Article Text

Abstract
In addition to catastrophic loss of life, and dramatic and unwanted alterations to the daily lives of those left behind, the COVID-19 pandemic has fostered the publication and dissemination of an unprecedented quantity of peer-reviewed medical and scientific publications on a single subject. In particular, the ophthalmic literature is now replete with clinical and laboratory studies on putative eye involvement by SARS-CoV-2, the aetiologic agent of COVID-19. In this review, we critically appraise the published literature on COVID-19, and suggest that the quality of scientific peer review and editorial decision-making also suffered during the COVID-19 pandemic.
- COVID-19
- conjunctiva
- cornea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
During the COVID-19 pandemic, the ophthalmic literature has been inundated with studies examining the role of SARS-CoV-2 in precipitating ocular disease. Such interest has been prompted by ongoing uncertainties regarding the basic biology and transmission dynamics of this new pathogen. However, the COVID-19 literature as it pertains to the eye also offers a parable for how modern structures of scientific inquiry—including peer review and editorial oversight—may falter when presented with newly observed phenomena, particularly one resulting in large numbers of deaths. At issue is the conception of ‘alternative facts’1 2 during a time of profound global anxiety, arising due to misinterpretations or overinterpretations of data that may nevertheless gain lasting traction within the popular press and community at large. This essay, written for the 2022 David L. Easty lecture, offers a critical appraisal of the many circulating ‘alternative facts’ concerning COVID-19 and the eye. Key debates include the true breadth of ocular manifestations of SARS-CoV-2 infection, the replicative potential of SARS-CoV-2 within ocular surface epithelia, and the risk of viral transmission through ocular secretions. To extent these questions will shape future eye care, including corneal transplantation in particular, they are also germane to the legacy of Dr. Easty, whose distinguished achievements as a corneal physician and ophthalmic virologist include establishing the UK National Eye Research Center (now Save Sight UK) and the UK’s first nationwide corneal transplant service, both in 1986.3 In keeping with the principles of evidence-based medicine, this essay highlights the methodological limitations that have been frequently overlooked in the ophthalmic COVID-19 literature, including flawed study designs, failures to recognise and minimise systematic biases, particularly confounding and erroneous conflations of association as causation. Failing to account for such limitations—and their resulting ‘alternative facts’—represents a departure from the high scientific standards required to direct clinical practice and public health during this global emergency.
‘Alternative facts’ in historical context
An unfortunate revelation of the COVID-19 pandemic has been the ease at which inaccurate information—whether intentional and malicious (‘disinformation’), or unintentional yet still potentially harmful (‘misinformation’)—has thwarted efforts to suppress community transmission, establish evidence-based clinical guidelines, and to understand SARS-CoV-2 biology.4 5 The strains of pandemic misinformation, recently described by the WHO as the COVID-19 ‘Infodemic’,6 have been felt most prominently in highly contentious debates surrounding the origins of SARS-CoV-2,7–9 vaccine hesitancy,10 mask refusal,11 and the safe reopening of public venues.12 13 The many harms of misinformation (figure 1) mean that those tasked with knowledge production during crises, including physicians, epidemiologists and basic scientists, have a unique responsibility to maintain the highest evidence-based standards to guide public health measures and the care of patients. Yet, the perceived need for expedited research during the pandemic has in some cases come at the expense of scientific rigour. A case–control study of over 500 COVID-19 articles matched to an equal number of historical controls from the same high impact-factor journals found that the median time from submission to acceptance was an astonishing 13.0 (IQR 5.0–25.0) days compared with 110.0 (71.0–156.0) days, respectively.14 It is almost inconceivable that such a discrepancy would not be associated to some degree with the reductions in peer review and editorial stringencies. Our exposition of ‘alternative facts’ and illusory causation in eye disease associated with COVID-19 is not intended as criticism, nor do we wish to conflate the absence of evidence as evidence of absence. Rather, the analysis is intended to emphasise the principles of sound evidence-based science, and to reconcile cognitive biases to which no clinician is immune.
Major harms of ‘alternative facts’ in biomedical discourse. Figure created using BioRender.com on a standard academic license.
Does SARS-CoV-2 cause ocular disease?
