18.5%) developed mild vortex keratopathy without altered vision.29 Five patients with AIDS who received 500 mg to 1 g of suramin weekly developed an asymptomatic epithelial and subepithelial vortex keratopathy, with the extent being proportional to the dose of suramin.30 Dose reduction or drug cessation led to improvement of these corneal changes which appear to be completely reversible.6
Tamoxifen
Tamoxifen is a selective oestrogen receptor inhibitor used in the treatment of hormone-sensitive breast cancer. Ocular toxicity with tamoxifen has been reported in the literature from a lowest cumulative dose of 7.7 g to a highest dose of 100 g.31 Small doses of tamoxifen over a 2-year period can cause clinically significant corneal deposits in approximately 11% of cases.32 These corneal subepithelial deposits also produce a reversible vortex keratopathy, which disappears after drug cessation. Of note, tamoxifen can also cause retinopathy.33 Retinal changes occur more frequently than corneal changes at high doses (180–320 mg/day),34 resulting in crystal-like deposits around the macula with macular oedema and granular changes in the retinal pigment epithelium, leading to impaired visual acuity.32 34
Chlorpromazine
Chlorpromazine is a phenothiazine antipsychotic that can cause skin and ocular pigmentation at high doses over a long period. It is also known to target the eyelids, conjunctiva, cornea, crystalline lens and rarely retina (figure 2).35 The most common ocular side effect of chlorpromazine is anterior lens capsule dusting followed by corneal stromal pigment dusting.36 In the cornea, it typically induces deposits in the stroma37 38 and endothelium,12 39 and causes vortex keratopathy in a minority of cases.40 The ocular deposits are believed to be composed of melanin and chlorpromazine metabolites that accumulate in sun-exposed areas through a phototoxic reaction.41
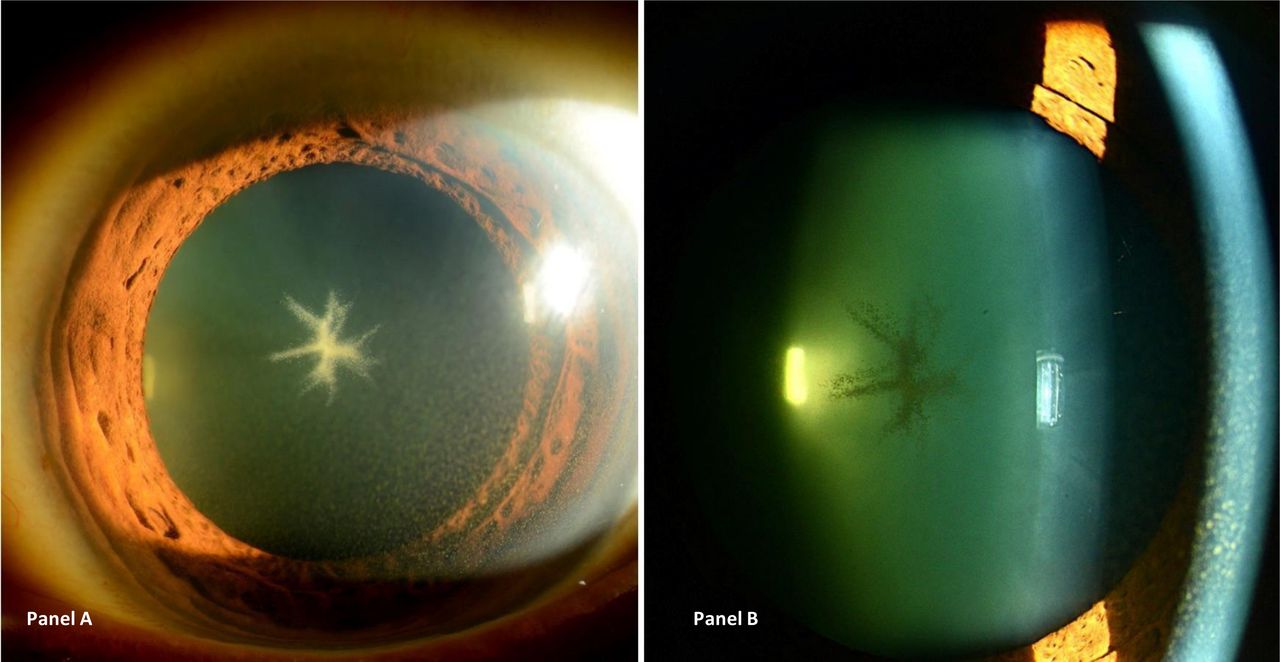
Stellate anterior subcapsular cataract and diffuse pigmented corneal deposits secondary to chlorpromazine, seen on slit lamp examination using diffuse (panel A) and focal (panel B) illumination.
