Article Text

Statistics from Altmetric.com
Shedding of SARS-CoV-2 in tears of patients with COVID-19 has been reported,1 2 which could serve as a source of infection for healthy individuals, including healthcare providers. The current standard antiseptic solutions used in ophthalmology in the setting of inoffice procedures and operating rooms include povidone-iodine (PVI) 5% and chlorhexidine gluconate (CHX) 0.1% or 0.05%, which are at concentrations that are lower than those used in other surgical specialties. Although laboratory and clinical studies to date have aimed to evaluate the virucidal benefits of routine PVI use for ophthalmic surgeries,3 currently there are no established guidelines regarding the optimal contact time and efficacy of varying dilutions as well as comparisons with other formulations such as CHX. Rigorous evaluation of the efficacy of virucidal agents for disinfecting ocular surface of potentially infected patients with SARS-CoV-2 is critical in mitigating the risk of transmission.
In the current study, we evaluated the virucidal efficacy and contact times for commonly used ophthalmic concentrations of PVI and CHX against SARS-CoV-2 using Vero E6 cells as indicator cell lines for residual viable virus based on previously established methodologies (online supplemental appendix).4–6 PVI (5% weight per volume, w/v) and CHX (0.05% and 0.1% w/v) were tested at full strength. Fifty microlitres of ophthalmic formulations were added to 10 µL of a SARS-CoV-2 suspension (viral transport media) and incubated at room temperature for varying contact times. A total of three experiments were conducted for PVI and CHX, each including three biological replicates per time point. Individual viral titres for each biological replicate were calculated based on five replicate wells per dilution. Viable residual SARS-CoV-2 was quantified by the Reed-Muench median tissue culture infectious dose (TCID50) procedure in Vero E6 cells.7 Additional efficacy testing using 1:4 and 1:16 dilutions in phosphate buffered saline were performed in order to mimic clinical settings where dilution of the formulations occurs as a result of mixing with patients’ ocular secretions. Cytotoxicity of residual PVI and CHX was predetermined at all test concentrations using uninfected Vero E6 cells.
Supplemental material
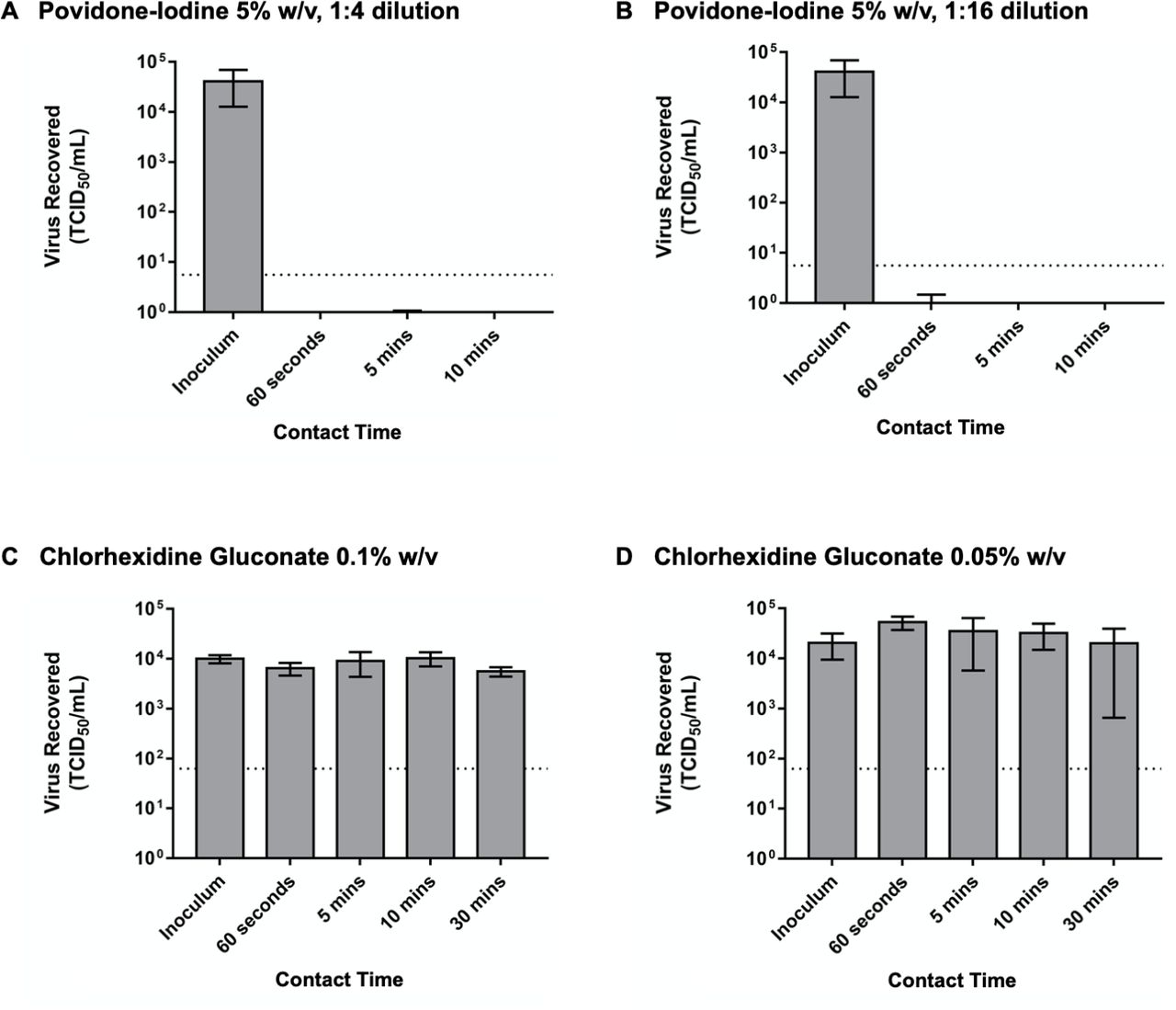
No SARS-CoV-2 was detected with PVI at full strength and 1:4 dilution after 60 s, 5 min and 10 min of contact time (figure 1). The 1:16 PVI dilution substantially decreased viral titres after 60 s of contact time (4.45, SD 0.44 vs 0.12, SD 0.24 log10 TCID50/mL, 95% CI of difference 3.53 to 5.13, p<0.001). No virus was recovered from the inoculated suspensions after 5 and 10 min of contact time with the 1:16 PVI dilution. Full strength CHX 0.1% (3.99, SD 0.08 vs 3.74, SD 0.10 log10 TCID50/mL, 95% CI 0.04 to 0.46, p=0.03) and CHX 0.05% (4.3, SD 0.5 vs 4.53, SD 0.44 log10 TCID50/mL, 95% CI −1.30 to 0.84, p=0.58) concentrations did not result in SARS-CoV-2 inactivation even after 30 min of contact time.
