Article Text

Abstract
Objective Femtosecond laser-assisted cataract surgery (FLACS) decreases the use of energy and provides a more precise capsulorhexis compared with conventional phaco surgery (CPS). The purpose of this study was to examine if the lower energy use in FLACS caused less endothelial cell loss compared with CPS and if there was a difference in refractive predictability between CPS and FLACS.
Methods and analysis This was a randomised controlled study of 96 patients with a 6-month follow-up comparing one eye surgery by FLACS and the contralateral eye operated by CPS (divide and conquer technique). Both eyes had intraocular aspheric lenses implanted. Uncorrected distance visual acuity, corrected distance visual acuity (CDVA), central corneal endothelial cell count and hexagonality (non-contact endothelial cell microscope) were assessed preoperatively at 40 and at 180 days postoperatively.
Results The mean phaco energies were 6.55 (95% CI 5.43 to 7.66) and 9.77 (95% CI 8.55 to 10.95) U/S (p<0.0001) by FLACS and CPS, respectively. At day 40, the mean endothelial cell loss (ECL) was 344 cells/mm2 (95% CI 245 to 443) by FLACS (12.89%) and 497 cells/mm2 (95% CI 380 to 614) by CPS (18.19%) (p=0.027). At day 180, ECL was 362 cells/mm2 (95% CI 275 to 450) in FLACS (13.56%) and 465 cells/mm2 (95% CI 377 to 554) in CPS (17.03%) (p=0.036).
The mean absolute difference from the attempted refraction was 0.43 (95% CI 0.36 to 0.51) dioptres (D) at day 40 and 0.46 D (95% CI 0.39 to 0.53) at day 180 by FLACS compared with 0.43 D (95% CI 0.36 to 0.51) at day 40 (p=0.95) and 0.46 D (95% CI 0.37 to 0.52) at day 180 (p=0.91) with CPS.
Conclusion ECL was significantly lower in FLACS compared with CPS at both day 40 and day 180. ECL was correlated to the energy used. We found no difference in refractive predictability or CDVA between the groups.
- Cataract surgery
- femtosecond-assisted cataract surgery
- LensAR
- Corneal endothelial cell loss
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Femtosecond laser-assisted cataract surgery (FLACS) reduces effective phacoemulsification time (EPT) and cumulative dissipated energy (CDE) usage and can perform a consistent capsulotomy. This study examined if the lower EPT and CDE usage caused less endothelial cell loss (ECL) on the long term and if the consistent capsulotomy resulted in better refractive outcome compared with conventional phaco surgery (CPS).
What are the new findings?
FLACS caused 21% less ECL compared with CPS. The cell loss difference was 103 cells/mm2 at 6 months. In our study, FLACS did not provide superior refractive predictability nor better visual outcome than CPS.
How might these results change the focus of research or clinical practice?
A patient with a healthy endothelium can endure the cell loss difference found in this study. These results indicate that FLACS is not superior to CPS in patients with healthy eyes and therefore it should not be chosen over CPS.
Introduction
Femtosecond laser-assisted cataract surgery (FLACS, see table 1 for abbreviations) was introduced in 2009 by Nagy et al.1 This technology provides a high-resolution anterior segment imaging system with a femtosecond laser, which delivers short pulses (10−15 s) of energy at a near-infrared wavelength, with the ability to focus at very specific depths within the anterior chamber. FLACS offers numerous potential advantages over conventional phaco surgery (CPS) as FLACS can perform automated, standardised corneal incisions, capsulorhexis and lens fragmentation. Studies have shown that FLACS leads to more accurate capsulorhexis with less intraocular lens (IOL) decentration and lens tilt compared with manually performed capsulorhexis in CPS.2–5 A precise capsulotomy has been proposed to improve the precision of the IOL position, and thus the predictability of both IOL power and refractive outcome.6 7 The corneal endothelium maintains the transparency of the cornea, thereby having an important role in maintaining a good visual outcome. It is well-known that phacoemulsification energy causes endothelial cell loss (ECL).8 Studies have shown that FLACS decreases endothelial cell loss compared with CPS. However, most studies have short-term follow-up and, therefore, the long-term effects of FLACS on the endothelium remains unknown.9–12 The purpose of this study was therefore to examine if FLACS is superior to CPS regarding refractive results and if the lower needed phaco energy in FLACS causes less ECL compared with CPS on the long term.
List of abbreviations used in the article
Materials and methods
This prospective randomised clinical trial consists of a consecutive cohort of 108 patients that were offered FLACS on one eye and CPS on the contralateral eye at the Department of Ophthalmology, Glostrup, University Hospital of Copenhagen, Denmark.
