Article Text

Abstract
Background/Aims To analyse the complications and outcomes of vitrectomy surgery for endophthalmitis.
Methods This was a retrospective case series. All cases that underwent 23-gauge vitrectomy surgery for endophthalmitis at a tertiary centre between 1 February 2013 and 1 February 2018 were included. Main outcome measures were as follows: visual acuity (VA) at final visit and post-vitrectomy complications.
Results 33 patients were included in the study with 20 men and 13 women, average age 63 years. Main post-surgical causes for endophthalmitis included phacoemulsification (n=9), trabeculectomy (n=5), intravitreal injection (n=5), corneal graft (n=4), vitreoretinal surgery (n=3) and endogenous endophthalmitis (n=6). Average follow-up was 18 months (SD 14). 21/33 (64%) patients had baseline perception of light VA. Analysis of exogenous endophthalmitis cases only demonstrated: mean LogMAR VA improved significantly from 2.68 to 1.66 (p=0.001). At final follow-up, 12% had VA of 6/12 or better, and 28% had VA of 6/36 or better. Vitrectomy within 7 days resulted in improved final VA outcomes (1.49 vs 2.16 LogMAR, p=0.032). Complications included retinal detachment (24.2%), macular hole (3%), hypotony (6%), suprachoroidal haemorrhage (3%) and enucleation/evisceration (6%).
Conclusion Vitrectomy for endophthalmitis leads to VA gains in some cases. Surgical outcomes may be improved with early vitrectomy performed within 7 days of the initial event for exogenous endophthalmitis. Patients should be advised of the potential risk of severe complications with/and without surgery.
- treatment surgery
- retina
- infection
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The Endophthalmitis Vitrectomy Study, published in 1995, concluded that vitrectomy achieves the best visual outcome for patients with perception of light vision or worse. Vitrectomy techniques have changed significantly over the last 24 years.
What are the new findings?
This study publishes the results that can be expected to be achieved with modern vitrectomy in a clinical practice with multiple causes for endophthalmitis. Vitrectomy for endophthalmitis leads to improved visual acuity gains in some cases, and early vitrectomy may give better outcomes.
How might these results change the focus of research or clinical practice?
These results help emphasise the importance of performing a new up-to-date randomised control trial into the surgical management of endophthalmitis. They also help set a benchmark by which other, similar, clinical practices can compare their results. They will help clinicians focus on considering early vitrectomy for endophthalmitis.
Introduction
Endophthalmitis is a devastating eye complication that may lead to blindness. Postoperative endophthalmitis (POE) is defined as an inflammation or infection of the intraocular space diagnosed within 6 weeks of surgery or any invasive procedure. The seminal study into the role of vitrectomy for post-cataract surgery endophthalmitis is the Endophthalmitis Vitrectomy Study (EVS) published in 1995. The conclusion of the EVS was that vitrectomy is of no benefit if the vision is better than perception of light (PL), namely hand motions (HMs) or better.1 Clinical practice for all types of endophthalmitis following intraocular surgery over the past 23 years has largely followed the EVS guidelines in the absence of other randomised control studies.
Vitrectomy surgery has changed significantly in the last decade with the introduction of small gauge surgery, wide-field viewing systems and the more frequent use of silicone oil: not used in the EVS study. In the EVS, only a 20-gauge core vitrectomy was permitted and performed compared with modern 23- and 25-gauge techniques where both a peripheral and core vitrectomy may be performed for POE. A 2005 study found 91% of patients achieving final VA of 6/122 where early small-gauge vitrectomy was performed on some patients with visual acuity (VA) better than PL. Other recent studies have demonstrated 75% with VA better than 6/12, 80% better than 6/18 and 40% better than 6/12 in the French Institutional Endophthalmitis Study (FRIENDS) study.3–5 These figures compare to 53% better than 6/12 in the EVS.1
These reported findings and a better understanding of the pathology of endophthalmitis have led clinicians to re-consider the role of early vitrectomy in endophthalmitis.6
Moorfields Eye Hospital sees, on average, 65 cases of suspected endophthalmitis per year, most of whom present via the emergency department. The emergency department serves patients in London and the south of England seeing over 100 000 patients per year.7 Given the large number of patients attending the emergency department, the causes of endophthalmitis seen are varied.8 Our study aims to review the changes in clinical practice at Moorfields over the past 5 years in the light of the EVS study, and we aim to study the contemporary role of vitrectomy in a wide range of real-world endophthalmitis presentations, reporting visual outcomes and complications.
