Article Text

Abstract
Objective To assess agreement and repeatability of white-to-white (WTW) and anterior chamber depth (ACD), and agreement of implantable collamer lens (ICL) size using these measurements from different devices.
Methods and analysis A retrospective review of 83 eyes with ICL implantation (42 patients) was conducted. The agreement of WTW (measured with WaveLight Topolyzer and Orbscan IIz) and ACD (measured with WaveLight Oculyzer and Orbscan IIz) was analysed. Correlation of ICL sizes and difference of eyes with unacceptable vaults between two data sets (WaveLight platform; Topolyzer and Oculyzer and Orbscan IIz) were assessed.
Results Average WTW measured by Orbscan IIz and Topolyzer demonstrated good agreement (Ρ 0.884) with low systematic bias (−0.03±0.1 mm) and narrow 95% limits of agreement (LoA) of −0.28 to 0.22. Average ACD measured by Orbscan IIz and Oculyzer also showed good agreement (Ρ 0.903) with low systematic bias (−0.04±0.1 mm) and relatively narrow 95% LoA (0.2 to 0.12). ICL size selected according to two data sets showed moderate to strong level of agreement (Kappa=0.81). There was a statistically significant difference (p<0.001) in the proportion of eyes with unacceptable postoperative vaults when using the Wavelight platform data set (five eyes, 6.02%) and the Orbscan IIz data set (12 eyes, 14.46%).
Conclusion Although the agreement of WTW and ACD between devices was good, there was a significant difference in proportion of eyes with unacceptable postoperative vaults when using two data sets. Therefore, Topolyzer and Oculyzer might not be suitable for operating interchangeably with Orbscan IIz for ICL size selection.
- treatment surgery
- diagnostic tests/investigation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Two parameters measured from Orbscan including white-to-white (WTW) and anterior chamber depth (ACD) are used in determining size of implantable collamer lens (ICL).
What this study adds?
WTW and ACD measured with WaveLight Topolyzer and Oculyzer show good agreement compared with those measured with Orbscan IIz. However, there was a statistically significant difference in the proportion of eyes with unacceptable postoperative vaults when using the data set from Wavelight platform and the data set from Orbscan IIz.
How this study might affect research, practice or policy?
Topolyzer and Oculyzer might not be suitable for operating interchangeably with Orbscan IIz for ICL size selection.
Introduction
The Implantable Collamer Lens (ICL; STAAR Surgical, Monrovia, California) is a posterior chamber, phakic intraocular lens. Over 1 000 000 ICLs have been implanted in more than 75 countries around the world.1 Long-term follow-up after implantation of ICLs has demonstrated good safety and high effectiveness for correction of moderate to high myopia and myopic astigmatism, in terms of predictable and stable refractive error correction, improvement in quality of vision and quality of life.2–5 A V4c model (EVO Visian ICL) launched in 2011 is the latest design with a central port to eliminate the need of preoperative iridotomy. The EVO design demonstrated a high rate of effectiveness and reduced rate of postoperative complication such as anterior subcapsular cataract (ASC) and pupillary block compared with the previous model.6 7 The adverse events from ICLs are usually associated with improper lens size, which results in high or low vault, the distance between anterior surface of the crystalline lens and posterior surface of ICL.
Currently, the horizontal corneal white-to-white (WTW) and anterior chamber depth (ACD) measured by Orbscan are two parameters used for calculating ICL size according to manufacturer recommendation.8 However, Orbscan is not always available in every refractive surgery centre due to individual preference and the withdrawal of device from the market. There are various instruments used for measuring WTW and ACD, including manual callipers, other corneal topography, optical biometry and anterior segment optical coherence topography (AS-OCT). The values of WTW and ACD are different depending on measurement methods. These differences could affect the variation of ICL size. Multiple research has demonstrated the correlation of WTW value between Orbscan (Bausch & Lomb, Rochester, New York) and the other devices including Pentacam HR (Oculus, Irvine, California), IOL master (Carl Zeiss Meditec, Jena Germany), EyeSys (EyeSys Laboratories, Houston, Texas) and Galilei analyzer (Ziemer group, Port, Switzerland).9 10 However, comparative study between the use of WTW and ACD measured from Orbscan and other devices to select ICL size is still lacking.
