Article Text

Abstract
Objective To evaluate the intraocular pressure (IOP)-lowering effect based on the number of ingredients and survival rate due to adverse reactions of brinzolamide (1%)/brimonidine (0.1%) fixed combination (BBFC).
Methods and analysis Among 424 patients newly administered BBFC from June 2020 to May 2021, 406 were retrospectively evaluated for adverse reactions and 299 were evaluated for the IOP-lowering effect of BBFC. Among those evaluated for IOP, group A (n=86) included patients whose treatment was changed to BBFC from other two ingredients, Group B (n=90) included patients who added one ingredient by switching to BBFC, and group C (n=123) included patients who added BBFC in addition to other drugs.
Results The mean IOP (mm Hg) at BBFC initiation and at 3, 6 and 12 months after BBFC initiation was 14.1, 14.0, 14.3 and 13.8 in group A, 15.9, 14.4, 13.8 and 14.5 in group B and 17.2, 14.0, 14.1 and 14.9 in group C, respectively. Group A showed no significant difference in mean IOP from baseline to any time point after BBFC initiation, whereas groups B and C showed significant IOP reductions at all time points. Seventy-three (18%) patients discontinued treatment due to adverse reactions. The survival rate was 72% at 12 months after the start of BBFC when discontinuation due to adverse reactions was defined as failure.
Conclusion Using BBFC, sustained IOP or decreasing IOP were observed depending on the number of ingredients. Drop-outs due to the adverse reactions should also be given attention.
- Glaucoma
- Intraocular pressure
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The efficacy of brinzolamide (1%)/brimonidine (0.1%) fixed combination (BBFC) has been reported in previous papers. However, there has not yet been a report examining the efficacy of glaucoma eye-drops focusing on the number of ingredients.
WHAT THIS STUDY ADDS
Switching to BBFC or adding BBFC had a similar intraocular pressure (IOP)-lowering effect to that when there was no change in the number of ingredients and a significant IOP-lowering effect was observed when the number of components was increased by one or two.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The efficacy of BBFC has been demonstrated and provides a rationale for glaucoma eye-drop treatment using combination drugs and enhances treatment.
Introduction
Lowering intraocular pressure (IOP) is the only effective means of treating glaucoma; moreover, it can prevent glaucoma or inhibit its progression.1 2 This has been reported in cases of primary open-angle glaucoma with high IOP when untreated3 as well as confirmed in cases of normal tension glaucoma.4 Some options to reduce IOP include drug use and incisional and laser surgeries. Glaucoma eye-drops are a commonly used as the first treatment option, but adherence to the drops can be problematic for continued treatment. In a retrospective cohort study of 1234 patients with newly diagnosed or initiated treatment for primary open-angle glaucoma, eye-drop adherence was good in 15% of patients at 4 years after treatment initiation.5 A study of 307 patients on eye-drop therapy followed for an average of 7.3 years reported that worsening eye-drop adherence was associated with worsening mean deviation values when patients were classified into the following groups: no eye-drop forgetfulness, ≤1/3, 1/3 to 2/3 and >2/36; this indicated that methods to prevent worsening adherence are needed.
Brinzolamide (1%)/brimonidine (0.1%) fixed combination (BBFC) has recently been used in glaucoma drug regime as the first β-blocker-free combination eye-drop for glaucoma treatment (the concentration of brimonidine was half in Japan). In BBFC, a combination of two eye-drops is present in one bottle; it is safer for patients with cardiac disease and asthma. Multiple drug use leads to decreased adherence,7 and conversely, reducing the number of eye-drop bottles and frequency of eye-drops leads to improved adherence.8 9 These factors suggest that combined eye-drop treatment with BBFC has a significant advantage. Previous reports showed the efficacy and safety of BBFC up to 4 weeks,10 11 3 months12 and 6 months.13 However, no previous report has shown the long-term effects of BBFC in terms of IOP reduction and safety profiles, especially based on the number of glaucoma medication components. In this study, we aimed to evaluate the IOP-lowering efficacy and safety of BBFC for a duration of 12 months, especially based on the number of medication components.