Methods
This was a single-centre retrospective case series study. Patients who were eligible for the study included all patients who had undergone vitrectomy for endophthalmitis at Moorfields Eye Hospital over a 5-year period between 1 February 2013 and 1 February 2018. This cohort included endophthalmitis patients that failed to improve/worsened following medical therapy or had worsening vision despite medical therapy, and proceeded to vitrectomy. Cases were identified using our electronic patient record with external validation using medical records and the hospital infection control database. No vitrectomy patients were excluded from our analysis. Prior to study commencement, this study was registered with the Moorfields trust Audit office, code: CA17/Vitreoretinal/17. The study adhered to the tenets of the Declaration of Helsinki.
We used the FRIENDS 2016 study of vitrectomy in 123 patients with endophthalmitis to establish specific postoperative VA and complication standards to measure against our study outcomes. The FRIENDS standards included the following: 40% of patients having VA better than 20/40; 32% of patients having VA worse than 20/400; 13% of patients developing a retinal detachment complication after vitrectomy surgery and 8% of patients with no perception of light (NPL)/loss of eye.5
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics (Windows V.24.0, release 2016; IBM, Armonk, NY, USA) for descriptive and numerical statistical comparisons. The VA was converted from Snellen to LogMAR for analysis. Snellen counting fingers at 1 metre vision was converted to 1.87 LogMAR, Snellen HMs vision to 2.3 LogMAR1 and Snellen PL vision to 2.8 LogMAR. Means were compared with student’s t-tests and intergroup mean comparisons were analysed with analysis of variance (ANOVA). Correlation and linear regression were performed for continuous variables. A p value<0.05 was considered statistically significant.
Patient and public involvement statement
Patient involvement was not part of this study. The patients were part of a retrospective audit study, and the audit was approved by our Institutional Review Board at Moorfields.
Results
In all, 33 patients underwent vitrectomy for endophthalmitis between 1 February 2013 and 1 February 2018. This included 20 men and 13 women with an average age of 63 years. All patients underwent 23-gauge pars plana vitrectomy performed by either a consultant vitreoretinal surgeon or senior fellow. Average length of follow-up following vitrectomy was 18 (SD 14) months. The primary indication for vitrectomy surgery was therapeutic surgery in the acute inflammatory/infected phase for patients who did not improve/worsened with medical management. Patients would have the same vitrectomy surgery approach/procedure irrespective of the final indication to operate. There were a total of six cases of endogenous endophthalmitis that underwent vitrectomy which are analysed separately. Table 1 gives the breakdown of causes for endophthalmitis.
Breakdown of causes for endophthalmitis in all patients included in the study
Vitrectomy technique
The 23-gauge pars plana vitrectomy involved core and peripheral vitrectomy. In cases where the vitreous was partially detached, the surgeon would separate already detached vitreous but would not complete the Posterior vitreous detachment (PVD) due to the risk of creating iatrogenic retinal breaks. In cases with no PVD, the surgeon would perform a core vitrectomy and remove peripheral vitreous opacities and not induce a PVD. Vitreous base shaving was not performed for any of the cases. At the time of vitrectomy surgery, three patients had either an intraocular lens or glaucoma drainage device explanted. Three patients had a lensectomy, and three patients underwent anterior chamber washout. Anterior chamber washout was performed to improve the view for vitrectomy when required. Primary silicone oil tamponade was used in three patients.
VA outcomes
For exogenous endophthalmitis
Our audit standard results were as follows: 10.3% patients had VA better than 20/40; 58.6% patients had VA worse than 5/200 and 13.8% patients had NPL/loss of eye.