Corneal changes occur mostly at a 2-year cumulative rate of low doses (>300 mg/day) of the medication, and in patients taking a high dose (>2 g/day) over a short time interval (few months). Slit lamp examination reveals granular white-grey opacities diffusely distributed along the entire corneal endothelium, most confluent centrally and decreasing in density towards the periphery. Ocular toxicity may be accompanied by corneal oedema.38A stellate-shaped opacification can be present in the central anterior cortex of both crystalline lenses. The corneal pigmentary deposits are generally irreversible, although some reports of slowly reversible epithelial keratopathy have been noted.35 ,42
Amantadine
Amantadine is an cationic amphiphilic inhibitor of replication of influenza A virus which can concentrate in the lysosomes.43 It has been recently widely used for the treatment of Parkinson disease. Among numerous corneal complications caused by amantadine such as corneal endothelial dysfunction, superficial punctate keratitis and corneal oedema, amantadine was shown also in a case report to induce corneal deposits in the basal layer of the corneal epithelium.44 However, although cationic and amphiphilic, amantadine does not cause vortex keratopathy, but a ‘belt-shaped epithelial opacity’ at the centre of the cornea.44 Possible mechanisms of these deposits are: (i) phospholipidosis (like amiodarone) in the corneal epithelium, or (ii) organic cation transporters (amantadine is a substrate for these transporters which are responsible for the excretion, uptake, elimination and distribution of cationic drugs, toxins and waste products).44 45 No follow-up of the patient was described by the authors in their case report.
Non-cationic amphiphilic drugs
Some non-cationic amphiphilic drugs can also induce corneal deposits; however, they usually do not cause the vortex keratopathy typical of cationic amphiphilic drugs.
Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs (NSAIDs) (naproxen, ibuprofen) are anionic-amphiphilic drugs and can cause corneal deposits. These deposits develop rapidly after days of treatment with NSAIDs, especially at high doses such as 1200 mg/day for ibuprofen.46 Corneal adverse effects range from vortex keratopathy to opacities in Bowman layer and Descemet membrane.8 Naproxen-induced keratopathy presents with parallel lines in the superficial cornea similar to a fingerprint pattern, followed by the development of the clear-cut corneal verticillate pattern.47 Ibuprofen also induces a similar deposit pattern.46 Indomethacin is also known to induce vortex keratopathy.48 These changes are reversible within weeks after treatment cessation. Corneal deposits due to NSAIDs are rare and the specific reasons why only some patients develop such deposits have not been elucidated.