Materials and methods
Of the 424 patients newly administered BBFC at Tsukazaki Hospital from June 2020 to May 2021, 406 who were traceable were evaluated for adverse reactions, and 299 were evaluated for IOP reduction after excluding patients who started other glaucoma medications at the same time as BBFC and those with a history of eye surgery within 1 year before starting BBFC. We retrospectively investigated the IOP-lowering effect and adverse reactions of BBFC using hospital medical records. If both eyes were prescribed BBFC, the right eye was used for the analysis of the IOP-lowering effect. Patients without changes in glaucoma medication or without ophthalmic surgery were evaluated for IOP during a 12-month period. Group A (n=86) comprised patients who switched from other glaucoma medications to BBFC and had no change in the number of ingredients before and after the medication change, group B (n=90) comprised patients who had an increased number of ingredients after the medication change (all patients had an increase of one ingredient) and group C (n=123) comprised patients who used BBFC along with other medications (increase of two ingredients). The patients evaluated for IOP at 3, 6, 9 and 12 months after the BBFC prescription were tested by using a paired t test, corresponding to the time of BBFC initiation, and a Kaplan-Meier survival curve analysis was performed, with discontinuation of BBFC due to adverse reactions defined as failure. Additionally, we evaluated the IOP response secondary to BBFC-induced allergic conjunctivitis. IOP at the start of BBFC, once before BBFC discontinuation and at the time of BBFC discontinuation were compared using a paired t-test in patients with BBFC-induced allergic conjunctivitis. Statistical analyses were performed using Statcel 4 (OMS Publishing, Tokyo, Japan).