Causal inference in ophthalmology
A major focus of recent ophthalmic research has sought to determine whether SARS-CoV-2 is causally associated with ocular disease, including infectious,15–19 inflammatory,20–26 coagulopathic,27–32 and neuro-ophthalmic33–35 pathologies involving virtually every structure of the eye. However, the definition of ‘cause’ remains a source of confusion, and is used with less than optimal restraint. The identification of causal associations36–38 from any clinical data require, at minimum: (a) well-defined exposures and outcomes,39 without which ‘cases’ cannot be identified, and without which the underlying study population cannot be determined;40 (b) temporality, where the exposure of interest must precede the outcome41; and (c) freedom from systematic error, including confounding and selection bias.42–44 Such biases are encoded in directed acyclic graphs (figure 2) that illustrate the causal structure for prototypical study designs, thereby helping visualise biases that threaten the internal validity of any study.45 46 Confounding arises as a result of factors that act as mutual causes of both the exposure and outcome of interest, distorting the true exposure effect and thus leading to misattribution of causality. Selection bias occurs when a parameter of interest—for instance, effect measures such as risk and odds ratios—for an underlying population is not equivalent to the quantity obtained from data containing a subset of the same population, and most frequently arises when individuals are preferentially enrolled into studies according to exposure and/or outcome status.47 Randomised controlled trials (RCTs) maintain a privileged position in the hierarchy of clinical evidence because by design, random treatment (exposure) assignment minimises the potential for confounding and selection bias (figure 2A). That is, in an intention-to-treat analysis of an RCT with double-blinding, no losses to follow-up, and perfect adherence, association is causation. However, because it would be unethical to conduct a trial wherein participants are randomly assigned to a harmful exposure (eg, SARS-CoV-2), observational studies are often the only method of addressing causal questions in clinical medicine and epidemiology. Unfortunately, some studies in the ophthalmic COVID-19 literature have disregarded the fundamental requirements for causal inference, leading to spurious associations that masquerade as ‘causal’ in nature, leading to propagation of ‘alternative facts’.
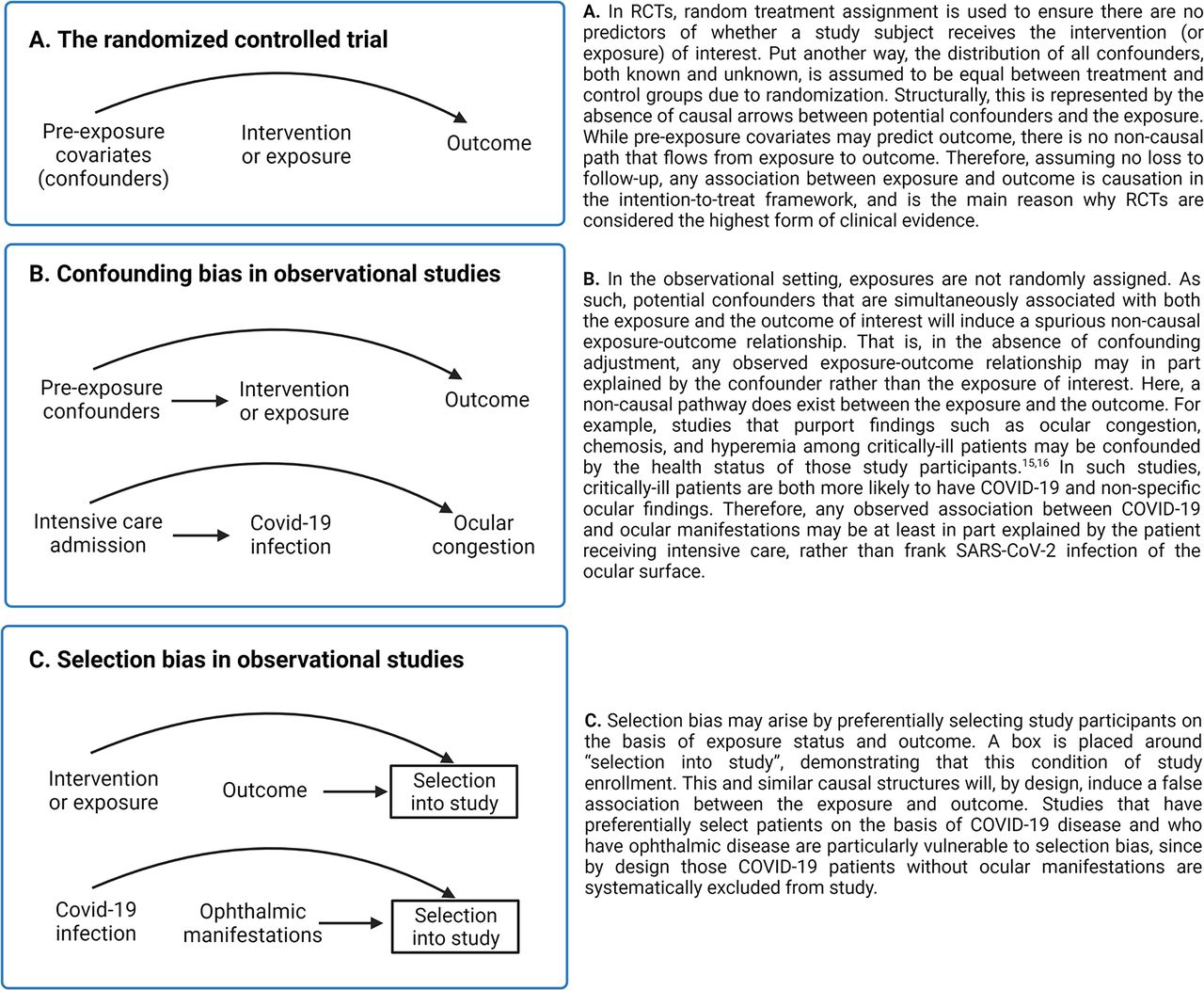
Directed acyclic graphs (DAGs) highlighting key sources of bias in clinical and epidemiologic studies. (A) An ideal randomised clinical controlled trial, marked by a complete absence of confounding within an intention-to-treat framework; (B) classic confounding in an observational study; and (C) selection bias in an observational study. Confounding and selection bias are threats to study validity, and if present, will bias both descriptive (eg, prevalence and incidence) and effect measures (eg, risk and odds ratios).169 All DAGs have been drawn under the null hypothesis, and examples from the COVID-19 literature in ophthalmology have been referenced. The flow of association is depicted by the presence of causal arrows between nodes. Further details on DAGs and structural representations of study biases may be found in Hernan and Robins (2020).170 Figure created using BioRender.com on a standard academic license.
Association between COVID-19 and ocular infection
