Article Text

Abstract
Objective Clear information is essential to properly determine preference in medical intervention. In neovascular age-related macular degeneration, patients need to understand the balance of risk and benefit of anti-vascular endothelial growth factor (VEGF) treatment. This balance is altered by the number of injections administered.
Methods Natural frequencies, displayed as pictographically as icon arrays, are used to show material outcomes from the MARINA and HARBOR (12 months) trials. We also calculated the number needed to treat (NNT) and number needed to harm (NNH).
Results MARINA 24-month data show the absolute risk reduction is 37% and the NNT is 3; meaning for one patient to benefit three need to be treated.
12 months’ HARBOR data show that compared with as-needed treatment, scheduled monthly injection treatment increases the number of patients achieving a better visual outcome. The number of patients suffering harm is also increased by the additional injections.
Conclusion Displaying MARINA and HARBOR trial data as natural frequencies, with numbers needed to treat and harm, communicates complimentary information on the positive and negative aspects of anti-VEGF treatment.
- macula
- neovascularisation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Intravitreal anti-vascular endothelial growth factor is an effective treatment for neovascular age-related macular degeneration.
What are the new findings?
Restating landmark publications as natural frequencies enhances appreciation of the balance of risks and benefits; specifically that although more injections provide better visual outcomes, risk also increases. The risks may well come to exceed benefit earlier than is currently appreciated.
How might these results change the focus of research or clinical practice?
Authors of these and other publications should consider reviewing their data to more precisely delineate the balance of risk and benefit.
The Montgomery decision says, the ‘doctor is under a duty to inform the patient of the material risks inherent in the treatment,’ any change in the balance of risk and benefit with repeated injections is material and patients need to understand if, how and when this balance changes.
Introduction
Neovascular age-related macular degeneration (nv-AMD) or wet AMD can be considered as an acute exacerbation of an underlying chronic disease state: dry AMD. nv-AMD affects only 10% of all AMD sufferers but is disproportionately disabling. Vision is lost as a result of abnormal, leaky blood vessel development, which damages the macula.
Bevacizumab (Avastin), ranibizumab (Lucentis) and aflibercept (Eylea) are available treatment options, delivered as intravitreal injections. These drugs block vascular endothelial growth factor (VEGF) and stop the new blood vessel from growing and leaking, but do not benefit the underlying dry AMD. The National Institute for Health and Care Excellence website features ranibizumab (Lucentis) in AMD pharmacological treatments,1 with the comment that there are ‘…no clinically significant differences in effectiveness and safety is between the different anti-VEGF treatments.’ For this reason, we confine our consideration of risks and benefits to ranibizumab (Lucentis).
Accessible information on the risks and benefits may be confusing for patients considering anti-VEGF treatment, possibly due to the way the information entered the public domain. The New York Times first reported successful treatment for nv-AMD with anti-VEGF on 19 July 2005; ‘Genentech Says Drug Restores Vision,’2 the report detailed ‘Lucentis restored patients' vision …(with) …an average gain of seven letters …compared with a 10.5-letter loss for …placebo.’ Ranibizumab (Lucentis) was not commercially available at that time but ophthalmologists in the USA and the UK had already begun using bevacizumab (Avastin—ranibizumab’s parent molecule) ‘off-label’3 to treat nv-AMD from about 2005.
Food and Drug Administration (FDA) approval and commercial availability of Lucentis followed the FDA’s June 2006 press release.4 ‘The FDA Approves New Biologic Treatment for Wet Age-Related Macular Degeneration’—which explained:
Lucentis (ranibizumab) is the first treatment which, when given as a dose each month, can maintain the vision of more than 90% of patients with nv-AMD.
Ninety-five per cent of patients who received a monthly injection maintained their vision compared with 60% of control patients.
One-third of patients had improved vision after 12 months.
After 24 months, these findings were maintained with continued monthly doses of Lucentis.
Serious adverse events were rare and related to the injection procedure, for example, inflammation, retinal detachment and cataracts.
This and other media announcements meant that many became aware of the benefits of ranibizumab (Lucentis) treatment more than a year before the evidence for these assertions was available for scrutiny. The MARINA randomised controlled trial was published on 5 October 2006 and supported claims for the benefits of ranibizumab (Lucentis). These notions seem now to have entered the collective unconscious and have become unchallengeable.