All patients volunteered to be included in the trial.
Inclusion criteria were a visually significant cataract of any type and degree and age older than 18 years. Exclusion criteria were a history of severe dry eye, corneal scars, history of herpetic keratitis, signs of keratoconus, history of uveitis, pseudoexfoliation syndrome, uncontrolled glaucoma, visually significant maculopathy, vitreomacular traction, lack of cooperation or tremor and previous ocular surgery. If patients failed to have both eyes operated on (one eye with FLACS and the other eye with standard CPS), they were also excluded.
Preoperatively
The patients underwent an assessment to establish eligibility for undergoing FLACS and CPS.
All patients were used as their own control, and the following measurements were done: corrected distance visual acuity (CDVA) using an LCD visual acuity chart with equal logarithmic difference between the lines with decimal numbers for later possible conversion to logMAR values, autorefraction, IOL power calculation by the SRK/T formula in axial length 22–28 mm and Haigis formula in axial length <22 or >28 mm (IOLMaster; Carl Zeiss Meditec AG), applanation tonometry and slit-lamp evaluation including corneal status, cataract grading and fundus status with ophthalmoscopy. The cataract grading was based on a subjective assessment from zero to four performed by an experienced cataract surgeon: zero representing a clear lens and four representing a dark brown lens. Endothelial cell density and percentage of hexagonal cells were analysed using a non-contact specular microscope (SP 3000P; Topcon, Tokyo, Japan) with the Image-Net imaging system (V.4.0; Topcon). All patients underwent an ocular coherence tomography to exclude macular pathology and vitreomacular traction.
Postoperatively
The patients had a follow-up after 40 and 180 days at an optometrist blinded for operation technique. The following measurements were performed: uncorrected distance visual acuity (UDVA), CDVA with subjective refraction performed by an optometrist using an LCD visual acuity chart with equal logarithmic difference between the lines with decimal numbers for later possible conversion to logMAR values, autorefraction and endothelial imaging with endothelial cell density and hexagonality.
Endothelial cell imaging
Preoperatively and at day 40 and 180, three photographs of each cornea were taken and analysed automatically by the Image-Net imaging system. Afterwards, a blinded observer chose the clearest image of the three and discarded the remaining two images. Hereafter, the cell count performed by Image-Net was manually corrected according to the golden standard.13 14
We calculated endothelial cell loss by:
Endothelial cell loss=Endothelial cell densitypreoperatively–Endothelial cell densityday 40 or day 180
When calculating percentage endothelial cell loss, the following formula was used:
(Endothelial cell loss/Endothelial cell densitypreoperatively)×100
Refractive outcome
Refractive outcomes were analysed using spherical equivalent (SE) and the mean absolute error (MAE), which is the absolute difference between predicted and achieved postoperative SE refraction. We performed a subanalysis on patients with a preoperative refractive status of hyperopic eyes (>3 D), myopic eye (>6 D) and astigmatic eyes (>2 D), and we analysed our refractive results both with and without these patients.
Ultrasound energy and fluid use
Infiniti Vision System (Alcon Laboratories, Fort Worth, Texas, USA) uses cumulative dissipated energy (CDE) as a value for phaco energy. This is calculated as (phaco time×average phaco power)+(torsional time×0.4×average torsional amplitude). The factor 0.4 represents approximate reduction of heat dissipated at the incision as compared with non-torsional phaco.
Fluid use was read from the Infiniti Vision System (Alcon Laboratories) after completed surgery.
Randomisation
All patients had one eye randomly allocated by computer randomisation into either FLACS or CPS. Randomisations were block randomisations performed by one clinician (TK) blinded from the operating order of the eyes. All randomisations were noted on a randomisation sheet. On surgery day, the surgeon would open the randomisation sheet and see what operation had to be performed. The other eye would receive the treatment not given to the randomised eye.
Surgical technique
All patients were operated on by the same experienced cataract surgeon (AM). The eye with much worse vision was operated on first in order to forecast the second better-seeing eye from any possible complication. AM had performed more than 100 FLACS procedures before patient inclusion started.
FLACS
The laser (LensAR Laser System; LENSAR, Orlando, Florida, USA) procedure started with the docking of the laser with a 3D imaging of the anterior chamber, suggesting a treatment plan. Treatment plan and images were confirmed before the laser procedure. The laser performed a 5.0 mm capsulotomy and lens fragmentation. Lens fragmentation pattern was ‘piecut 6’ with three concentric circles. Hereafter, the laser was disconnected, and the remaining surgery was done as conventional phaco (CPS).