While SARS-CoV-2 may cause an acute and self-limiting follicular conjunctivitis,48 similar to that caused by its relatives SARS-CoV49 and HCoV-NL63,50 quantifying the true frequency with which conjunctivitis occurs among patients with COVID-19 remains fraught with difficulty. Case series have reported the prevalence of conjunctivitis among the COVID-19 infected as ranging from 1% to 55%.15–17 51–53 However, making sense of such a wide spectrum of values requires several considerations. First, one must reconcile the application of varying clinical (eg, fever and dyspnoea), radiologic (eg, findings on CT), and laboratory (eg, real-time (RT)-PCR) criteria used to define COVID-19 infection. Some studies15 16 have not required the most stringent test—a positive RT-PCR—as a condition for cohort entry. One must also consider whether the setting of patient recruitment (eg, hospitalised vs non-hospitalised), severity of infection, and asymptomatic transmission (likely exceeding a third of all cases54 55) may ultimately render the study participants non-representative of the underlying COVID-19 population. Descriptive epidemiology, much less causal inference, cannot be conducted without explicitly defining the population denominator. Second, loosely applied definitions for conjunctivitis—including congestion, chemosis, hyperemia and secretions,16 51 56 and less commonly conjunctival haemorrhage57 and pseudomembrane formation58—should invite considerations of outcome misclassification, particularly if observed among severely ill patients and/or if ascertained retroactively.59 Finally, as described earlier, drawing causal inferences requires freedom from structural biases such as confounding that could in part explain the observed association(s). Systematic reviews and meta-analyses60 61 that do not consider such methodological constraints are vulnerable to misinterpretation.
In one of the earliest studies on COVID-19 ocular surface infection, now cited over 1000 times, Wu et al reported 12 of 38 hospitalised patients (32%) who developed features ‘consistent’ with conjunctivitis, chiefly chemosis, secretions, epiphora, and hyperemia.16 All cases occurred among the moderate-to-critically ill, and only 3 of 38 (8%) patients had hyperemia, itself insufficient to define conjunctivitis. The report did not provide any data from the underlying study population that gave rise to cases, thereby giving no sense of the relative frequency at which these conjunctival findings were observed in comparable controls without COVID-19. Furthermore, the results were also almost certainly confounded owing to extraneous predictors of both COVID-19 illness and clinically diagnosed ‘conjunctivitis’ (figure 2B). Subsequent commentaries published in the wake of the study correctly noted that mechanical ventilation, fluid overload and third-spacing, pre-existing eye conditions, and ocular surface compromise (eg, exposure keratopathy) are common reasons for chemosis, epiphora and even hyperemia among severely ill patients.62 63 The confluence of these methodological limitations—since recapitulated in other studies15 52 64–66—has nonetheless created the impression that conjunctivitis will manifest in an implausibly large proportion (>30%) of patients with COVID-19. Large population studies have reported a far lower prevalence (<1%) of laboratory-confirmed patients with COVID-19 developing, at most, ‘conjunctival congestion’.51 67 This finding would imply that perhaps an even lower proportion would have frank conjunctivitis caused by SARS-CoV-2 replication within ocular surface epithelia, and conversely that SARS-CoV-2 is likely an uncommon aetiology of conjunctivitis cases that present for care.68 Despite this, numerous studies have ascribed conjunctivitis as an independent predictor of COVID-19 clinical course, including mortality,64 69 based on observations almost certainly subject to confounding and selection bias.