In this study, we aimed to compare WTW and ACD measured from machines incorporated with WaveLight femtosecond and excimer laser systems (ie, ALLEGRO Topolyzer VARIO and Oculyzer Corneal Topography) with WTW and ACD measured from Orbscan. Then, we compared ICL size based on parameters measured from two alternative machines with measurements from Orbscan. The postoperative achieved vault was measured to evaluate an optimal ICL calculation size method.
Materials and methods
This retrospective study included consecutive patients who underwent V4c (EVO Visian ICL) or V5 (EVO +Visian ICL) model implantation for correction of moderate to high myopia with or without astigmatism at Ramathibodi Hospital between January 2019 and December 2020. The V5 model has a larger optic diameter than the V4c model. All surgeries were performed by four experienced surgeons (VC, TS, PJ and MN). Consent form was waived due to a study design of retrospective chart review and anonymised report. Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Inclusion criteria were patients with myopia in the range of correction of phakic IOL (myopia; −0.5 to −18 diopters (D) and Cylinder;+0.5 to+6.0 D), age between 21 and 45 years, having stable refraction for at least 1 year before surgery, those with access to preoperative information of WTW and ACD, no previous intraoperative complication and patients with postoperative follow-up period of at least 6 months with available actual vault measured by anterior segment OCT. Patients with ocular pathology and previous intraocular surgery were excluded from study.
A total of 83 eyes (42 patients) were included. A complete ophthalmic examination consisting of uncorrected distant visual acuity (UDVA) and best-corrected visual acuity (BCVA), manifest refraction, slit lamp examination, fundus examination, intraocular pressure and specular microscopy was performed preoperatively. A single experienced technician measured WTW and ACD using three different machines including Orbscan IIz, ALLEGRO Topolyzer VARIO and WaveLight Oculyzer II.
Orbscan IIz is a combined placido rings and scanning-slit topography system that automatically detects the corneal limbus and calculates WTW distance. After software reconstruction of a three-dimensional anterior segment image, the ACD value is calculated automatically. ALLEGRO Topolyzer VARIO and WaveLight Oculyzer II are devices that incorporate in the Alcon/WaveLight Refractive Suite and is used for preoperative evaluation prior to refractive surgery. ALLEGRO Topolyzer VARIO is a placido disc-based topography machine (WaveLight AG, Erlagen, Germany) that contains 22 rings and generates high-resolution data of the corneal surface with 22 000 elevation points. The ‘bright ring illumination’ mode was used to capture placido camera images. Diameter of cornea (Ø cor) derived from the device was defined as ‘WTW Topolyzer’. The average of two qualified measurements with signal ‘R’ was used. WaveLight Oculyzer II is a high-resolution Pentacam camera (Oculus Optikgeräte GmbH, Wetzlar, Germany). The integrated rotating Scheimpflug camera acquires up to 50 images in real time. The average of two qualified measurements of internal ACD was defined as the distance from anterior corneal surface to the anterior lens capsule, excluding corneal thickness. Scans with a quality (Q) rated ‘OK’ were used for analysis.
The ICL power was calculated to achieve the target refraction of emmetropia using modified vertex formula developed by the manufacturer. The ICL size (ie, 12.1, 12.6, 13.2 and 13.7 mm) was determined based on WTW distance and ACD measured using Orbscan IIz. ICL model, power and size were recorded.
Postoperative achieved vault was measured using anterior segment optical coherence tomography (Visante AS-OCT: Carl Zeiss Meditec, Dublin, California). The AS-OCT scan was performed along the horizontal meridian (0–180°) centred on the pupil. After surgery, patients were followed-up at 1 day, 1 week, 1 month, 3 months, 6 months and then every year. A single scan with good quality determined by an experienced examiner was used for analysis. The actual vault was the perpendicular distance between the apex of crystalline lens and the central most anterior point of the ICL posterior surface. Acceptable and optimal vaults were defined if the measured vault fell within the range of 250 to 1000 µm and 500 to 750 µm, respectively.
Statistical analysis
Continuous data were presented in mean±SD or median (range). Category data were presented in number and percentage. The Kolmogorov-Smirnov test was used for normality checking. A paired t test was used to compare all average parameters between two devices within the same subject. The repeatability of device and the agreement of WTW (Topolyzer vs Orbscan IIz) and ACD (Oculyzer vs Orbscan IIz) between two different devices were evaluated using Bland-Altman, Deming regression11 and Pearson’s correlation analyses. The limits of agreement (LoA) between the devices with 95% CI were calculated and plotted. The Bland-Altman plots were used to identify a relationship between the differences (y-axis) and the magnitude of measurements (x-axis) and detect any bias between the two methods. Systematic bias was defined when mean difference (MD) between two methods was not close to zero. Proportional bias was defined when the difference between two methods tended to change depending on the magnitude of measurements.