Gold salts
Gold salts are used to treat rheumatoid arthritis. Crystalline corneal deposits were first described in 15 patients who received gold thiomalate intramuscular injections for rheumatoid arthritis.49 Corneal deposits are graded from 0 (no deposit) to 3 (marked deposits). Epithelial deposits were present in 87% of patients who received gold treatment. These deposits typically present following a cumulative dose exceeding 100 mg, representing 7 months of treatment.49 Confocal microscopy has also revealed gold salts deposits in other corneal layers such as the stroma. Gold deposits were seen in the anterior and middle stroma in a patient treated with gold sodium thiomalate for 6 years.50 Likewise, in a patient treated with gold salts for 32 years, every corneal layer contained highly reflective deposits with the biggest dimension of deposits located in the anterior stroma.51 Usually, gold deposits are asymptomatic and do not cause visual impairment or other ocular symptoms.49 As such, the presence of gold salts deposits is not an indication for treatment discontinuation. When the drug is stopped for other reasons, deposits have remained even after 9 months of drug cessation.49
Antibiotics
Rifabutin
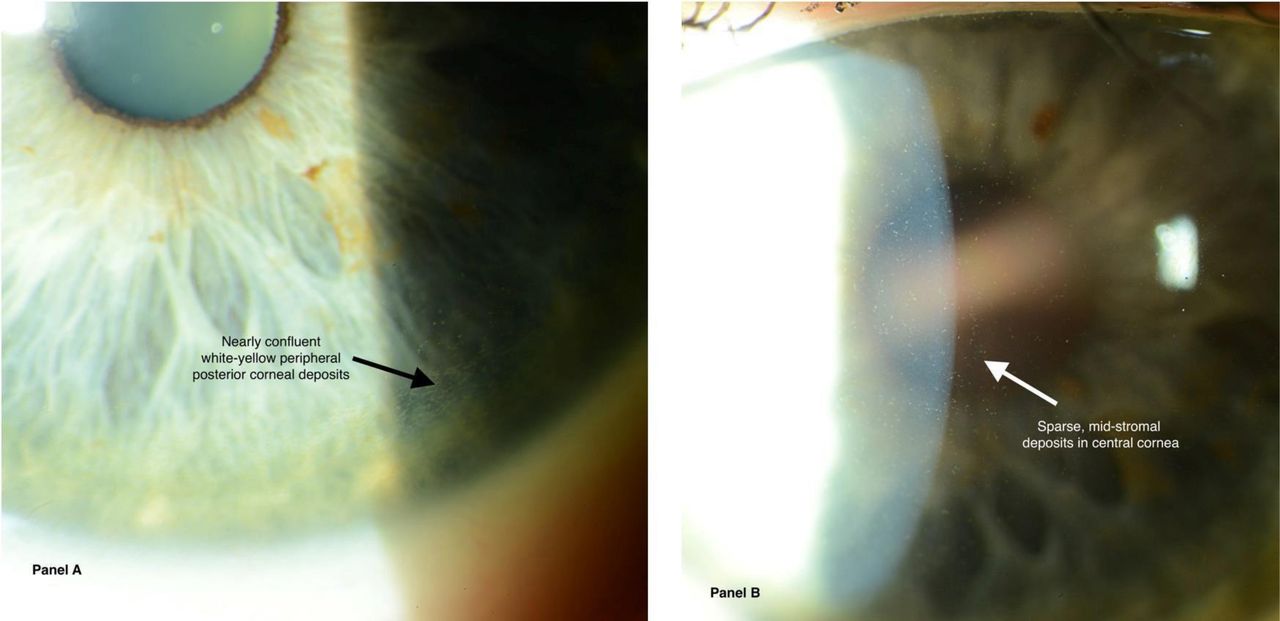
Rifabutin is an antibiotic which is commonly used in the treatment of tuberculosis and in the prevention and treatment of Mycobacterium avium complex (MAC) in immunodeficient patients. The pathophysiology of rifabutin-induced corneal deposits is not yet understood. A possible explanation is that, due to the drug’s high lipid solubility, these deposits derive from the aqueous humour and, following trans endothelial transport, assemble in the deep stroma.52 In the first report of rifabutin-induced corneal deposits, bilateral stellate corneal endothelial deposits were found in 24% of immunodeficient children receiving systemic rifabutin for prevention of MAC.53 Longer duration of rifabutin treatment was a risk factor for deposit development.53 Corneal deposits usually appear after 18 months of treatment,54 are usually bilateral and at first peripheral and stellate55 (figure 3). Although these deposits increase in number progressively and gradually affect the central cornea, no visual impairment is noted.55 Rifabutin deposits are localised in the deep corneal stroma as visualised using anterior segment OCT and confocal microscopy.56 However, unlike most other drugs cited above, no resolution of deposits is seen after treatment discontinuation.56
{kind=link}
{kind=link}
{kind=link}
(A) Peripheral corneal deposits secondary to rifabutin. (B) Mid-stromal deposits in central cornea secondary to rifabutin.