The mean LogMAR VA prior to vitrectomy was 2.7 (SD 0.31), and 20/27 patients had PL vision (74.1%). The mean LogMAR VA at 2 weeks post-vitrectomy was 1.85 (0.81 SD), and 5 (18.5%) patients had PL vision. The mean LogMAR VA improved significantly at final follow-up to 1.66 (SD 0.95, paired t-test, p=0.001), with a mean VA gain of 1.0 (SD 1.0) (figure 1). At final follow-up, two patients had PL vision and four patients had NPL vision. In all, 20 of the 27 patients (74%) patients had an improvement in VA following their vitrectomy, 8/27 (29.6%) had VA of 6/36 or better, and 3/27 (11.1%) patients had VA of 6/12 or better. Patients who started with PL vision gained 1.1 LogMAR while those with vision better than PL gained 0.7 LogMAR (one-way ANOVA, p=0.3): their final VA and VA at 2 weeks post-op were also not significantly different (one way ANOVAs, p=0.94 and p=0.57).
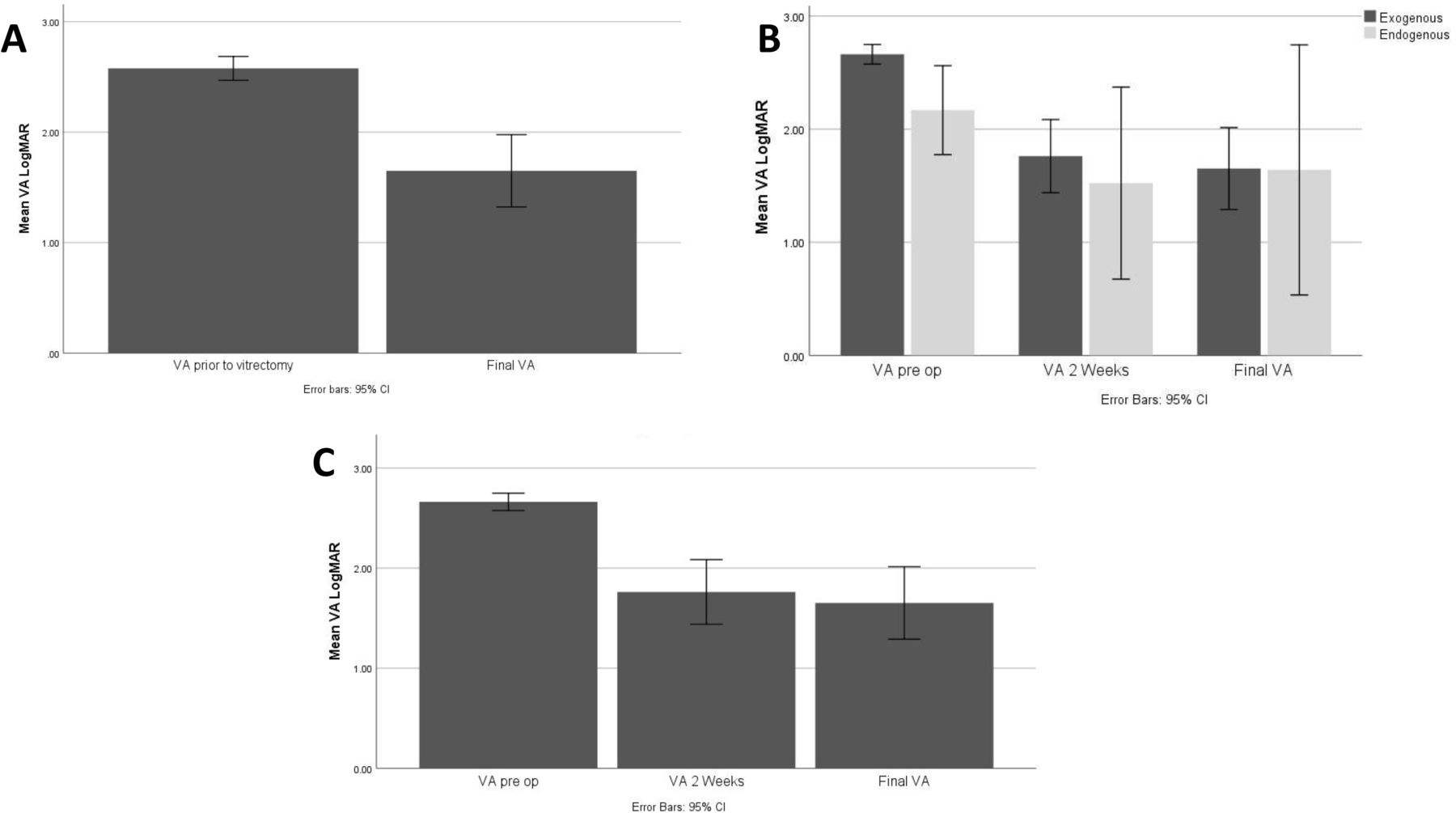
VA outcomes (a): bar chart comparing mean VA (LogMAR) before and after vitrectomy for whole group. Mean VA pre-op is 2.6 and significantly lower final VA at 1.65 (p=0.0001) (B): Cluster bar chart comparing visual outcomes of exogenous and endogenous causes of endophthalmitis. (C): Bar chart showing mean VA outcome for patients with exogenous endophthalmitis. Mean VA pre-op is 2.67 and significantly lower final VA at 1.65 (p=0.0001). VA, visual acuity.