For agreement of ICL size calculated by two data sets, (1) WTW and ACD from Orbscan IIz and (2) WTW from Topolyzer and ACD from Oculyzer, was analysed using Cohen’s kappa. The difference in proportions of acceptable postoperative vaults between two data sets was calculated using McNemar’s test. All analyses were performed using STATA software for Windows V.17.0 (StataCorp. 2021. Stata Statistical Software: Release V.17. College Station, Texas). A p value of equal or less than 0.05 was considered statistically significant.
Results
A total of 83 eyes from 42 patients (30 women and 12 men) were included. The patient mean age was 28.6±5.7 years. The mean of manifest refractive spherical equivalent (MRSE) was −9.9±2.3 D. All baseline characteristics and anterior segment measures are shown in table 1.
Preoperative characteristics of 83 eyes
The mean of UDVA at the last follow-up visit was 0±0.12 logMAR with the mean MRSE of −0.16±0.26 D. The mean postoperative actual vault at last follow-up period was 671.20±206 µm. Postoperative results consisting of UDVA, BCVA, MRSE and actual vaults at each follow-up visit are demonstrated in table 2. The acceptable vault (250–1000 µm) and optimal vault (500–750 µm) were achieved in 94% and 37% of eyes, respectively. High vault (>1000 µm) and low vault (<250 µm) were found in four eyes (4.8%) and one eye (1.2%), respectively.
Postoperative results after ICL implantation
Intradevice and interdevice agreement of WTW and ACD measurements
For repeatability (intradevice agreement), Topolyzer and Oculyzer demonstrated good repeatability for measuring WTW and ACD, respectively, see figure 1A,B. Topolyzer showed good agreement (Ρ=0.964) in measuring WTW with low systematic bias (−0.002±0.1 mm) and narrow LoA (95% CI −0.12 to 0.15). Similarly, Oculyzer also demonstrated good agreement (Ρ=0.875) in measuring ACD with low systematic bias (−0.003±0.1 mm) and narrow LoA (95% CI −0.20 to 0.20).

(A,B): Bland-Altman plots of differences between measurements 1 and 2; (A) White-to-white (WTW) by Topolyzer. (B) Anterior chamber depth (ACD) by Oculyzer, (C,D): Bland-Altman plots of the measurement differences between two devices; (C) WTW between Orbscan IIz and Topolyzer (D) ACD between Orbscan IIz and Oculyzer.
For interdevice agreement, the average WTW values measured by Orbscan IIz and Topolyzer demonstrated good agreement (Ρ=0.884) with low systematic bias (−0.03±0.1 mm) and narrow LoA (95% CI −0.28 to 0.22). The average ACD measured by Orbscan IIz and Oculyzer also showed good agreement (Ρ=0.903) with low systematic bias (−0.04±0.1 mm) and relatively narrow LoA (95% CI −0.2 to 0.12), see figure 1C,D. Deming regression was performed to investigate the agreement between two different devices and is presented in table 3. Similar to the results from Bland-Altman plots, the 95% CIs of the slopes included 1, which indicated good agreement of WTW and ACD measurements between different devices. However, the paired t test demonstrated statistical significance of MD in WTW measured by Orbscan IIz and Topolyzer with a p value of 0.04 (MD −0.03; 95% CI −0.06 to –0.001) and in ACD measured by Orbscan IIz and Oculyzer with a p value of <0.001 (MD −0.04; 95% CI −0.05 to –0.02).