The association between COVID-19 and other ocular infections, including keratoconjunctivitis,70 71 epithelial keratitis,72 reactivation of herpes simplex keratitis and herpes zoster73–75 and endophthalmitis,19 are currently limited to unconfirmed case reports that cannot be interpreted causally. For instance, a study presented at the 2020 American Academy of Ophthalmology meeting reported three patients with COVID-19 with infectious keratitis, and which progressed to endophthalmitis, proposing a possible causal association between COVID-19 and infectious keratitis progressing to endophthalmitis.19 However, patients were preferentially enrolled into the study on the basis of their exposure (COVID-19), and also their development of the outcome (endophthalmitis), and so by design the study induced a false exposure–outcome relationship (figures 2C and 3) owing to selection bias. Unmeasured confounders, such as patient comorbidities, may have also introduced bias had there been factors predictive of both COVID-19 infection and endophthalmitis.

{kind=link}
{kind=link}
{kind=link}
Selection bias in epidemiologic and clinical studies. Selection bias may result in a distortion of descriptive and/or effect measures obtained in a study population, compared with that of the larger population that gave rise to the cases.171 Figure created using BioRender.com on a standard academic license.
Retinal manifestations of COVID-19
In another cautionary tale, we next consider the recent controversy surrounding the possible retinal manifestations of COVID-19. In a widely cited imaging study, Marinho et al reported the presence of hyperintense lesions within the ganglion cell layer in 12 patients imaged with optical coherence tomography, 4 of whom were also reported to have developed cotton wool spots (retinal infarcts) and microhaemorrhages on fundus examination and photography.76 However, the study did not provide any detail of the underlying study population that gave rise to the cases—for instance, the total patients who underwent funduscopy—nor how the study population was selected. Sampling inadequacies aside, the study proposed a causal association between COVID-19 and retinal disease using cross-sectional data that could not determine whether SARS-CoV-2 exposure had preceded the retinal lesions. Even more problematic was the attribution of these perceived imaging abnormalities to SARS-CoV-2, a hypothesis that came under severe scrutiny by several independent groups who suggested that the retinal hyperintensities represented normal retinal vessels given their stereotypical calibre, tube-like morphology, and dorsal shadowing.77–80 Furthermore, no attempt was made at the time of publication to report patient comorbidities that could have confounded the association between COVID-19 infection and observed microangiopathic changes. It was later revealed in an authors’ response that five patients had known cardiovascular comorbidities, including diabetes mellitus, hypertension and dyslipidaemia.81 While it is certainly possible that COVID-19 may result in retinal manifestations,82 the results in this study were likely misinterpretations of what were later deemed to be either normal visualisations of the retinal vasculature or features easily attributable to underlying chronic disease.
Eyeglass-wear duration and COVID-19 infection
Not infrequently, published studies have suffered from both intractable confounding and selection bias. Consider the case–control study by Zeng et al, which evaluated the association between duration of eyeglass-wear and risk of COVID-19.83 The study compared 276 hospitalised patients with laboratory-confirmed COVID-19 to historical controls sourced from data published over three decades earlier. The authors found the proportion of patients who self-reported wearing eyeglasses for ≥8 hours per day was 5.8% among cases and 31.5% among controls, suggesting that prolonged eyeglass wear was associated with a decreased susceptibility to COVID-19 infection. However, limitations in study design should temper this conclusion. Patient controls were selected from a convenience sample that almost certainly differed from cases with respect to demographic features, comorbid status, and other unmeasured factors, given the aged nature of the data (figure 3). This invalid sampling scheme led to the enrolment of controls who did not represent the same study population that gave rise to the cases, a telltale sign of selection bias.84 Furthermore, there are many plausible scenarios where an unmeasured pre-exposure covariate could confuse the true effect of the exposure on the outcome. For instance, socioeconomic status could conceivably influence one’s ownership of eyeglasses as well as their susceptibility to COVID-19, and its unaccounted presence in these data would confound the protective effect of prolonged daily eyeglass wear against COVID-19 infection. While several commentaries advised caution in interpreting the results, most discussion of the study’s limitations focused on the hindrances inherent in data from a single centre with a small sample size.85 86 Yet, the underlying design of this study would have produced invariably biased results, regardless of the scale at which it was conducted.