CPS
A 1 mm side port was created with a keratome followed by instillation of 0.5 mL lidocaine (10 mg/mL) and an ophthalmic viscosurgical device (Healon; Abbott Medical Optics, Santa Ana, California, USA). Then, a clear cornea main incision was fashioned with a 2.4 mm angled keratome. A continuous curvilinear capsulorhexis with an intended diameter of 5 mm was created (Utrata Forceps, Antony, France).
Phacoemulsification (Infiniti Vision System; Alcon Laboratories) and irrigation/aspiration (I/A) were performed using the technique ‘divide and conquer’. An aspheric, hydrophobic IOL (ZCB00; Abbott Medical Optics) was implanted using Healon, which was then aspirated. The procedure was concluded by instillation of 1 mL cefuroxime (2.5 mg/mL) and hydration of the incisions.
All statistical analyses were performed using R software (V.1.0.44). Baseline values were expressed as the mean with a 95% CI. Between-group comparative statistics were determined using a paired Student’s t-test or the Mann-Whitney U test in case of non-parametric data. To evaluate visual outcome, all decimal values which came from an LCD visual acuity chart with equal logarithmic difference between the lines were transformed to logMAR values for the statistical analysis. Afterwards, logMAR values were back-transformed into Snellen values for easier reader-interpretation of the results. A univariate analysis with patients as random effects was used to evaluate the impact of operation variables on endothelial cell loss. Variables were operation method, phaco energy, fluid use, surgery time, preoperative endothelial cell density and cataract grade. Afterwards, a multivariate analysis of all variables with a significant outcome in the univariate was performed. P values of less than 0.05 were considered statistically significant. The sample size was calculated based on SD obtained in a previous study.9 This calculation resulted in 65 eyes per group, which was increased to 108 to compensate for possible drop-outs.
Patient inclusion and exclusion
The study comprised 216 eyes of 108 patients (56 women) with a postoperative follow-up of 180 days. The mean (±SD) number of days from operation to 40 days follow-up was 60±34 and the mean number of days from operation to 180 days follow-up was 234±124.
Results
Complications
In total, we had five cases with preoperative and postoperative complications. These were equally distributed between the two groups (figure 1). We had one case without recognised preoperative risk factor who suffered nucleus loss and retinal detachment. This patient had FLACS and was excluded from the data analysis because the second eye was not operated on. In the remaining four cases with complications, the preoperative risk factors that we detected were as follows: (1) one CPS patient who used alpha-1-antagonist medicine and suffered capsule rupture—this patient cancelled the second eye surgery and was therefore excluded from the data analysis; (2) one FLACS patient suffered corneal oedema—this patient cancelled the second eye surgery and was, therefore, excluded from the data analysis; (3) one CPS patient suffered corneal oedema—this patient cancelled the second eye surgery and was, therefore, excluded from the data analysis; (4) one FLACS patient who had previous steroid treatment and suffered zonula rupture with sulcus implantation of the IOL—this patient had both eyes operated on and was included in the data analysis.

Display of patients included and follow-up. *Four patients with complications cancelled second eye surgery and failed to appear for follow-up. One of these patients had preoperative risk factors with alpha-1-antagonist treatment. This patient suffered from capsule rupture. Three patients with no preoperative known risk factor suffered from complications. Two patients suffered from corneal oedema and cancelled the next operation. One patient suffered nucleus loss and retinal detachment. All four patients cancelled the second eye surgery and were, therefore, excluded from the data analysis. FLACS, femtosecond laser-assisted cataract surgery.
Preoperatively
In the FLACS eyes, there were 10 hyperopic (>3 D), 1 myopic (>6 D) and 7 astigmatic patients (>2 D). In the CPS eyes, there were 13 hyperopic, 2 myopic and 6 astigmatic patients. Therefore, the two groups had comparable preoperative refractive status. When pairing the eyes, the mean (±SD) preoperative difference in SE was −0.24±1.68 D (95% CI −0.58 to 0.09). The cataract grade was comparable between the two groups (table 2).
Baseline characteristics of cataract grade and operation data: refractive and visual results
For MAE, we detected no significant difference between the two groups at day 40 or day 180 (table 3). This result remained non-significant after adjusting for preoperatively refractive status with hyperopic eyes (>3 D), myopic eyes (>6 D) and astigmatic eyes (>2 D) (table 3). At day 40, we found that 13.5% achieved attempted refraction (MAE=0) in FLACS compared with 10% in CPS, FLACS had 66% with an MAE less than 0.5 while CPS had 65%. At day 180, 10% achieved attempted refraction in both FLACS and CPS. Fifty-six per cent of eyes treated by FLACS ended with an MAE of less than 0.5 D, compared with 64% treated by CPS.