Results of Deming regression analysis to investigate the agreement between two different devices
Agreement of ICl size between two sets of parameters
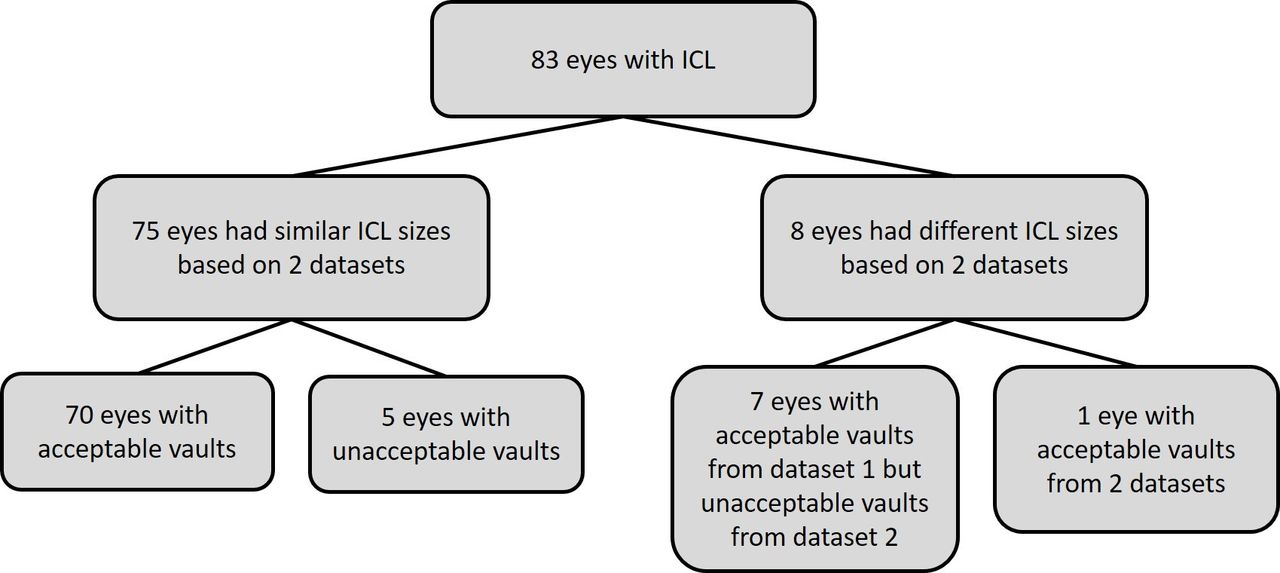
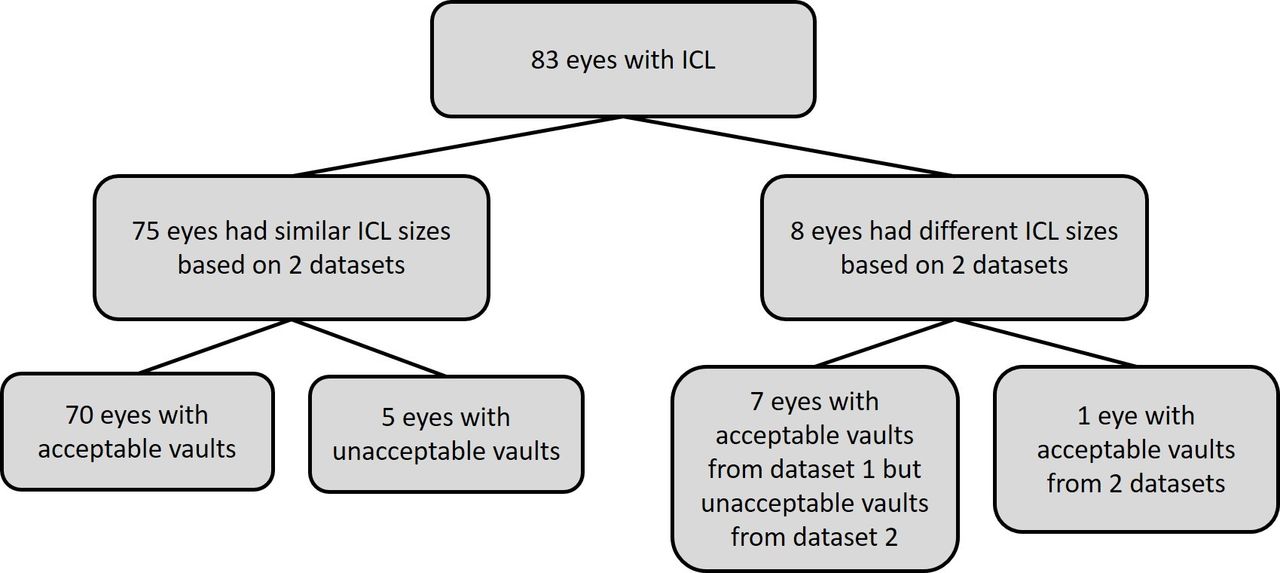
ICL size selection based on data from Topolyzer and Oculyzer (dataset 2) showed moderate to strong agreement (90.36%, Kappa=0.81, p<0.001) based on data from Orbscan IIz (dataset 1). Five out of 83 eyes (6.02%) showed unacceptable postoperative vaults (four eyes with high vaults and one eye with low vault, which subsequently need ICL exchange). Among those five eyes, ICL sizes calculated based on parameters from two data sets were the same size, see table 4. There were eight eyes (9.63%), which calculated ICL sizes were different between the two data sets, see table 5. ICL sizes calculated from Topolyzer and Oculyzer were larger than those calculated from Orbscan IIz in six eyes (7.22%), which could result in higher postoperative vaults. On the other hand, ICL sizes in two eyes (2.40%) were smaller when using parameters from data set 2, which could result in unacceptable low vaults (<250 µm). According to the assumption that the vault should increase 550 µm for each step larger ICL size (0.5 mm increment),12 the presumed postoperative vaults were calculated based on actual postoperative vaults. There was a statistically significant difference (p<0.001) in the proportion of unacceptable postoperative vaults when using data set 1 (5 eyes, 6.02%) and data set 2 (12 eyes, 14.46%), see figure 2. Presumed postoperative vault using data set 2 was 295±474.1 µm higher than postoperative vault using data set 1.
Characteristics, ICL information and postoperative vaults of five eyes with unacceptable postoperative vaults
Characteristics, ICL information and postoperative vaults of eight eyes with different ICL size based on two datasets
{kind=link}
{kind=link}
Diagram showing agreement of ICL sizes of 83 eyes when using measurements from two datasets (dataset 1; WTW and ACD from Orbscan IIz and dataset 2; WTW from Topolyzer and ACD from Oculyzer). ACD, anterior chamber depth; ICL, implantable collamer lens; WTW, white-to-white.
Discussion