Results
The patients’ background characteristics are shown in table 1.
Patient characteristics
IOP-lowering effect
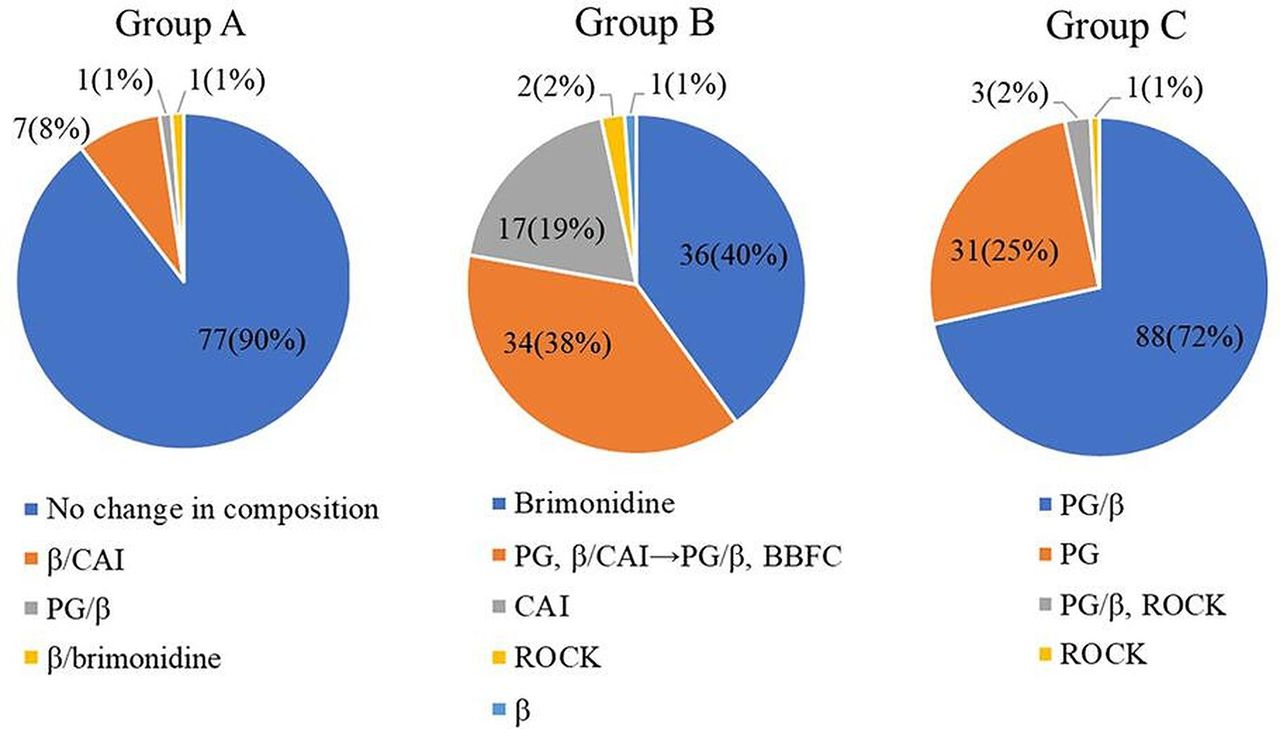
The profiles of eye-drops used before changing to BBFC are shown in figure 1. In group A, 90% of the cases had no change in the ingredients included before and after the treatment change from brinzolamide 1% and brimonidine 0.1% concomitantly to BBFC. In the remaining 10% of patients, β-blocker/carbonic anhydrase inhibitor (CAI) fixed combination, prostaglandin analogue (PG)/β-blocker fixed combination and β-blocker/brimonidine fixed combination were changed to BBFC in seven, one and one case, respectively. In group B, 40% of the patients switched from treatment with brimonidine alone to BBFC; 38% from PG and β-blocker/CAI fixed combination concomitantly to PG/β-blocker fixed combination and BBFC; and the remaining 22%, from CAI, Rho kinase inhibitor, or β-blocker alone to BBFC. In group C, BBFC was added to PG/β-blocker fixed combination and PG in 72% and 25% of patients, respectively. The mean number of ingredients in the glaucoma eye-drops before and after the treatment change was 3.8±0.6 in group A, increasing from 2.9±0.6 to 3.9±0.6 in group B, and from 1.8±0.5 to 3.8±0.5 in group C. The mean IOP (mm Hg) at the start of BBFC and at 3, 6, 9 and 12 months after the start of BBFC was 14.1, 14.0, 14.3, 13.5 and 13.8 in group A, 15.9, 14.4, 13.8, 14.1 and 14.5 in group B, and 17.2, 14.0, 14.1, 14.8 and 14.9 in group C, respectively (table 2). The mean IOP from before and after the treatment change at all time points showed no significant