Clarithromycin
Clarithromycin is a cationic non-amphiphilic macrolide antibiotic. Like rifabutin, it is usually used in immunodeficient patients to prevent MAC. Clarithromycin can cause epithelial changes that results in subjective blurring of vision without objective impairment in visual acuity.57 While these changes are not well described in the literature, deposits and symptoms usually resolve with treatment discontinuation.
Clofazimine
Clofazimine is a part of a multitreatment regimen for leprosy. The first study describing clofazimine-induced corneal deposits was published in 1976.58 It comprised 19 patients who were on clofazimine for psoriasis, with a daily dose of 400 mg for 1–2 months. A corneal pigmentation rate of 53% was found in patients treated for 6–24 months.59 Fine, brownish lines, similar to chloroquine keratopathy, can be observed with no visual impairment.58 Another study revealed polychromatic crystalline deposits accompanied by red-to-brown staining of the bulbar conjunctiva and peripheral cornea, with no visual impairment.60 All of these changes were reversible after treatment cessation.
Antitumoral agents
Vandetanib
Vandetanib (ZD6474) is a TKI used mainly in the treatment of metastatic solid malignancies, such as medullary thyroid cancer and non-small cell lung cancer (NSCLC).61 62 Although not cationic or amphiphilic, vandetinib induces vortex keratopathy of gold to brown epithelial deposits.61 Vandetinib inhibits epidermal growth factor receptor (EGFR) in addition to vascular endothelium growth factor receptor 2. Since EGF is an important growth factor for corneal epithelial homeostasis,63 this inhibition of EGFR causes defective epithelial turnover and migration and therefore vortex keratopathy. Confocal microscopy showed hyper-reflective deposits in the epithelium as well as subepithelial nerve plexus, microdots in the stroma and hyper-reflective keratocytes in the anterior stroma.62 An appearance similar to cornea verticillata has also been described.64 Visual complaints included symptoms of lacrimation and blurred vision. After treatment with carboxymethyl cellulose, sodium chloride ointment and decreasing the vandetinib doses, the patient’s symptoms improved but corneal findings persisted.64
Osimertinib
Osimertinib (AZD9291) is another TKI approved for the treatment of metastatic NSCLC. Briefly, this drug has been shown to induce a vortex keratopathy16 similar to vandetinib.65
Cytarabine arabinoside
Cytarabine arabinoside is an oncologic drug used mainly in the treatment of acute myelogenous leukaemia. After 10 doses of 3 g/m2 two times per day for >5 days, patients can start experiencing lacrimation, photophobia and blurred vision. The same dose schedule administered over 2–4 days (<5 days) does not cause ocular toxicity.66 As shown in a prospective confocal microscopy study of 11 patients treated with cytarabine arabinosid, cytarabine causes necrosis of basal epithelial cells with a granular cytosolic signal; these necrotic cells migrate to the wing layer and ultimately to the apical epithelial layers over time.67 This leads to bilateral corneal changes beginning as numerous central reflective epithelial microcysts measuring 5–6 mm in diameter and disseminated reflective granular and irregular intraepithelial opacities mainly in the basal epithelial layers.68 69 Corneal opacities disappears within 4 weeks of drug cessation.66 Treatment with topical dexamethasone may help symptoms resolve within a few days and the disappearance of corneal microcysts within 1 week.70 The application of topical loteprednol etabonate 0.5% four times daily was recently shown to help relieve the symptoms within 1 week and disappearance of corneal changes after 2–3 weeks.69
Antibody-drug conjugates
Antibody-drug conjugates (ADCs) are a combination of an antibody targeting a specific receptor, and a drug attached to this antibody. ADCs have multiple uses in oncological and rheumatological conditions. Nearly 50% of patients receiving ADCs have ocular side effects.71 The corneal toxicity of these medications is thought to result from off-target delivery and deconjugation of the cytotoxic drug. However, more complex mechanisms involving antibody-mediated delivery have not been ruled out.