Does SARS-CoV-2 replicate in ocular surface epithelia?
Corroborating laboratory evidence thought to show that SARS-CoV-2 infects ocular surface epithelia has now been published by many groups, using a combination of approaches including: RT-PCR analyses on ocular samples (eg, tears, swabs and cadaveric eyes); determining the ocular surface tropisms of SARS-CoV-2 by analysing the expression of cell surface receptors, including angiotensin converting enzyme-2 (ACE2) and type 2 transmembrane serine protease (TMPRSS2), among other secondary proteins; and in models of infection within human cell lines and animals. However, the evidence to support SARS-CoV-2 infection of ocular surface epithelia is far thinner than generally appreciated, with interpretations of results impacted by neglecting the limits of biological plausibility, absence of control data, and doubtful transportability assumptions between the wet bench and the dynamics of infection in real-world settings. Such limitations become clearer by specifying the model of live human infection that would most accurately describe active SARS-CoV-2 replication within ocular surface epithelia: (a) exposure of ocular surface epithelia to SARS-CoV-2, either by aerosols and/or by direct contact; (b) evasion of robust ocular surface protections, including mechanical (eg, tear washout) and chemical (eg, mucosal immunoglobulins, complement and antimicrobial peptides)87 defences; and (c) attachment to, invasion of, and replication within ocular surface epithelia, resulting in pathognomonic cytopathic effect.
PCR analysis of ocular surface samples
Possible ocular surface tropisms of SARS-CoV-2 have been studied most commonly via RT-PCR analyses of ocular samples, including conjunctival swabbing and tears. The proportion of patients with COVID-19 who have returned positive RT-PCR tests from the ocular surface has ranged from 0% to 57%,16 88–98 with the large range of values attributable once again to differences in sampling fractions, highly variable case definitions for both COVID-19 and ‘conjunctivitis’, and test collection methods employed (including live vs postmortem testing).99 Furthermore, results may also be contingent on the testing laboratory, since clinical laboratories are often subject to different regulatory requirements regarding validation and limits of detection than when compared with research laboratories.100 Correctly interpreting RT-PCR tests also requires nuance and understanding of the methodology to avoid misinterpretation. RT-PCR of any surface only tests for the presence of the nucleic acid, and does not necessarily indicate infectious virus. That is, RT-PCR cannot confirm whether the viral RNA discovered represents intact virus capable of replication, for example, in the preocular tear film, or whether there is actual viral replication in ocular surface epithelium. SARS-CoV-2 RNA has been identified by RT-PCR on windowsills, air vents, bedrails and shoes,101 102 and no one would suggest the virus is replicating on these acellular, nonliving surfaces. Therefore, detecting SARS-CoV-2 RNA on the eye surface by RT-PCR may be no more significant than finding the RNA on the same person’s shoes. Rather, positive tests merely provide an indication that viral RNA has been recovered from the sampled area, and neither its source nor viability can be determined with certainty. Likewise, negative tests should not be construed as definitive absence of virus, since false-negatives may arise due to poor collection technique, the clinical window in which sampling occurred, and the potential need for repeated collection.100 103
Clinical correlations between conjunctivitis and a positive conjunctival RT-PCR test remain poor at best. For example, Azzolini et al conducted a cross-sectional study on 91 hospitalised patients with COVID-19 (confirmed on nasopharyngeal RT-PCR), reporting that among 52 (57%) patients whose conjunctiva tested positive, only 3 (6%) had conjunctival hyperemia and 3 (6%) had ocular ‘secretions’.104 The authors quite correctly suggested that viral RNA detected from the ocular surface could have been sourced elsewhere, for instance from the aerosolised microenvironment around the face (particularly patients on mechanical ventilation), or from the lacrimal glands or ocular surface vasculature in the setting of systemic infection and viremia. To date, only one report has provided evidence of infectious virus—not just RNA—directly isolated from the conjunctiva of a patient with COVID-19. Colavita et al reported the case of a 65-year-old patient with laboratory-confirmed COVID-19, who presented with fever, mild upper respiratory symptoms, and bilateral conjunctival hyperemia and chemosis.105 The authors took a conjunctival swab on day 3 of hospitalisation, and inoculated its contents within Vero E6 kidney epithelial cells, observing viral cytopathic effects 5 days later. Concurrently, viral RNA was isolated from spent cell media using RT-PCR, along with positive RT-PCR tests on ocular swabs collected throughout hospitalisation. While this report provides a compelling account of in vitro SARS-CoV-2 infectivity, the authors did not perform PCR for other viruses. Furthermore, the cytopathic effect observed in cell culture after inoculation by the clinical sample could not be definitively attributed to SARS-CoV-2, as immunodetection assays, including those testing for antigens of other viruses, were not performed.