difference in group A, whereas groups B and C showed a significant decrease in IOP before and after the treatment change at all time points (p<0.05). A number of eyes in patients who were excluded from the IOP assessment were 6, 4 and 8 in groups A, B and C, respectively, because of skipped medical visits; 17, 15 and 18 in each group because of the addition of other glaucoma medications or glaucoma surgery because of poor IOP control; and 3, 2 and 3 eyes in each group because of the discontinuation of glaucoma medications, besides BBFC, secondary to side effects or temporary discontinuation of BBFC because of non-glaucoma surgery. The survival rates were 33%, 35% and 47% (p=0.27; log-rank test) at 12 months after the start of BBFC in groups A, B and C, respectively. This occurred when two consecutive IOPs exceeded the IOP at the start of BBFC (group A), two consecutive IOPs were <10% from the IOP at the start of BBFC (groups B and C), or when the addition of other glaucoma medications, or glaucoma surgery were defined as failures (figure 2A).
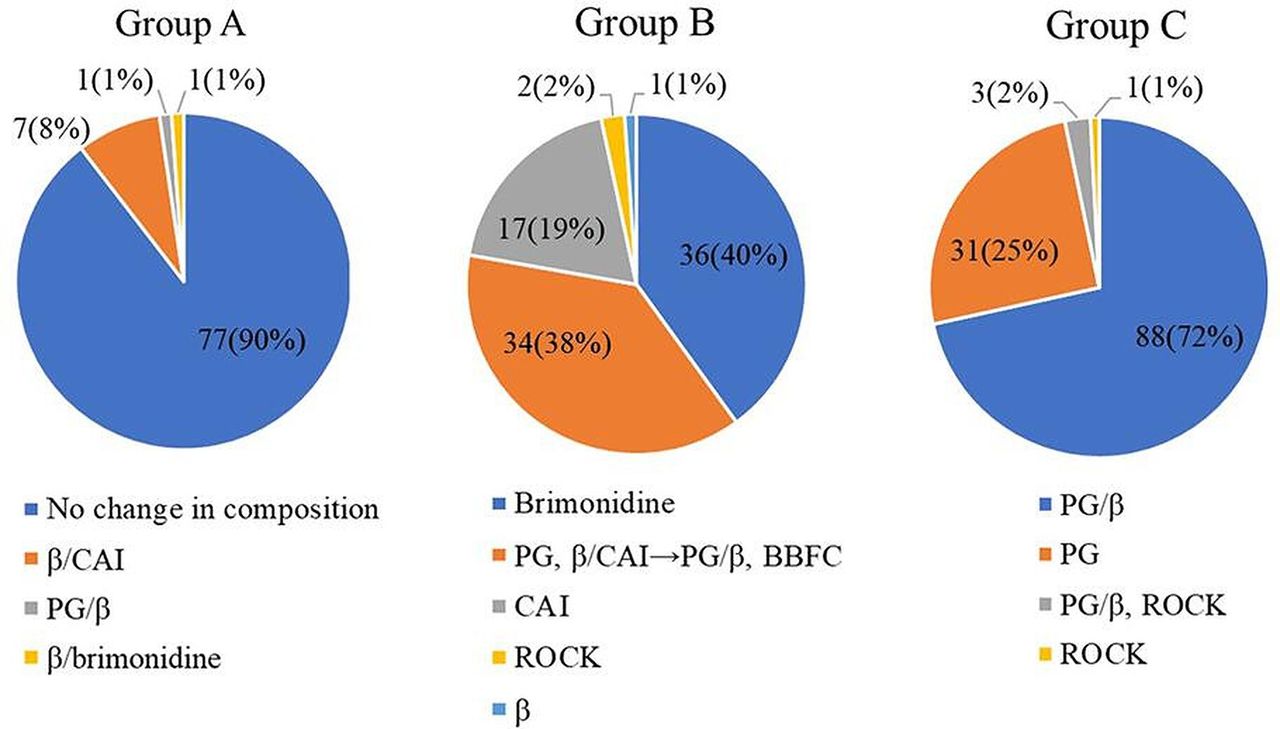
Details of the eye-drops used prior to BBFC prescription. BBFC, brinzolamide (1%)/brimonidine (0.1%) fixed combination; CAI, carbonic anhydrase inhibitor; PG, prostaglandin analogue; ROCK: Rho kinase inhibitor.
Intraocular pressure before and at 3, 6, 9 and 12 months after brinzolamide (1%)/brimonidine (0.1%) fixed combination prescription
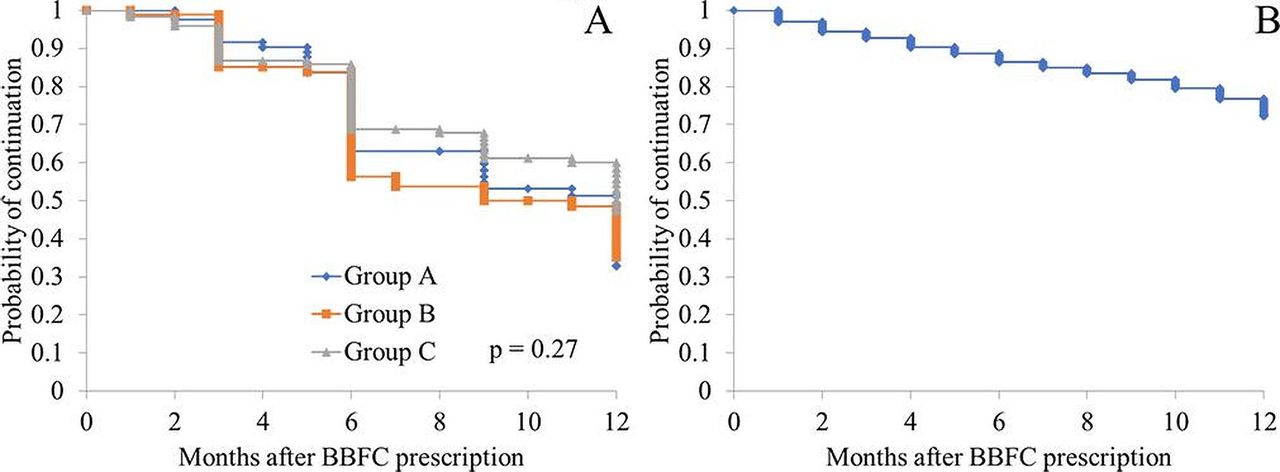
Kaplan-Meier survival curve analysis of IOP control in each group (B) Kaplan-Meier survival curve analysis of the discontinuation of BBFC due to adverse effects. BBFC, brinzolamide (1%)/brimonidine (0.1%) fixed combination; IOP, intraocular pressure.