{kind=link}
Virucidal efficacy of ophthalmic formulations of povidone-iodine (PVI) and chlorhexidine gluconate (CHX) against SARS-CoV-2. (A and B) Mean (±SD) titre of the positive control (inoculum, 0 min contact time) and the postneutralisation samples (60 s, 5 min and 10 min contact time) with PVI 5% at 1:4 and 1:16 dilutions, respectively. (C and D) Mean (±SD) titre of the positive control (inoculum, 0 min contact time) and the postneutralisation samples (60 s, 5 min, 10 min and 30 min of contact time) with CHX 0.1% and 0.05%, respectively. The horizontal dashed lines indicate the limit of detection (LOD) of the assay. Note that the LOD is higher for CHX (1.8 log10 TCID50/mL) than PVI (0.8 log10 TCID50/mL) due to its cytotoxicity on Vero E6 cells. TCID50, tissue culture infectious dose; w/v, weight per volume.
The findings from this in vitro study demonstrate that PVI at commonly used ophthalmic concentration of 5% has greater virucidal activity than CHX against SARS-CoV-2 in inoculated suspensions, with CHX proving to be ineffective at full concentration of 0.1% even after 30 min of contact time. The virucidal benefits of routine PVI in reducing patients’ ocular surface viral load may be effective at 1:16 of the initial concentration with only 60 s of contact time. It is important to note that CHX 0.1% w/v is at the upper limit of the concentration commonly used in ophthalmic procedure settings. These findings are in keeping with previous findings which have shown the efficacy of PVI in managing upper respiratory tract infections and suggested the use of PVI on the sinonasal and oral mucosa against the transmission of SARS-CoV-2.8 Overall, this study has important implications for clinicians when selecting an ophthalmic solution for routine procedures that reduces transmissibility of SARS-CoV-2 via ocular secretions among patients and healthcare providers. The adoption of guidelines for ophthalmic surgeries such as lacrimal surgeries using PVI may be useful in decreasing viral burden in the setting of the COVID-19 pandemic and other viral infections.
Ethics statements
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design: TF, TM, TAC. Data collection: TF, SBK, JK, TAC. Analysis and interpretation: TF, SBK, JK, TAC. First manuscript draft: TF. Critical revisions of the manuscript: TF, SBK, JK, SRE-D, TM, TAC. Obtained funding: JK, TAC. Overall responsibility: TF, TAC.
Funding This work was funded through a Collaborative Research Agreement with the Public Health Agency of Canada. The authors did not receive non-governmental support.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.