Ocular surface tropisms of SARS-CoV-2
It is well-established that the two canonical transmembrane receptors for SARS-CoV-2 infection in human epithelial cells are ACE-2 and TMPRSS2.106–112 ACE-2 serves as a direct viral binding site, while TMPRSS2 is involved in cleaving the SARS-CoV-2 spike (S) protein at S1/S2 and S2, thereby priming the virus for cellular entry. Whether the ocular surface epithelium expresses co-localised ACE-2 and TMPRSS2 in the requisite quantities to permit routine SARS-CoV-2 infection remains controversial, with divergent perspectives captured by studies reporting both high111 113–119 to essentially negligible120 121 expression of these proteins. Furthermore, it is not known whether the expression of these receptors may vary with various health states (eg, systemic COVID-19 infection vs non-infection), with pre-existing eye disease, or in the setting of comorbidities where ACE-2 plays a pathophysiological role (eg, cardiovascular disease). There is some limited evidence to suggest that ACE-2 and TMPRSS2 may be localised to ocular surface tissues. In one such study where immunohistochemistry was performed on postmortem surgical specimens from healthy individuals, Zhou et al demonstrated diffuse presence of ACE-2 and TMPRSS2 in corneal and conjunctival epithelia.113 Curiously, however, ACE-2 staining was far more prominent within the basal corneal epithelium relative to the outermost apical layers, with this staining asymmetry most pronounced at the corneal limbus. Furthermore, while the authors showed putative ACE-2 expression within conjunctival crypts, it was not clear whether the isotype control captured the same conjunctival crypts shown with the primary antibody.
Data on whether SARS-CoV-2 can infect ocular surface epithelium also remain sparse, even under ideal experimental conditions. In one immunohistochemistry study of ex vivo human conjunctival explant cultures by Hui et al, a clinical SARS-CoV-2 isolate was used to inoculate three human conjunctival explant cultures, with an exponential rise in viral titers 48 hours post infection (hpi) strongly suggestive of infection.122 However, when anti-SARS-CoV-2 nucleoprotein was used to stain the conjunctival specimens at 48 hpi, viral antigen appeared only within the conjunctival substantia propria, and not in the epithelium. This may be because explant cultures lack a confluent epithelial barrier—virus in the culture media bathes and can access cells within the tissue from any side, including the stromal side of the explant. In another ex vivo human explant study, Miner et al showed that a clinical isolate of SARS-CoV-2 did not replicate within human corneal donor tissue recovered from seven non-COVID-19 infected patients, confirmed using serial RT-PCR and plaque assays, and as compared with a positive control using HSV-1 to infect the same specimens.123 Furthermore, the authors reported that SARS-CoV-2 did not replicate in the residual conjunctival and limbal tissue that remained attached to the explanted corneas. Unsurprisingly, there is similarly conflicting evidence as to whether SARS-CoV-2 can be detected from human donor corneas retrieved from patients known to be COVID-19 positive at the time of death. One immunohistochemical study by Sawant et al reported SARS-CoV-2 spike and envelope protein in the epithelium of three donor corneas that had not undergone disinfection with povidone-iodine.124 Meanwhile, RT-PCR analyses from independent groups did not identify SARS-CoV-2 RNA from iodine-disinfected donor corneas.125 126
The ocular surface as a passive conduit to nasopharyngeal SARS-CoV-2 infection
Consideration of the ocular surface as both contagion and anatomical conduit has naturally invited speculation that nasopharyngeal SARS-CoV-2 infection may occur through the nasolacrimal system.127 128 This theory came to prominence early during the pandemic, when Dr Wang Guangfa, a distinguished SARS expert, developed COVID-19 after visiting a Wuhan hospital in January 2020.129 Having worn a personal protective gown and an N95 mask, Dr Wang attributed his infection to a lack of protective eyewear, recalling bilateral conjunctival congestion prior to the onset of respiratory symptoms. While other respiratory viruses such as human and avian influenza can cause systemic illness130–132 following conjunctival inoculation, whether the same can be concluded for SARS-CoV-2 remains unclear. Deng et al applied a relatively large inoculum (106 TCID50/mL) of SARS-CoV-2 to the conjunctival surfaces of two rhesus macaques, and reported that both animals developed mild COVID-19 respiratory symptoms, with a continuously detectable viral load sourced from nasopharyngeal and oropharyngeal swabs up to 7 days post inoculation.127 However, virus could not be detected from conjunctival swabs after 1 day post inoculation. Histology was not performed on the conjunctiva at euthanasia, but the repeatedly negative RT-PCR results from conjunctival swabs after 24 hpi suggests ocular surface infection did not occur.