Adverse reactions
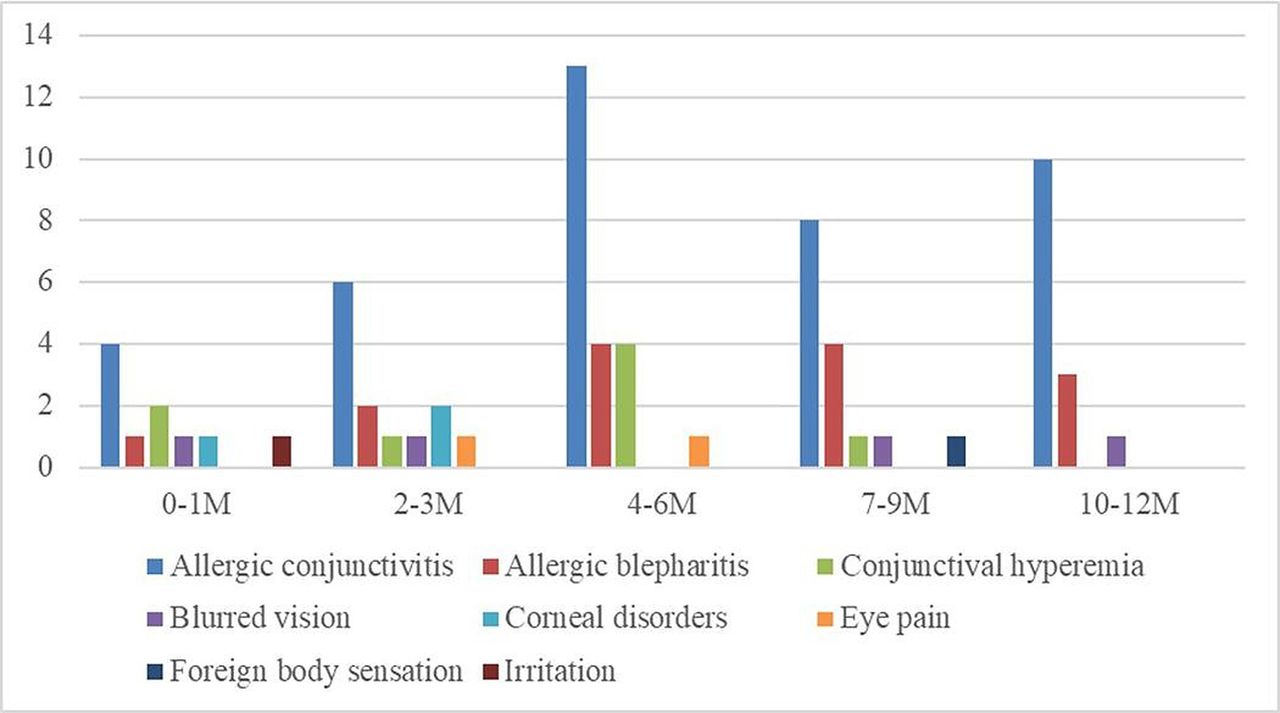
BBFC was discontinued due to the development of adverse reactions during follow-up and reasons other than adverse reactions in 73 (18%) and 68 (17%; glaucoma surgery in 56 cases, good IOP in 12 cases) cases, respectively. The local ocular adverse reactions (with duplicates) and onset time of each adverse reaction are shown in figure 3. Allergic conjunctivitis was seen in 41 eyes, allergic blepharitis in 14 eyes, conjunctival hyperaemia in 8 eyes, blurred vision in 4 eyes, corneal disorders in 3 eyes, eye pain in 2 eyes, and foreign body sensation and irritation in 1 eye each. The survival rates were 93%, 86%, 82% and 72% at 3, 6, 9 and 12 months after the start of BBFC, respectively, when discontinuation due to adverse reactions was defined as failure (figure 2B).

{kind=link}
{kind=link}
{kind=link}
Time of onset of adverse reactions.