For endogenous endophthalmitis
Our audit standard results were as follows: 16.7% patients had VA better than 20/40, 66.7% patients had VA worse than 5/200 and 16.7% patients had NPL/loss of eye.
The mean LogMAR VA prior to vitrectomy was 2.17 (SD 0.37), and 1/6 patients had PL vision (16.7%). The mean LogMAR VA at 2 weeks post-vitrectomy was 1.85 (0.81 SD), and 5 (18.5%) patients had PL vision. The mean LogMAR VA improved significantly at final follow-up to 1.52 (SD 0.81, paired t-test, p=0.017), with a mean VA gain of 0.52 (SD 0.77) (figure 1). At final follow-up, 0 patients had PL vision and 0 patients had NPL vision. Three out of six patients (50%) patients had an improvement in VA and two out of six patients remained unchanged (33.3%) following their vitrectomy, 2/6 (33.3%) had VA of 6/36 or better and 1/6 (16.7%) patients had VA of 6/12 or better.
Aetiology of infection
The causes of endophthalmitis and indications for vitrectomy are shown in table 2. A causative organism was cultured in 21/27 (77.8%) exogenous endophthalmitis patients: 48.1% (13/27) gram-positive bacteria, 29.6% (8/27) gram-negative bacteria and 22.2% (6/27) no growth. Of the endogenous patients, 50% (3/6) were positive for fungi and 50% (3/6) had no growth. There was no significant difference in VA gain between organismal groups (ANOVA, p=0.348).
A summary table of demonstrating the major patient characteristic and outcomes for all patients included in the study
In exogenous POE, the median time between the inducing operation and the diagnosis of endophthalmitis was 387 days (range: 1 day-19 years). There were significant improvements in vision in two subgroups of these eyes: (1) post-phacoemulsification group, the mean VA gain was LogMAR 0.77 (p=0.03) and (2) post-vitrectomy group, the mean VA gain was LogMAR 2.3 (p=0.012). In the post-intravitreal injection group (mean VA gain LogMAR 1.29 (p=0.061)), post-trabeculectomy (LogMAR 0.84 gain, p=0.133) and post-corneal graft (LogMAR 0.68 gain, p=0.292) subgroups, the improved levels of vision were not significant.
Intravitreal agents
A vitreous tap and injection (TI) of intravitreal antibiotics was delivered in 27/27 (100%) patients with exogenous endophthalmitis as part of the standard endophthalmitis protocol prior to vitrectomy surgery. 4/6 (66.7%) patients with endogenous received TI prior to vitrectomy. Our protocol for the management of endogenous endophthalmitis differs between whether the infection is suspected to be bacterial or fungal and, if fungal, whether there is vitreous involvement. With vitreous involvement in suspected fungal endophthalmitis, we proceed to vitrectomy within 48 hours and inject intravitreal amphotericin or voriconazole at the time of surgery rather in the emergency department on the day of presentation. 6/27 patients with exogenous had a total of two TI procedures. Patients that underwent a second TI gained significantly less vision (LogMAR 0.83 vs 1.05, two-sample t-test, p=0.003) and had significantly poorer final vision (LogMAR 1.96 vs 1.58, two-sample t-test, p=0.001) compared with patients that had one TI. There was no significant difference in timing of vitrectomy between those receiving one TI and those receiving two TI (6.86 days vs 11.83 days) (ANOVA, p=0.291). The antimicrobials injected prior to vitrectomy are shown in table 3 together with the antimicrobials injected at the time of vitrectomy. Three patients had intracameral tissue plasminogen activator injected at the time of their pre-vitrectomy intravitreal antibiotics due to severe fibrin in the anterior chamber. In addition to intravitreal antibiotics, all patients received oral antibiotic or antifungal therapy, mainly moxifloxacin or fluconazole, and oral steroids, except for in fungal cases.