ICL is an alternative option for correcting refractive errors when surface ablative procedures, for example, laser in situ keratomileusis or refractive lenticule extraction are contraindicated. However, inappropriate ICL sizing with unacceptable postoperative vaults can result in irreversible ocular complications. Low vault constitutes a risk factor for developing ASC, whereas high vault increases the incidence of pupillary block and glaucoma.13 14 The new EVO design with a central port could reduce the rate of postoperative complication compared with the previous model.6 7 Our study showed that mean postoperative vault (671 µm) and the percentage of acceptable postoperative vault (94%) were similar to the results from a previous meta-analysis.8 The percentage of acceptable vault was achieved increasingly over the follow-up periods. Theoretically, horizontal WTW distance could not directly reflect the distance from sulcus to sulcus (STS) where ICL is located; therefore, using WTW to determine the size of ICL might cause an error. STS measured by ultrasound biomicroscopy was used to calculate ICL size and demonstrated favourable postoperative vaults.15 16 However, interdevice bias between WTW and STS has been found in various degrees of correlation, thus applying error correction between two parameters for calculating ICL size could not be performed.17–19 Other parameters, including angle to angle diameter (ATA), anterior chamber width (ACW) or the iris pigment end to pigment end diameter measured with OCT, were used to create a novel formula for optimising ICL size.20–22 To date, the most appropriate formula for selecting ICL size has not been established. Moreover, it has been demonstrated that patient age, ICL power and shape of crystalline lens also affect the depth of ICL vault.22–24 These factors might need to be considered for selecting the optimal ICL size. The recent studies have applied machine learning incorporating multiple clinical measurements (eg, age, sex, preoperative spherical equivalent, ICL refractive power, type of ICL, WTW, ATA, ACD, ACW, crystalline lens rise, central corneal thickness, pupil size and lens size) to predict ICL vault and select the optimal ICL.25 26 These proposed models showed promising results with good performance compared with the conventional manufacturer’s nomogram.
In our study determining ICL size based on WTW and ACD, most eyes with unacceptable vaults were categorised in high vault (four eyes, 4.8%) and only one eye (1.2%) was classified in low vault. This result contrasted to the finding from the previous meta-analysis, which demonstrated higher ratio of having low vault (16%) more than having high vault (0.4%).8 The difference of the findings might be explained by the variety of acceptable vault criteria in the individual study.