In sum, clarity around ocular involvement in COVID-19 is lacking. Experimental studies have either not been confirmed or would be difficult to reproduce, and existing data do not lend the sort of overwhelming support for ocular surface infection that has been suggested by some retrospective clinical studies. Rather, the weight of current evidence supports a limited role for the ocular surface in viral shedding and transmission. Questions remain regarding how routinely SARS-CoV-2 (and its variants133) infects ocular surface epithelia as compared with other vulnerable cell types (eg, nasopharyngeal epithelia), whether the conjunctival and corneal epithelium may have different susceptibility profiles (eg, due to discordant expressions of cell surface proteins required for viral entry) and the potential for viral carriage and infectivity within the eye among recovered patients.134 135 Furthermore, ex vivo models may not fully capture the real-world viral kinetics on the ocular surface, including the protective effects of the tear film and adnexa.136
Alternative facts: what is to be done?
Implications for ophthalmology: the case of corneal transplantation
Far from being an esoteric academic exercise, the prompt recognition of ‘alternative facts’ derived from faulty study design and/or misinterpretations of data—around which expert consensus may coalesce—is of enormous clinical and public health importance. It would not be unreasonable to suggest that the evidence base concerning COVID-19 and the eye may have a long-lasting impact on the global state of corneal transplantation, principally owing to fears of donor-to-recipient SARS-CoV-2 transmission. As of March 2022, guidelines from the Eye Bank Association of America (EBAA) exclude from the donor pool any patient with known or suspected COVID-19 within 10 days preceding death, defined by a positive RT-PCR or antigen test, receipt of treatment for COVID-19, and/or a history of close contact.137 The European Eye Bank Association (EEBA),138 and the Global Alliance of Eye Bank Associations (GAEBA) 139 have issued similar guidance to exclude potential donors diagnosed with COVID-19 in a 14 day window prior to death. These recommendations are less conservative than those that were released last year, where the same agencies required eligible COVID-19 donors to be at least 28 days removed from their last positive RT-PCR test and/or the resolution of COVID-19 symptoms. On the other hand, the US Food and Drug Administration (FDA) as recently as January 2021 affirmed that the risk of respiratory virus transmission via transplantation of human cells and/or tissues is negligible, with no known cases of donor-transmitted COVID-19.140 The US FDA has issued general guidance recommending against screening asymptomatic potential donors, leaving this decision to the discretion of individual tissue banking agencies.
The risks of donor–recipient transmission, of course, must be weighed against the profound human, social, and economic costs associated with corneal blindness. An estimated 13 million persons globally are in need of corneal transplantation,141 and the greatest disparities in access to this sight-restoring procedure exist in low-to-middle-income countries.142 143 Corneal transplantation ground to a virtual halt during the first global lockdowns in February–March of 2020,144 145 and the EBAA estimates that over the entire year there was a ≈20% reduction in tissue procurement (54 740 donors in 2020, compared with 68 759 in 2019) and in corneal transplantations (108 382, compared with 136 130 the year before).146 Moreover, corneal transplants outside the USA decreased from 28 402 to 16 123, representing a reduction of over 40% of procedures performed in countries that generally rely on donor cornea importation from surplus eye banks. With an already low proportion (~2%147) of EBAA-eligible US donors who eventually undergo tissue recovery, continued COVID-19-related restrictions on donor eligibility will reduce an already slim donor pool. Currently, EBAA regulations state that while some viral infections are absolute contraindications to donation (eg, HIV, hepatitis B virus, hepatitis C virus, herpes simplex virus type 1/2), others such as cytomegalovirus, adenovirus and influenza are not. As Desautels et al note,147 it would not be unprecedented for patients who succumb to non-septic complications of a respiratory virus—for instance influenza, which has confirmed ocular tropisms148—to remain donor eligible, given the rarity of donor–recipient transmission with appropriate disinfection measures. To date, out of eight known cases of corneal transplantation in which the donor tissue came from persons later identified to have had COVID-19, only one recipient later developed COVID-19. On investigation, this single case of putative donor-to-recipient infection was later attributed to community transmission rather than from the donor cornea.149
The question of whether SARS-CoV-2 can be transmitted through donor corneal tissue is therefore one of urgent clinical equipoise. Whether by putting donor recipients at risk of COVID-19 through corneal transplantation, or conversely, by needless wasting of otherwise viable and desperately needed corneal tissue, the public health significance is broad and the margin for error narrow. Therefore, high-quality studies are required to: (a) elucidate the biological mechanisms and true frequency of ocular surface infection caused by SARS-CoV-2; (b) determine whether virus is reliably inactivated by topical applications before donor harvest, for example, with povidone-iodine150 151 or polyvinylpyrrolidone152 153 (and including whether subepithelial layers would be protected by such treatments); (c) provide guidance on donor screening, for example, with universal or risk-stratified testing149; and (d) establish evidence-based guidelines for how to accurately distinguish, using PCR-based testing or otherwise, between the shedding of replicating virus versus presence of non-infectious RNA fragments.134