The level of evidence MARINA provided, and this remains the only treatment –v- no treatment study of anti-VEGFs, ought to have made a 24 injection in 2 years treatment schedule the norm - as was the case in the later HARBOUR study.5
However, this ran contrary to the experience of Avastin early adopters who knew that only two to four injections of Avastin were needed to produce a worthwhile outcome.6 Also, the 2009 PrONTO study7 showed ‘variable-dosing regimen with intravitreal Ranibizumab (Lucentis) resulted in VA outcomes comparable with the outcomes from… MARINA…, but fewer intravitreal injections were required.’
In real-world practice, a PrONTO-like ‘treat and extend’ regimen has become familiar, patients currently receive a mean of 5.0 and 2.2 ranibizumab (Lucentis) injections in the first and second year, respectively,8 considerably less than MARINA’s 24 injections, in 2 years of treatment.
Ranibizumab (Lucentis) treatment also exposes patients to risk of harms to their eyes and general health. The Montgomery decision of the Supreme Court9 in 2015 set out, ‘The correct position, in relation to the risks of injury involved in treatment…. An adult person of sound mind is entitled to decide which, if any, of the available forms of treatment to undergo, and her consent must be obtained before treatment interfering with her bodily integrity is undertaken.’ The judgement continues, (the) ‘doctor is under a duty to inform the patient of the material risks inherent in the treatment. A risk was material, for these purposes, if a reasonably prudent patient in the situation of the patient would think it significant.’ The decision quotes directly from the General Medical Council’s Good Medical Practice,10 ‘Give patients the information they want or need in a way they can understand.’
In the management of nv-AMD, anti-VEGF injection is a decision for the patient to make. This obliges the ophthalmologists to share with their patients material information that is comprehensible. This information derives from clinical trials, reliant on properly collected data, which are then statistically analysed and presented in scientific journals. This can be a barrier to understanding for those who do not have the high statistical literacy. Gigerenzer11 has shown how even expressing results as percentages can produce a math’s puzzle that will cloud the minds of many people, including health professionals, who then may inadvertently impart misleading advice to their patients.
Natural frequencies are a joint frequency of two events,12 such as the number of patients with disease who respond to treatment or no treatment. Using natural frequencies is an alternative to presenting the same information as statistically analysed means, distribution intervals and percentages. Presenting material information using natural frequencies graphically can overcome many of the cognitive biases that inhibit accurate consideration of statistical information.13 Herein, we explain how we used data from MARINA and HARBOR to produce icon arrays to provide patients with information on the benefits of ranibizumab (Lucentis) treatment, the inherent risks and their magnitudes.
Materials and methods
We reviewed the MARINA and HARBOR studies. The MARINA study was used as it provides guidance on whether a patient should choose to accept treatment with anti-VEGF for nv-AMD, and HARBOR because it provides information that can guide on how many injections a patient should choose to accept.
From each study’s results section relevant outcome data were entered into prerelease Factarray software.
The Factarray app is a decision aid for consent. It is designed to ensure that both the physician and the patient share the same understanding of the risks and benefit inherent in any intervention; in this instance, nv-AMD treatment with anti-VEGF. The clinician can input data into the software using the highest available level of evidence on any intervention. The app will generate a list of facts on the intervention, a pictographic icon array allowing comparison of outcomes in the situation under consideration, for example, treatment versus no treatment; also basic data, number of patients needed to treat to produce each harm or benefit.
Each colour-coded dot in the icon array represents the experience 1 out of 1000 similar patients.
Results
The MARINA study, at 24 months, showed that 90% of those treated with monthly Lucentis 0.5 mg achieved the primary or secondary outcome measure, by either losing fewer than or gaining 15 Early Treatment Diabetic Retinopathy Study letters (figure 1).

MARINA 24-month data; each dot on this icon array represents the experience of each one of a thousand patients. Benefits are coloured green, death is coloured black, harms are coloured red (when the frequency of an event—in this case visual benefit—exceeds 50% of subjects, the colour surrounds the dot rather than fills it). CVA, cerebrovascular accident; MI, myocardial infarction.