Allergic conjunctivitis and IOP-lowering effect
The IOP at the start of BBFC in the 41 eyes with allergic conjunctivitis was 15.3 mm Hg. The IOP at the one visit before discontinuation of BBFC because of allergic conjunctivitis was 14.2 mm Hg, which was significantly lower than that at the start of BBFC (p<0.05). The IOP at the time of discontinuation was 14.5 mm Hg, which was not significantly different from that at the start (p=0.055) and at the time of discontinuation compared with the IOP one visit before discontinuation (p=0.81).
Discussion
In this study, there was no significant difference in IOP from baseline to after the treatment change at all time points in group A (switched from other glaucoma medications to BBFC and had no change in the number of ingredients). In groups B (switched from other glaucoma medications to BBFC and had an increase in one ingredient) and C (two ingredients were added by BBFC to other glaucoma medications), the IOP was significantly lower after the treatment change at all time points than that before the change. Allergic conjunctivitis was the most common adverse reaction with a rate of 10%, followed by allergic blepharitis and conjunctival hyperaemia. Adverse reactions occurred at any time point from as early as 1 month after the start of BBFC to as late as 12 months.
Previous reports have reported on the IOP-lowering effect of BBFC, similar to that shown by group A in this study. Onoe et al12 reported no significant difference in IOP when changing from brinzolamide 1% and brimonidine 0.1% concomitantly to BBFC at 4 and 12 weeks before and after the change. A randomised controlled trial of the combination of brinzolamide alone and 0.2% brimonidine concomitantly and BBFC reported no difference in IOP-lowering efficacy.14 Moreover, in a study on the IOP-lowering efficacy of BBFC among patients with normal tension glaucoma, Jin et al15 reported that a change from brinzolamide and brimonidine concomitantly to BBFC resulted in no significant difference between the mean IOP of 12.4±1.4 mm Hg before the change and 12.6±1.5 mm Hg after the change to BBFC. Similarly, Inoue et al13 reported no significant difference in IOP at 3 and 6 months after switching from brinzolamide 1% and brimonidine 0.1% concomitantly to BBFC. Kozobolis et al16 investigated the changes from other ingredients compared the dorzolamide/timolol fixed combination with the BBFC. The mean morning IOP reduction was 7.0±2.8 and 8.4±1.9 mm Hg for dorzolamide/timolol fixed combination and BBFC, respectively, showing a significant difference, whereas the mean afternoon IOP reduction was 8.6±2.7 and 7.9±1.6 mm Hg, respectively, showing a non-significant difference. In the present study, group A had the same IOP before and after treatment change at any time point, similar to the finding of previous reports. However, considering that a smaller number of drugs leads to improved adherence,8 9 the reported efficacy of using combination drugs rather than single agents concomitantly,15 17 and the benefits of using combination drugs for severe ocular surface disease,15 it is considered effective to switch from a single-agent combination to BBFC, as in the treatment received by group A.
Previous studies have also reported on cases similar to our group B cases. In a phase III clinical trial conducted in Japan, at 4 weeks after switching from brimonidine 0.1% alone or brinzolamide alone to BBFC, the IOP was significantly lower, as compared with that before the switch.10 11 Comparing brinzolamide 1% alone or brimonidine 0.2% alone with a combination of both at 6 months after initiation, Aung et al18 reported that the IOP was significantly lower from baseline in all groups, and the fixed combination produced significantly better IOP reduction than treatment with brinzolamide alone or brimonidine alone. The study by Inoue et al13 involving patients with primary open-angle glaucoma and ocular hypertension who also switched from brinzolamide 1% alone or brimonidine 0.1% alone to BBFC, both patient groups showed a significantly lower IOP after the change. Jin and Lee15 reported that the mean IOP of patients with normal tension glaucoma who switched from brinzolamide 1% alone to BBFC decreased from 13.4±1.6 mm Hg to 12.3±1.4 mm Hg, whereas the mean IOP of those who switched from brimonidine 0.2% alone to BBFC decreased from 13.3±1.6 mm Hg to 12.4±1.4 mm Hg, with the IOP significantly lower in both groups after the change to BBFC. In group B of the present study, the brimonidine or brinzolamide component was added in 87 of the 90 cases due to the treatment change to BBFC, and, as in previous reports, significant IOP reductions were obtained at any time point after the BBFC prescription. Other glaucoma eye-drops, such as PG and β-blockers, were already used before the change to BBFC, and the mean number of components before the change was 2.9. Compared with cases with untreated IOP, the IOP had already decreased. Therefore, achieving IOP reduction may be more difficult with BBFC. However, based on the results of the present study, further IOP reduction can be expected even with an increase in only one component from the status treated with other glaucoma eye-drops, and treatment intensification with BBFC is an effective means of treatment.