Preoperative and postoperative values of SE and MAE
At day 40, CPS had a significantly better UDVA than FLACS. UDVA at day 180 and CDVA at day 40 and day 180 were not significantly different between the groups (table 4). In FLACS, 31% had UDVA ≥1.0 at day 40 compared with 27% in CPS. At day 180, 30% of the FLACS eyes had UDVA ≥1.0 compared with 32% in the CPS group. At day 40, both FLACS and CPS had 71% with a CDVA ≥1.0. At day 180, FLACS had 75% with CDVA ≥1.0 while CPS had 75% with CDVA ≥1.0.
Visual outcome day 40 and day 180 in FLACS and CPS
Surgical results
CDE was significantly lower in FLACS compared with CPS. Comparing the two treatments, there was no statistically significant difference between knife time (see table 2); however, total procedure time (laser and knife time combined in FLACS vs knife time in CPS) was significantly longer in the FLACS eyes compared with the CPS eyes. There was a 15% significantly higher fluid use in FLACS compared with CPS.
Endothelial cell results
The ECD and hexagonality were comparable between the two groups preoperatively. At day 40 and day 180, ECL was significantly lower in FLACS eyes compared with CPS eyes. Comparing the two groups, there was no statistically significant difference between hexagonality change at day 40 or day 180 (table 5).
Preoperative and postoperative values of ECD, endothelial hexagonality and ECL in FLACS and CPS (ECL is also presented as percentages in parentheses)
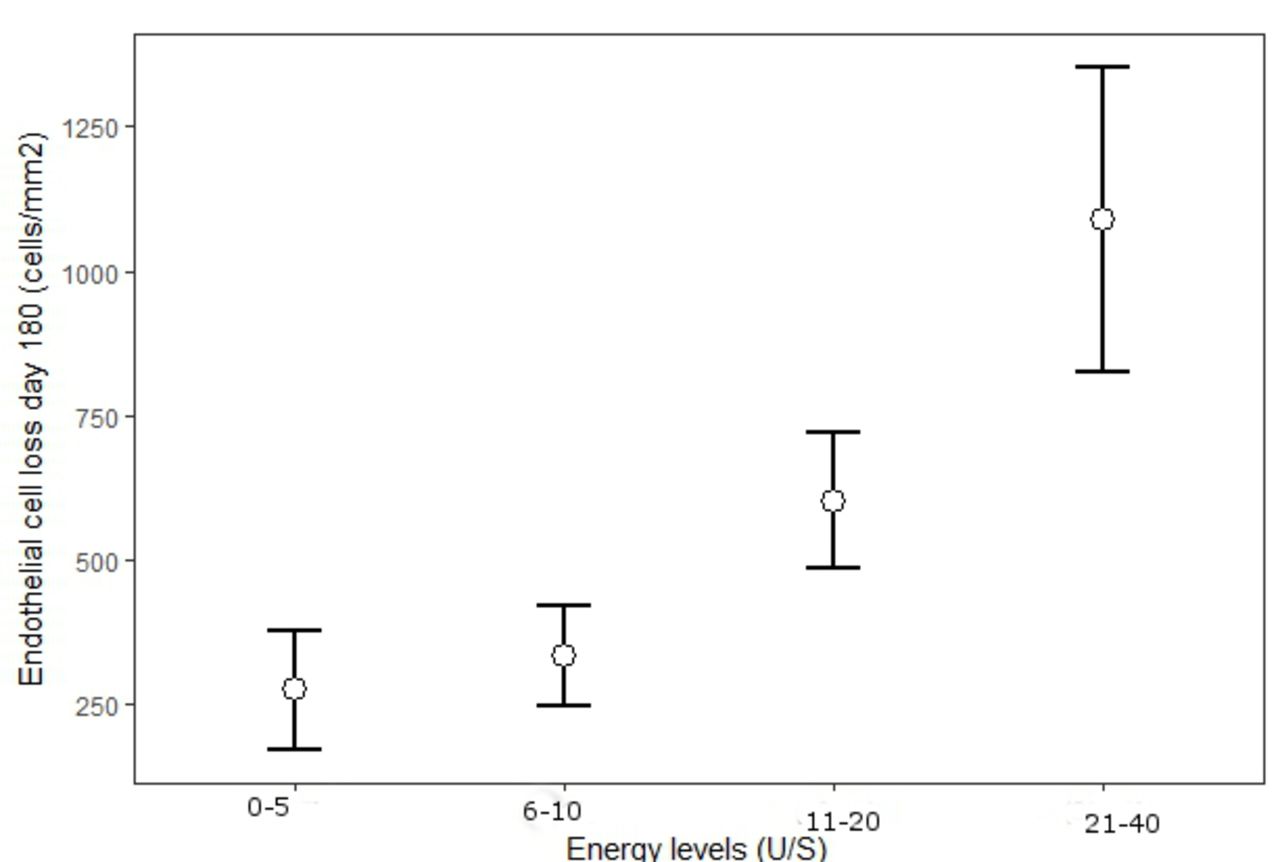
Univariate analysis showed that CDE, preoperative endothelial cell density, fluid use and operation method all had a significant effect on ECL. The multivariate analysis confirmed the significant correlation between ECL and CDE use as well as preoperative ECD; however, operation method and fluid use were insignificant in the multivariate analysis (table 6). We also performed another model where we divided CDE into different levels (0–5, 6–10, 11–20 and 21–40 U/S) and examined what impact the different levels of CDE had on ECL (figure 2).