The absolute risk reduction (ARR) is the difference the treatment makes and is the difference between that 90% and the 52.9% of untreated subjects who achieved the same result: in this case 37%.
The reciprocal gives the number needed to treat (NNT)–3, meaning, for every three people treated with 24 Lucentis injections one person will achieve the trial benefit.
The harms are higher in the treated group: 1 in 26 of this group died compared with 1 in 40 controls, 1 in 29 suffered an ocular adverse event compared with 1 in 83 controls, 1 in 58 suffered a stroke compared with 1 in 125 controls.
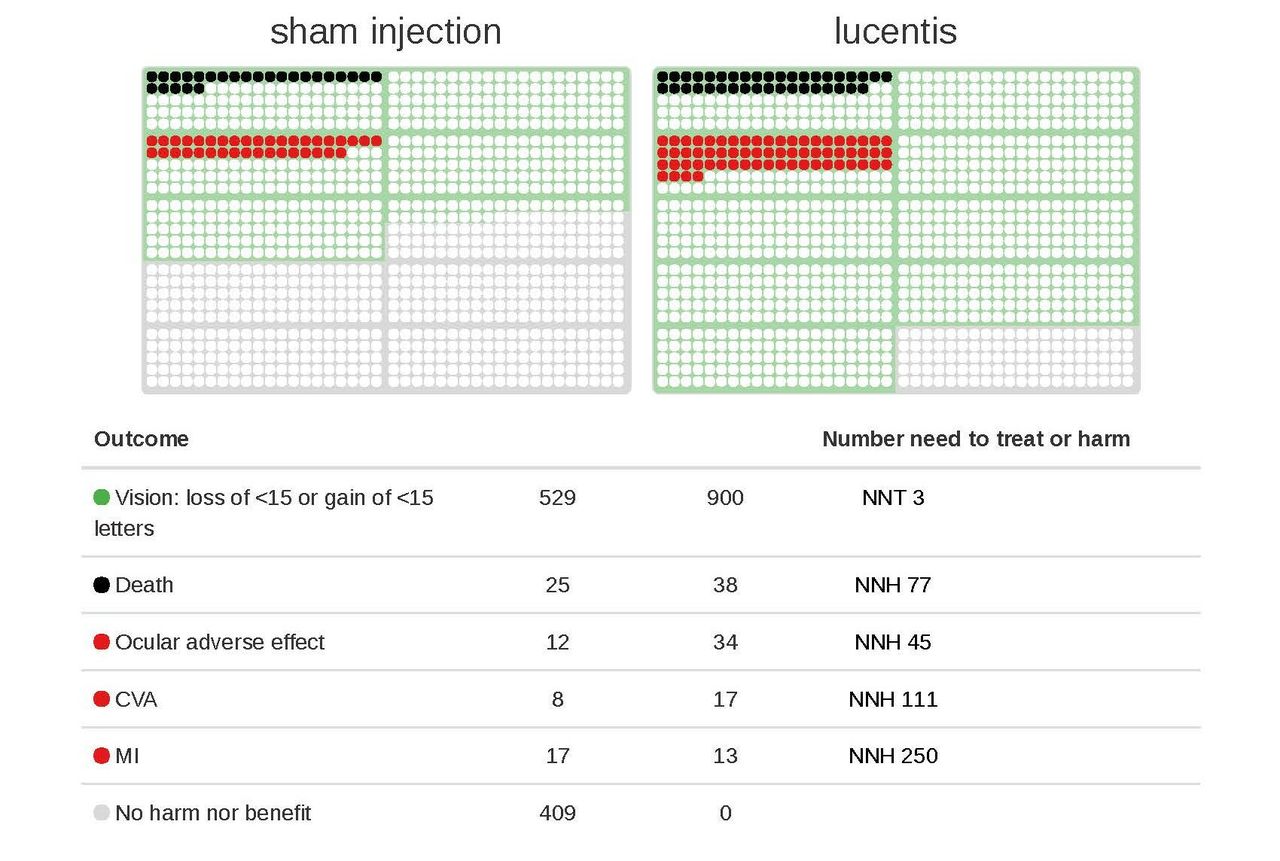
The HARBOR study evaluated the efficacy and safety of intravitreal ranibizumab (Lucentis) 0.5 and 2.0 mg administered monthly and on an as-needed (PRN, pro re nata) basis in treatment-naïve patients with subfoveal nv-AMD (wet AMD). The study confirmed 0.5 mg as the optimum ranibizumab (Lucentis) dose. Because patients could ‘crossover’ after 12 months’ efficacy and safety information is only valid up to 12 months. These 12-month data allow comparison of benefits and harms between those who underwent 12 scheduled monthly injections compared with PRN patients who had a total of six injections in the first 12 months after diagnosis.