Pharmacological agents injected prior, and during vitrectomy
Timing of vitrectomy surgery
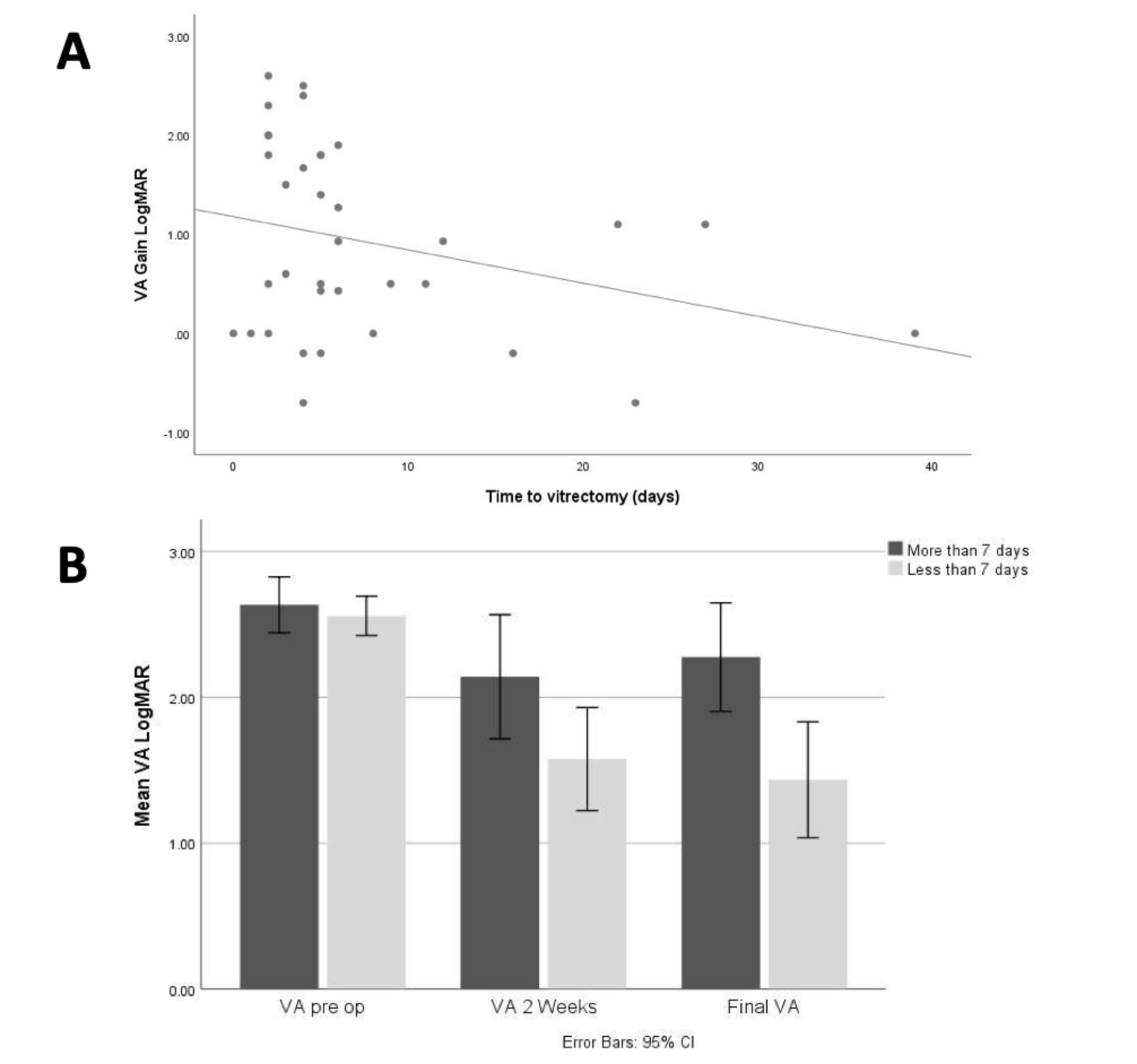
Mean time between diagnosis of endophthalmitis and vitrectomy was 8 days (median 5 days, range: 0–39 days). Delay in surgery was associated with less VA gain but this was not significant on regression analysis (p=0.112).