Multivariate analysis

Mean endothelial cell loss at day 180 (cells/mm2) at different cumulative dissipated energy (CDE) levels. The figure demonstrates that the relationship between CDE and endothelial cell loss is non-linear and that there is less endothelial cell loss at lower CDE.
Discussion
The aim was to compare refractive predictability and endothelial cell loss in FLACS compared with CPS with a 6-month follow-up.
The timeframe for endothelial cell recovery is 1 to 180 days.15 To evaluate the long-term effect of FLACS on the endothelium, we therefore measured endothelial cell loss at day 180. We detected a significant difference in ECL between FLACS and CPS at both day 40 and 180 with a mean difference of 152 cells/mm2 (30% cell loss reduction in FLACS compared with CPS) at day 40 and 103 cells/mm2 at day 180 (21% cell loss reduction in FLACS compared with CPS). A patient with a healthy endothelium can endure a cell loss of 100–160 cells/mm2 without suffering from corneal oedema; however, for patients suffering from pre-existing endothelial cell loss, this amount of cell loss might cause corneal oedema.
In CPS, there are ECL rapports between 1.4% and 23%.8 16–19 Comparative studies between FLACS and CPS describes the ECL percentages as 5.8%–13.7% in the CPS group and 4.3%–17.06% in the FLACS group.9–12 20 21 Our findings with a difference in ECL percentages of 12.89%–18.19% are in the high end of these findings.9–12 20 21 A problem when comparing ECL results in comparative studies is the heterogeneity in the cell counting technique. Validation studies report that the most reliable cell counts are obtained by choosing the clearest image, which is used for automated cell count performed by Image-Net and then manually correcting any incorrectly drawn cell borders.13 14 We used this technique. However, most studies examining ECL and FLACS do not mention how ECD are counted, which might explain the different ECL results found in other reports. Another problem with previous studies is that the majority of these are non-randomised studies with a short follow-up of about 3 months making them inadequate to evaluate the long-term effect. To our knowledge, none of the comparative studies between CPS and FLACs have examined endothelial hexagonality. We saw an initial change of hexagonality at day 40 which was more profound in the FLACS group compared with CPS (5% vs 1.8% p>0.05). At day 180, the hexagonality change was normalised in FLACS while CPS reported a 2% hexagonality change (p>0.05). Our findings are in agreement with previous findings examining hexagonality after cataract surgery in patients with a healthy endothelium.8 16 19
When plotting the effect of different CDE levels on ECL (figure 2), we found that the relationship between ECL and CDE is non-linear, and CDE use above 10 U/S causes a doubling or more in ECL compared with CDE use below 10 U/S. In figure 3, ECL and the use of CDE in the two groups are plotted, showing that the initial ECL is higher in FLACS until a CDE level of approximately 10 U/S, after which the curve flattens. This suggests that one can use up to 10 U/S of CDE in CPS without causing more cell loss than with FLACS. The higher amount of ECL at <10 U/S in FLACS compared with CPS suggests that factors other than CDE are involved in ECL. These other factors might be manual handling, turbulence, knife time and fluid use—in our study, we found that FLACS was associated with increased fluid use compared with CPS. This could be due to lens fragments that are not completely divided by FLACS compared with the cracking method used in CPS.