WTW from Topolyzer and ACD from Oculyzer showed good intradevice agreement (repeatability) with narrow LoA. Our findings supported the advantage of using automated devices for WTW measurement over the use of manual method on imaging.27 However, in patients with anatomical abnormalities at the limbus such as pterygium, pigmentation or neovascularisation, manual callipers should be used to avoid measurement error from the automated devices. To the best of our knowledge, this is, the first study to investigate the agreement of WTW values derived from Orbscan IIz and Topolyzer. We found a good agreement between two devices with narrow LoA (95% CI −0.28 to 0.22). WTW from Orbscan IIz was slightly lower than from Topolyzer (MD −0.03 mm). With current STAAR ICL sizing nomogram, approximately every 0.4 mm of increasing horizontal WTW distance would increase the ICL size,1 therefore, LoA of less than 0.4 mm between two devices implies that they might be interchangeable with each other for WTW measurement. ACD is another parameter affecting the ICL size. The average ACD measured by Orbscan IIz and Oculyzer demonstrated good agreement with low systematic bias (−0.04 mm) and relatively tight LoA (95% CI −0.20, 0.12). Although the paired t test showed statistically significant differences of interdevice measurements (WTW and ACD), these differences were not considered as clinical significance. Similar to results from previous studies, ACD measured by Orbscan was slightly shallower than that measured by Pentacam (bias −0.05 mm to −0.08 mm).28 29 This result could be due to the relatively low-depth resolution of slit scanning compared with the Scheimpflug system. However, the bias between two systems was not clinically significant.
For ICL size selection, agreement of ICL size selection between two datasets was at moderate to strong level of agreement. Different ICL size was found in eight eyes (9.6%). Based on data set 2 (Topolyzer and Oculyzer), seven of eight eyes would have presumed postoperative vaults in unacceptable range (two eyes with low vaults and five eyes with high vaults). Furthermore, there was a statistically significant higher proportion of eyes with unacceptable vaults when using parameters from Topolyzer and Oculyzer compared with Orbscan IIz. This remarks that ICL size selection by using data from Topolyzer and Oculyzer instead of data from Orbscan IIz might not be appropriate. Data from Topolyzer and Oculyzer should be used with caution when Orbscan IIz is unavailable. Comparing WTW and ACD from different devices is mandatory before using these parameters for selecting ICL size, especially when WTW and ACD are the only parameters available. Moreover, taking the average of multiple readings for each parameter is recommended to verify accuracy of measurements.
This study has some limitations. First, due to the nature of a retrospective study, the actual postoperative vaults were variously measured during 1–6 months after surgery. Second, there was a small sample size with five eyes classified as having unacceptable vaults. Thus, factors contributing to unacceptable vaults could not be evaluated. Finally, presumed postoperative vaults were calculated based on assumption, which might not entirely represent the actual postoperative vaults. This could overestimate a number of eyes with unacceptable postoperative vaults based on parameters from Topolyzer and Oculyzer and lead to underestimate the performance of ICL size selection based using data set 2. Further prospective studies comparing other commonly used devices such as Pentacam and IOLMaster or using aggregate measurements (eg, mean, median, and mode) from multiple devices with larger sample size are warranted to determine the factors associated with unacceptable vaults and to obtain the most appropriate formula for ICL size selection.
Conclusion
Topolyzer and Oculyzer demonstrated good repeatability for measuring WTW and ACD, respectively. Additionally, they also showed a good interdevice agreement with WTW and ACD measured by Orbscan IIz. However, when we applied WTW and ACD measured by these alternative devices for determining ICL size, we found significantly higher number of patients with unacceptable vault compared with using values measured from Orbscan IIz. Therefore, measurements derived from Topolyzer with Oculyzer might not be suitable to use interchangeably with data from Orbscan IIz for determining ICL size.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Committee of Ramathibodi Hospital (Number MURA 2021/195).
Acknowledgments
We thank Ms. Sukanya Siriyotha for her assistance with data analysis and Ms. Sranya Phaisawang for English-language editing of the manuscript.
References
Footnotes
Correction notice This article has been corrected since it first published. Author name 'Nontawat Cheewaruangroj' has been updated.
Contributors MN and PJ were responsible for study design. MN, PP, NC and VC were involved in data acquisition. MN and PJ conducted data analysis. MN, PJ and KL drafted and wrote the manuscript. All authors approved the final manuscript. PJ was the guarantor on behalf of all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.