Table 4 and figure 2 summarise VA outcome data for those undergoing surgery in less than compared with more than 7 days. We concentrate on the results for 7 days, as although it is an arbitrary cut-off, it might represent what might be achievable in reality with the assessment and reassessment that is often required by the medical and surgical retinal teams. For patients with exogenous endophthalmitis, the final vision for patients having surgery at 7 days or less was significantly better at LogMAR 1.49 versus LogMAR 2.16 for patients having vitrectomy after 7 days (two sample t-test p=0.032). A similar change was found with separate analysis of the endogenous endophthalmitis cohort but this was not significant (table 4).
Summary of visual acuity outcomes in patients having surgery within 7 days or greater, from date of diagnosis

{kind=link}
{kind=link}
VA results and timing of vitrectomy surgery: (a) scatter plot showing distribution of VA gain for duration to vitrectomy in days. The best fit line shows downward trend of visual gain with delaying vitrectomy. (B) Cluster bar comparing VA between patients having vitrectomy 7 days or less CF. More than 7 days, there was a statistically significant difference for final visual outcome 1.43 (≤7 days) versus 2.27(>7 days) p=0.02. VA, visual acuity.
Complications
Our audit standard result was 24.2% developing retinal detachment post-vitrectomy (eight patients). Five patients had intraoperative iatrogenic retinal breaks (15.1%). Three patients required primary silicone oil tamponade and 5/8 patients underwent revisional surgery with resultant long-term silicone oil. Further complications included postoperative hypotony or choroidal effusions (n=3, 9%), postoperative macular hole (n=1, 3%) and suprachoroidal haemorrhage (n=1, 3%). Following primary vitrectomy surgery, additional surgical interventions included: enucleation (1/33), evisceration (1/33), lensectomy (1/33), laser peripheral iridotomy for iris bombé (1/33) and glaucoma drainage device insertion (1/33). There was no significant difference in rates of intraoperative complications based on organisms (Pearson’s χ2, p=0.267)).
Discussion
Despite, on average, 65 cases of endophthalmitis being seen at Moorfields per year only 33 went on to have vitrectomy over a 5-year period. This small number reflects how restricted the indications for vitrectomy are. The majority of patients who present with endophthalmitis either have a good response to intravitreal therapy, insufficient view for vitrectomy or have reached NPL vision so are not considered for vitrectomy surgery
In our experience of vitrectomy surgery for all types of acute endophthalmitis, patients with exogenous endophthalmitis may gain increased visual benefit when surgery is performed within 7 days. Surgery can, however, be associated with a range of intraoperative and postoperative complications (24% risk of retinal detachment and 6% risk of losing the eye).
The EVS found 33% of patients who underwent vitrectomy with PL vision had VA of 6/12 or better and 56% had VA better than 6/36 at final follow-up.1 63% of our patients had PL vision prior to their vitrectomy surgery with the remainder having better vision. 11% of our patients had VA better than 6/12 at final follow-up and 26% had VA better than 6/36. Our results are also worse than the FRIENDS standards as already described. There are a number of different potential reasons for our worse visual outcomes.
1: Compared with the FRIENDS cohort and EVS, in our study, the inciting operation included not only cataract surgery but also trabeculectomy, corneal transplant, glaucoma drainage device surgery, intravitreal injection and vitreoretinal surgery. The rate of sight-affecting comorbidities was therefore higher in our cohort.
2.The timing of vitrectomy in EVS was within 6 hours, and the median time to vitrectomy surgery was 2 days in FRIENDS. In our hospital, as in most UK eye centres, we do not have a protocol to perform early vitrectomy surgery meaning that our average delay between presentation and vitrectomy was 8 days. Although small numbers, we found favourable improvements in vision for early vitrectomy for endophthalmitis following cataract surgery, vitrectomy surgery, and post-intravitreal injection therapy.