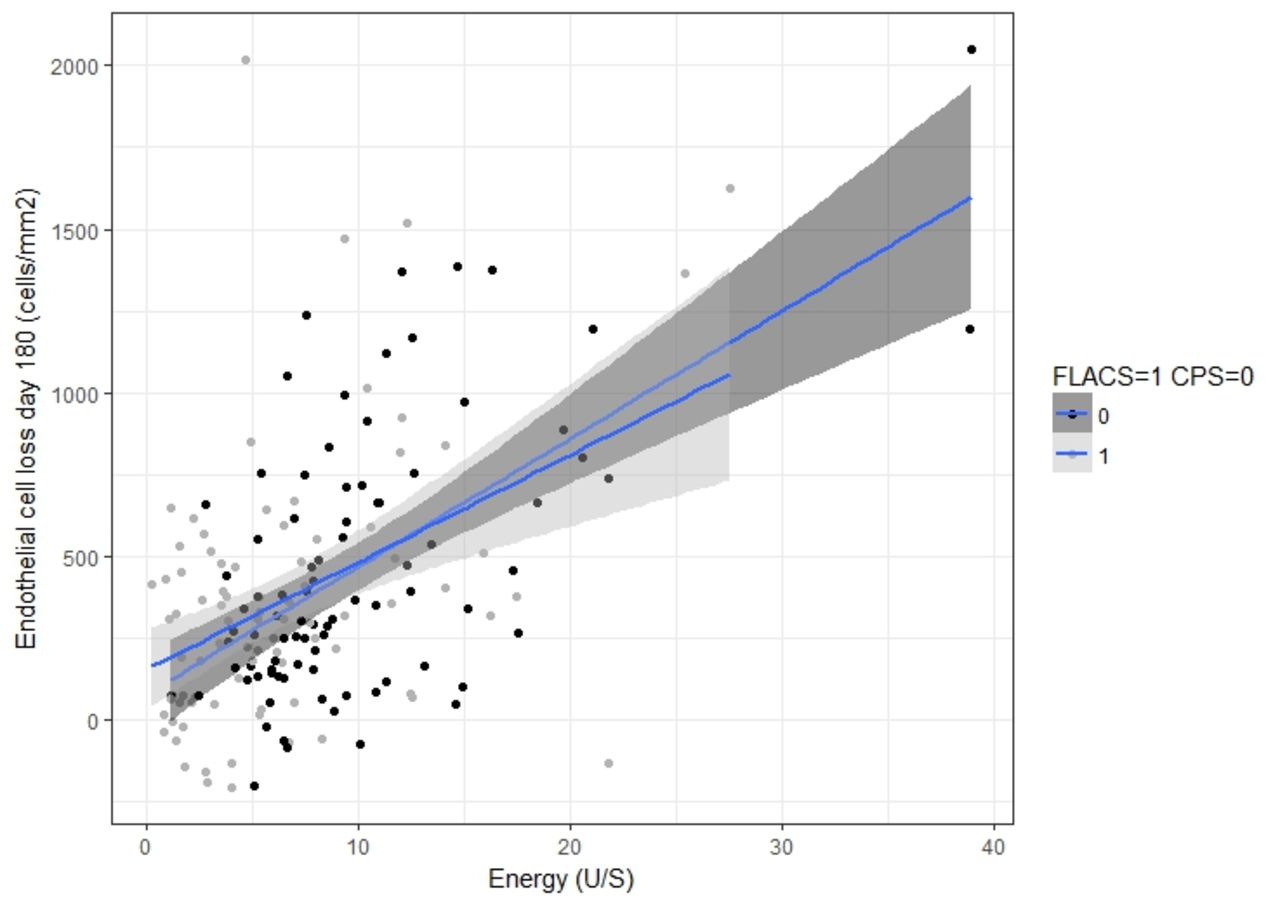
Correlation between cumulative dissipated energy (CDE) and endothelial cell loss (ECL) in femtosecond laser-assisted cataract surgery (FLACS) and conventional phaco surgery (CPS). At day 180, the mean ECL was 326 cells/mm2 in FLACS and 465 cells/mm2 in CPS. FLACS had greater ECL than CPS up to CDE energy levels of around 10 U/S.
Our univariate analysis found that both fluid use and operation method were significant for ECL. Both variables became non-significant in the multivariate model (table 6), leaving only CDE and preoperatively ECD as significant for ECL. This indicates that the main contributor to ECL is CDE and operation method becomes non-significant as it is correlated to energy; thus, as FLACS uses less CDE than CPS, it has a lesser impact on the ECL.
In our study, we found a 33% decrease in CDE by FLACS. We used the operation method ‘divide and conquer’ and not chopping. The energy difference between CPS and FLACS would probably have been smaller if a chopping method had been used.8 However, we chose divide and conquer as this method was the preferred method by our experienced surgeon. Chopping technique can be more surgeon dependent and might lead to more manipulation in the eye with more impact on the endothelium.8
We report five cases of complications: two cases in CPS eyes and three cases in FLACS eyes. The types of complications were different between the two groups but of equal severity. Four of the patients with complications cancelled their second eye surgery and, thus, were not included in the data analysis. Because the complications were equally distributed between the two groups, there was no skewness in the data.