Alternative facts: the role of cognitive biases
While insights drawn in the fog of a pandemic may be subject to question, the processes that govern the genesis of medical and scientific ‘facts’ justify further scholarship. Facts are generated by complex human processes that reflect our innate desire to understand the world around us, but they also reflect both our cognitive biases and the social conditions of our time. Therefore, while the apparent lowering of research standards both before154 155 and during156 157 the pandemic remains a topic of keen discussion, the question of why misinterpretations of data have become so commonplace is also critically important for the future of science. The development of evidence-based medicine was in part a reaction to the many internal heuristics and narrative-based practices158 felt to sway care guidelines from what evidence would posit as the most appropriate course of action.159
Arguably, the crush of opportunistic and lesser quality publications during the pandemic has been fueled by cognitive errors magnified by a deep global anxiety. Cognitive biases now riddle the entire COVID-19 corpus, appealing to automated and instantaneous systems of human judgement—a euphemism for mental ‘shortcuts’160—rather than the typically slow but often well-reasoned nature of traditional peer review.161 For example, confirmation bias has been evident in most examples presented above, where one is far likelier to accept the results of studies that accord with their own beliefs, while remaining inattentive to methodological flaws or omissions that might otherwise temper conclusions.162 163 The availability heuristic, which amplifies one’s perception of how probable an event is according to how quickly and/or vividly a relevant experience is recalled,164 may explain part of the tendency to erroneously describe COVID-19 disease manifestations in causal terms. Anchoring bias, where judgments are made on the basis of pre-existing and often minimal data,165 may explain why ‘conjunctival congestion’ has been so often reported as caused by SARS-CoV-2 infection rather than more common causes, particularly in critically-ill patients. These examples are only three of many evident in the COVID-19 literature (table 1).166 167 Existing systems of expedited yet rigorous, multistage peer review have not therefore protected us against misinformation. Clearly, finding evidence-based strategies to recognise cognitive biases within medical and scientific discourse are needed to prevent overinterpretation of flawed study designs and imprecise research findings.
Common cognitive biases evident in the ophthalmic COVID-19 literature, and more broadly in the biomedical sciences
Conclusion
In a November 1710 edition of British newspaper ‘The Examiner’, satirist and editor Jonathan Swift cautioned, ‘Falsehood flies, and the truth comes limping after it’.168 Contrary to what may be suggested by the volume and pace at which studies are being published, this essay offers a sobering assessment of how truly little is known about COVID-19 and the eye. Expedited throughput of submitted manuscripts, reduced stringency in peer review and editorial oversight, and the apprehensive reader’s willingness to accept the literature on COVID-19 with less than a critical eye have all led to the proliferation of ‘alternative facts’ without qualification. Common errors have included drawing causal inferences in clinical and epidemiologic studies that may not permit such conclusions, owing to reasons such as poor study design, confounding, and selection bias. Basic laboratory research has suffered from overinterpretations that stretch the limits of biological plausibility, may lack appropriate controls, and rest on doubtful assertions of model generalisability to real-world settings. The central theme of this essay is, categorically, not to call into question the scientific underpinnings of current mitigation strategies to decrease community transmission of SARS-CoV-2. Rather, in light of our duty of care to patients and the wider public, the highest standards of scientific rigour must be preserved. Only the most robust forms of evidence should inform our behaviour during this global emergency. The potential harms from misinformation demand no less.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors wish to acknowledge Dr David W. Parke II, MD, and the American Academy of Ophthalmology for their tireless work on behalf of patients, staff, and ophthalmologists during the COVID-19 pandemic.
References
Footnotes
Contributors JC conceived the project. LU wrote the first draft and contributed the figures and table. Both authors closely collaborated on the final version.
Funding Supported in part by an unrestricted grant to the Department of Ophthalmology, Harvard Medical School, from Research to Prevent Blindness, NY, NY; and by the Dozoretz Family Private Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.