Trastuzumab emtansine
Trastuzumab emtansine is an ADC composed of an antibody that binds human epidermal growth factor 2 and DM1 (a maytansinoid), forming the ADC T-DM1, and is mainly used in solid tumours, mainly breast and gastric cancers. Although the ocular adverse events are numerous (conjunctivitis, glaucoma, cataract),71 those affecting the cornea include a symptomatic punctate keratitis with blurred vision which occurs in 5.4% of cases.72 Vision impairment can progress, and dose reduction helps relieve the symptoms.71
Monoclonal antibodies
Corneal limbal infiltrates were described with dupilumab, a monoclonal antibody used for allergic diseases (chronic sinusitis, eczema, etc), which is also better known to cause conjunctivitis.73 Belantamab mafodotin, a drug used for relapsed and refractory multiple myeloma, was demonstrated to cause superficial punctate keratopathy and/or microcyst-like epithelial changes.74
Other ADCs
Numerous other ADCs were reported to have corneal side effects, some of which are still under investigation. All of these ADCs are used for oncological purposes and include: gemtuzumab ozogamicin (Mylotarg), lorvotuzumab mertansine (IMGN901), IMGN242 (huC242-DM4), SAR3419 (CD19-DM4), SGN-CD19A, AVE9633, SGN-75 (CD70-MMAF), SAR566658 (DS6-DM4), BT-062 and many more.71 Corneal changes are the most frequent ocular adverse events, leading to peripheral microcystic epithelial deposits that coalesce towards the centre. Small intraepithelial clusters of whitish material are also occasionally seen. Patients present with blurred vision and dry eyes. Pathogenesis is not completely understood. The majority of corneal changes are mild, reversible and controllable with dose modification and/or symptomatic treatment.
Management and follow-up of corneal deposits
Due to the sparse cases in the literature, no clear recommended treatment exists for corneal deposits. As we have seen above, the majority of deposits typically resolve with drug cessation and are not visually significant. Therefore, no change in medication regimen and no further workup is needed if we diagnose an isolated finding of cornea verticillata.
Some medications that are known to cause corneal deposits can also cause other ocular ocular adverse events such as optic neuropathy or retinopathy. These include amiodarone, tamoxifen, antimalarials and chlorpromazine. The extent of corneal verticilliata caused by these medications does not correlate with the risk of optic neuropathy and retinopathy. In such cases, routine monitoring should be performed with automated visual fields and OCT to assess for optic nerve and retinal structure and function.75 To avoid visually significant adverse events, a dose reduction or a switch to another medication should be considered in the patient presenting with new visual symptoms. In the patient taking rifambutin, particular consideration of ethambutol-related optic neuropathy should be investigated as these drugs are often used concomitantly.
While the management of corneal drug-induced deposits is often limited to observation and conservative management, some treatments have been proposed in the literature. For example, topical heparin eyedrops, prepared with a sterile phosphate-free solution of 0.1% sodium hyaluronate, has been reported as a possible treatment for amiodarone-induced vortex keratopathy.76 Otherwise, local therapies such as topical lubricants or corticosteroids may provide an improvement in symptoms.
Topical treatments
Finally, corneal deposits can result from topical ophthalmologic treatments. Chalky white precipitate and crystalline patterns within epithelial defects have been described with topical fluoroquinolones. While ciprofloxacin drops and ointment are most commonly implicated,77 reports of deposits from topical moxifloxacin,78 norfloxacin,79 ofloxacin,80 tosufloxacin,81 sparfloxacin82 and gatifloxacin83 have been published as well. Furthermore, topical heparin may cause cornea verticillata.76 Long-term use of topical epinephrine may lead to pigmented adenochrome deposits.84
Conclusion
Numerous drugs can accumulate in the cornea or alter local metabolism, leading to visible deposits on slit lamp and confocal microscopy. Most cases present with mild to moderate symptoms with little to no visual impairment. While often not clinically indicated, drug cessation can sometimes result in resolution of the deposits over days to years. Drug cessation or modification can be helpful to reduce symptoms but should be weighed against the systemic risks of the underlying disease.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors All authors have made substantial contributions to all the following: the conception and design of the study, drafting the article or revising it critically for important intellectual content and final approval of the version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None of the authors has any financial/competing interests to disclose, except M-CR who discloses being a consultant for TALLC, Han-ALL, Santen and an employee of EBSCO. This study does not contain any personal identifying information.
Provenance and peer review Not commissioned; externally peer reviewed.