We hypothesise that the timing of vitrectomy surgery is important because the intravitreal environment associated with the natural history of endophthalmitis alters over time. In the acute stages, there is mainly vitreous infective debris and opacification that responds well to vitrectomy surgery. In the subacute phase, starting from 7 days over several weeks, the endophthalmitis condition is associated with abnormal vitreoretinal adhesions and vitreoretinal traction can develop and worsen during this time. We believe that these factors can lead to complications despite the newer modern instrumentation. Our study reports that earlier vitrectomy surgery can lead to better visual outcomes. This may reflect the progression of the inflammatory vitreoretinal interface, retinal ischemia, retinal thinning, retinal breaks and preretinal fibrosis that can develop if surgery is delayed.
Other case series of vitrectomy in endophthalmitis that have been published since the EVS have demonstrated mixed visual outcomes and surgical complication rates. In their editorial, Kuhn et al demonstrate some of the best results, yet to be repeated, for 47 cases: no cases of postoperative retinal detachment, enucleation or phthisis and 91% of patients achieving a final VA better than 6/12.2 They have not, however, published preoperative VA and there was no specific VA threshold prior to vitrectomy. It is difficult to interpret their results without clear preoperative VA data. In 2012, Alamanjourmia et al reported on 10 patients who underwent vitrectomy on average 2 days following diagnosis of endophthalmitis.4 All patients had POE following cataract or filtration surgery, with a preoperative VA of HM or worse. Eight (80%) patients achieved final VA of 6/18 or better, with complications of retinal detachment (20%), hypotony (10%) and choroidal detachments (10%). In contrast to these good VA results, Behera and coworkers demonstrated 16% of cases achieved VA better than 6/36, in a study of 31 cases undergoing early vitrectomy for fungal endophthalmitis.9 Complications included phthisis (25.8%), retinal detachment (3.22%) and evisceration (3.22%). Ho and co-workers in Australia have recently reported on 64 postoperative endophthalmitis patients with entry VA of Counting fingers (CF) or worse, who underwent vitrectomy surgery within 72 hours.10 The median time to vitrectomy was same-day surgery as per the EVS, and better outcomes were achieved for patients with HM or PL vision. However, there were complications of retinal detachment (9%) and evisceration (3%).
There are a number of limitations with this study. We report a selective case series that underwent vitrectomy surgery with no control group so it is not possible to compare our outcomes with a similar cohort of patients with medical management only. Due to the case series nature of our study, we cannot completely discount confounding factors in our results. Although we have shown better results with earlier vitrectomy, we cannot discount the possibility that an eye that has shown little sign of improvement at 4 days and might still improve by seven or 8 days. Thus, the eyes having earlier vitrectomy might have done better than those having late vitrectomy regardless of whether or not they had a vitrectomy.
The wide diversity of aetiologies of endophthalmitis, which may be a reflection of our institution, should also be acknowledged as another potential source of confounding.
Although the diversity of aetiologies is a potential source of confounding, we think this study with its wide range of aetiologies is important. Intravitreal injections are the biggest treatment change in the past 10 years for age-related macular degeneration (AMD) and diabetic macular oedema (DMO). The incidence rates of POE vary between 0.038 and 0.053.11 12 In the EVS, patients were excluded based on pre-existing visual impairment secondary to other ocular conditions so benefits of contemporary early vitrectomy surgery in patients with POE with AMD and DMO cases remains unclear. In glaucoma, bleb-associated POE has a poor visual outcome; vitrectomy surgery in these cases has been shown to produce more favourable outcomes for patients.13
Due to the rarity of endophthalmitis, the numbers involved were not large enough for the regression analysis of delay in surgery to be significant (p=0.112) but there was a negative VA gain trend with increase delay in surgery (see figure 2). As the study was retrospective, it was designed largely to detect trends that could direct future research rather than powered for analysis.
EVS guidance of vitrectomy within 6 hours is not compatible with current intravitreal antibiotic treatment protocols for endophthalmitis in the UK. Good results are frequently obtained from the standard of care for endophthalmitis, intravitreal injections, so any future randomised clinical trial examining early vitrectomy for acute endophthalmitis should have medical therapy as the comparator control group.6
Acknowledgments
Support from the NIHR London Biomedical Research Centre is acknowledged. We would like to thank the Vitreoretinal, Medical Retina and Uveitis Services at Moorfields Eye Hospital for their support in patient management during the study period.
Footnotes
Contributors Study design, planning, conduct, analysis of data and reporting of work: GN, WOC, CP, MMMK. We confirm that GN and MMMK are responsible for the overall content as guarantors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
↵Logarithm of the Minimum Angle of Resolution