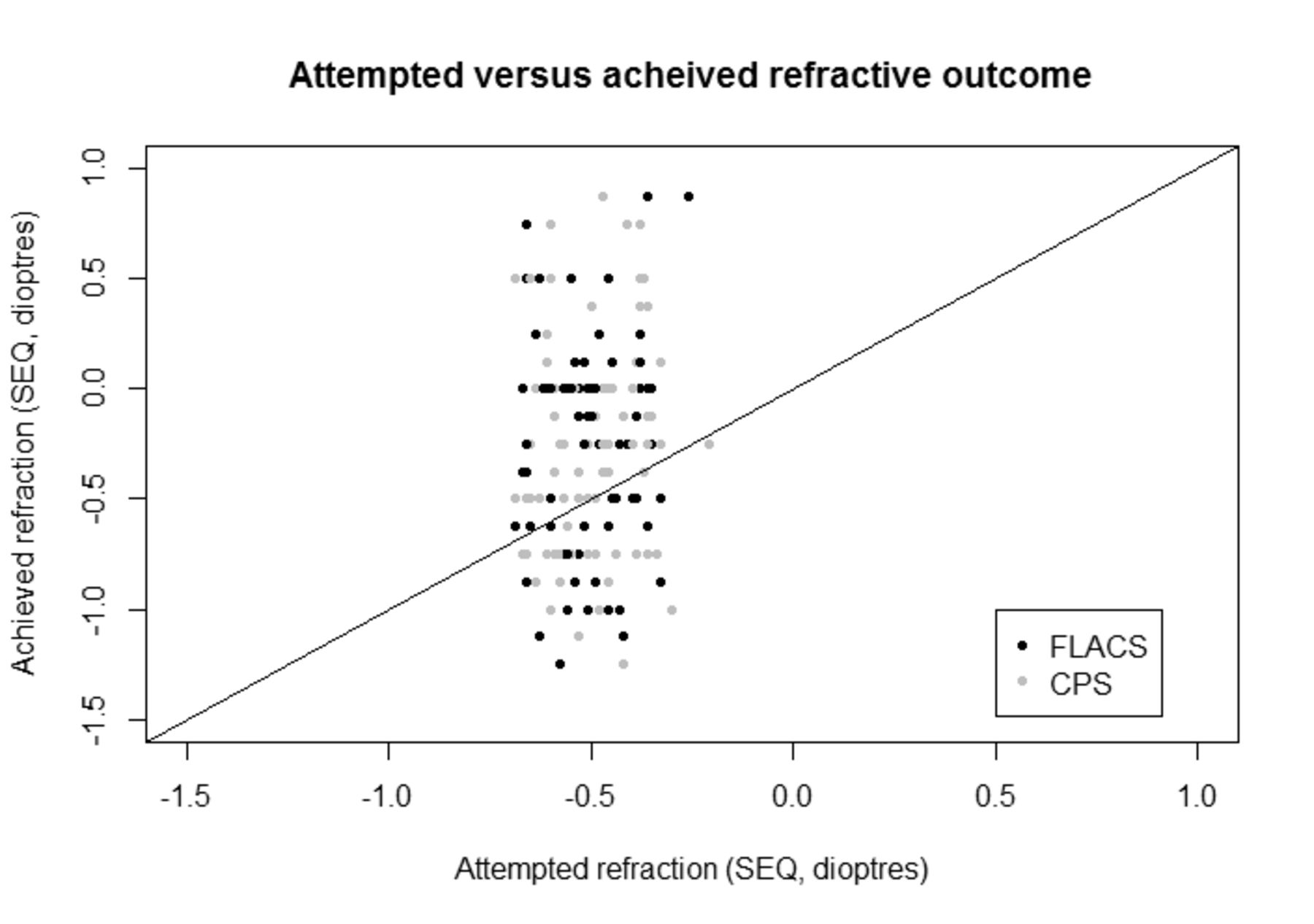
FLACS produces a more centred circular capsulotomy compared with CPS. A more precise capsulotomy would likely improve the position of the IOL and, thus, the predictability of the IOL power and the refractive results. We found no significant difference in MAE (table 3 and figure 4) even when adjusting for myopia, hyperopia and corneal astigmatism. These results concur with previous findings by other authors.3 22–24 We found that our target refraction trended towards a more hyperopic refraction than intended (figure 5). In contrast to our findings, Conrad-Hengerer et al performed a randomised controlled trial examining refractive and visual outcome in 100 patients with 180 days of follow-up.25 They found significant less MAE in FLACS (92% within 0.5 D) compared with CPS (71% within 0.5 D). This may be due to their exclusion of patients with high myopia, hyperopia or corneal astigmatism of more than 1.5 D.