Finally, previous studies have also reported on cases similar to our group C cases. Jin and Lee15 reported that in a study involving cases of normal tension glaucoma treated with BBFC, the mean IOP decreased from 17.1±1.4 mm Hg to 12.4±1.8 mm Hg. In a study of the efficacy of a combination of travoprost/timolol with the addition of BBFC, Lerner et al19 found a 4.25 mm Hg reduction of IOP after 6 weeks of treatment from baseline of 21.6 mm Hg, which was significantly better than that of the control group. Topouzis et al20 added a combination of brinzolamide (1%)/brimonidine (0.2%) to PG and reported that the IOP reduced to 5.59 mm Hg from the baseline of 22.8 mm Hg after 6 weeks of treatment, as compared with that of the control group, showing a significant difference. Fechtner et al21 and Feldman et al22 also have shown that adding BBFC to PG resulted in a significant IOP reduction. Group C in the present study also showed a significant decrease in IOP at any time point after the addition of BBFC, similar to the finding of the previous report. In group C, 88 of the 123 patients were treated with BBFC in addition to PG/β-blocker fixed combination. Considering the advantage of having four ingredients in two bottles of eye-drops, BBFC is an effective option as a second eye-drop to be used when intensifying treatment. In addition, BBFC was added 31 eyes treated with PG, as in previous reports,20–22 which may be an effective treatment intensification option for patients with asthma, chronic obstructive pulmonary disease and cardiac disease.
Regarding adverse reactions, conjunctival hyperaemia was reported to be the most common at 5.5%, followed by allergic conjunctivitis at 3.1%,14 and allergic conjunctivitis, allergic blepharitis and conjunctival hyperaemia were the top three adverse reactions in the present study, with similar results. These adverse reactions were relatively common complications reported in other previous reports.13 21 23 24 Discontinuations due to adverse reactions occurred at any time from within 1–12 months after the start of BBFC, and the Kaplan-Meier survival curve analysis showed no significant decline in the probability of continuation at any particular time, but rather a steady decline. Therefore, regardless of the length of the BBFC eye-drop treatment period, attention should be paid to the appearance of adverse reactions at any time.
Yeh et al reported that patients who received brimonidine monotherapy showed significantly increasing IOP after they experienced brimonidine allergy, except those who had multiple therapies with brimonidine.25 Our cohort was treated with multiple therapies which our results support.
The present study has several limitations. First, patients receiving other glaucoma medications or who had undergone glaucoma surgery due to inadequate IOP reduction during the course of the study were excluded from the IOP evaluation. Therefore, the IOP-lowering effect of BBFC may have been overestimated. Second, the IOP-lowering efficacy in each type of glaucoma has not been evaluated. Third, regarding the evaluation of adverse reactions, allergic conjunctivitis, which was the most common adverse reaction, included some cases that were difficult to clearly distinguish from allergic conjunctivitis caused by other substances, such as seasonal ones. Therefore, the adverse reactions may have been overcounted.
In conclusion, in groups B and C, in whom additional ingredients were added, the IOP was significantly lower at all time points after the BBFC prescription. The IOP in group A (no change in the number of ingredients) was similar before and after the treatment change. BBFC is a good option in terms of improving eye-drop adherence owing to the use of a combination eye-drop. Additionally, we should pay attention to the drop-outs due to the adverse reactions at any time after the start of BBFC.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board (IRB) of Saneikai Tsukazaki Hospital (approval nos. 221003 and 221004). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank Enago (https://www.enago.jp) for English language editing.
References
Footnotes
RA and SN contributed equally.
Contributors RA and SN contributed equally to this paper. RA and SN made substantial contributions to the design and analysis of this work. RA and SN contributed to the conception and design of the study, data analysis, and drafting of the manuscript. ET, SD, MS, SO, KU, YK and YN contributed to the data acquisition. All the authors approved the final manuscript. RA is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.