Comparison of postoperative MAE at 180 days after surgery between FLACS and CPS. Ten per cent achieved the attempted refraction in both FLACS and CPS. Fifty-six per cent treated by FLACS ended with an MAE of less than 0.5 D, compared with 64% treated by CPS. We detected no significant difference in CDVA or UDVA outcome between the two groups. CDVA, corrected distance visual acuity; CPS, conventional phaco surgery; FLACS, femtosecond laser-assisted cataract surgery; MAE, mean absolute error; UDVA, uncorrected distance visual acuity.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Achieved vs attempted refraction. Most eyes achieved an attempted refraction of zero spherical equivalent (SEQ). The circles below the line indicate that the eyes achieved a more myopic refraction than intended and vice versa. We found a subtle trend towards a more hyperopic refraction. CPS, conventional phaco surgery; FLACS, femtosecond laser-assisted cataract surgery.
We detected a significantly better UDVA in the CPS group at day 40 compared with the FLACS group. However, this difference was non-significant at day 180. We detected no difference in CDVA between the two groups, at day 40 or day 180.
A possible explanation for the non-superior refractive results in FLACS could theoretically be that FLACS causes a more unstable capsulorhexis leading to more IOL decentration and lens tilt. However, Panthier et al recently found that the mean diameter, mean deviation from intended rhexis size and mean deviation error were greater in CPS compared with FLACS a long with their finding with no significant differences in in UDVA, CDVA and MAE between the two groups.26
Mastropasqua et al and Toto et al examined lens decentration in the sagittal plane and both reported significantly less lens decentration in FLACS compared with CPS at day 180.3 24 In monofocal lenses, multiple reports state that decentration becomes clinically relevant with a decentration of >0.4 mm.27 28 Mastropasqua et al and Toto et al found lens decentration in both CPS and FLACS to be less than the clinical relevant 0.4 mm.3 24
Limitations in our study is the lack of an objective or standardised subjective grading of the cataract grade preoperatively. This was not performed as cataract grading was not of primary concern instead we used energy consumption to evaluate ECL. We chose to use the patient as an intraindividual control and therefore randomised one eye leaving the other to get the opposite treatment than the randomised eye. It would have been possible to randomise all eyes instead of only one of the two eyes. We chose the former to reduce interindividual variation and because randomisation of all eyes would require inclusion of twice the number of eyes.
We included two follow-up controls. Follow-up at day 40 was to examine refractive predictability not too long after surgery and follow-up at day 180 was to examine the long-term results of FLACS and CPS. However, it is possible that the interval between these two follow-ups are too long to detect a significance, and it would have been interesting to have a follow-up closer to the surgery date and after 3 months. We used the surgical technique ‘divide and conquer’, and we might have had different energy and ECL outcome if chopping technique had been used. Also, we used the LensAR Laser System (LENSAR) and Infiniti Vision System (Alcon Laboratories), and it would have been interesting to test a fluid-based interface system such as the Centurion Vision System (Alcon Laboratories). Furthermore, we did not measure IOL decentration or lens tilt.
Our study is strengthened by its study design, which includes randomised choice of operation, a large patient cohort, use of a single experienced surgeon, counting of ECD by manually correcting the automated drawn cell borders by a blinded observer (as validation studies suggest), and blinded optometrist refraction performed at day 40 and day 180, as well as the use of the patients as their own control: one eye operated on by FLACS and the other eye by CPS.
Conclusion
We found that FLACS is associated with a 30% reduction in ECL at day 40 compared with CPS and a 21% reduction at day 180, with a mean difference in cell loss of 103–152 cells/mm2. These are promising results that could potentially benefit patients with pre-existing endothelial cell loss. Future studies examining the impact of FLACS on the endothelium and its effect on corneal oedema in patients with pre-existing endothelial cell loss are needed. In our study, we detected no difference in refractive predictability nor visual outcome. At the moment, FLACS has yet to be shown to be advantageous compared with CPS in refractive clinical results.
Acknowledgments
The authors thank Mette Correll and Henrik Alf Melsom for their great help with patient inclusion.
References
Footnotes
Contributors TK: concept and design, recruitment of patient, data acquisition, drafting manuscript, statistical analysis, revision of manuscript. RE: data acquisition, data analysis, critical revision of manuscript. ALM: concept and design, data acquisition, data analysis, critical revision of manuscript. LMH: concept and design, data analysis, statistical analysis, critical revision of manuscript. MlC: concept and design, data analysis, statistical analysis, critical revision of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study adhered to the Declaration of Helsinki and was approved by the Local Committee of Ethics and the Danish Data Protection Agency.
Provenance and peer review Not commissioned; externally peer reviewed.