From HARBOR at 12 months: the ARR was 3.3%. This being the greater percentage of those subjects treated with 12 ranibizumab (Lucentis) 0.5 mg injections who achieved the primary or secondary outcome measure by either losing fewer than or gaining 15 EDTRS letters (figure 2) than those treated with six injections. The reciprocal is the NNT of 30. This means 30 patients need to be treated with monthly rather than PRN injections for one such patient to benefit.

{kind=link}
{kind=link}
HARBOR 12-month data; each dot on this icon array represents the experience of each one of a thousand patients. Benefits are coloured green, death is coloured black, harms are coloured red (when the frequency of an event—in this case visual benefit—exceeds 50% of subjects, the colour surrounds the dot rather than fills it). CVA, cerebrovascular accident; MI, myocardial infarction.
The additional harms per thousand for the six additional injections in the first 12 months of the study are: 14 deaths, 15 heart failures, 3 strokes, 7 endophthalmitis and 15 myocardial infarctions.
Discussion
The form in which the authors of the MARINA and HARBOR originally presented information caused difficulties. MARINA reported relative risk reduction but reported neither ARR nor the NNT. This is contrary to clause 7 of the Association of the British Pharmaceutical Industry Code of Practice14 that mandates outcome expressed as ARR and NNT and says: ‘Referring only to relative risk, especially with regard to risk reduction, can make a medicine appear more effective than it actually is. In order to assess the clinical impact of an outcome, the reader also needs to know the absolute risk involved. In that regard relative risk should never be referred to without also referring to the absolute risk.’
There are other potential sources of confusion. MARINA commented on the benefit of only the first injection, ‘the mean improvement from baseline in visual acuity scores was evident 7 days after the first injection.’
MARINA did not discuss the relative benefits or the harms experienced after each of any of the remaining 23 injections. This may have invited an assumption; that repeated injections are essential to maintain visual improvement and that this imperative outweighs the inherent risk of repeating treatment.
MARINA did not publish the absolute number of letters read and only the change in the number of letters read since baseline. The AURA10 observational study did, saying, ‘Visual acuity: change from baseline… an improvement in (mean) visual acuity was observed until about day 120 thereafter visual acuity noticeably decreased.’10 This seems to suggest the response of nv-AMD to anti-VEGF treatment may be greatest during the early stages of the disease.
When the New York Times reported first on AMD treatment, ‘Laser use reported effective in averting Blindness in The Elderly,’15 they emphasised the short window of opportunity for treatment to be effective, ‘The results are so promising that The NEI…(The USA National Eye Institute—the trial’s sponsors)… took the unusual step of disclosing them at a news conference to spread the word quickly. It has also terminated further clinical tests and today urged all potential patients to seek laser treatment promptly… The results demonstrated that early treatment was essential. Of the cases in which diagnosis was made within two weeks of the onset of symptoms, 83 percent were still treatable. In contrast, only 10 percent could be treated if five to six months had elapsed.
It seems difficult to reconcile the idea of laser treatments being most effective in the early months of nv-AMD’s natural history with MARINA’s conclusion that ‘Lucentis treatment is needed for two years.’
Genentech’s current ‘Lucentis’ data sheet16 may reinforce this notion, ‘LUCENTIS 0.5 mg (0.05 mL) is recommended to be administered by intravitreal injection once a month (approximately 28 days).
Although not as effective,patientsmay be treated withthreemonthly doses followed by less frequent dosing with regular assessment. Although not as effective,patientsmay also be treated with one dose every3monthsafterfourmonthly doses.Patientsshould be assessed regularly.’
‘Although not as effective’ suggests to us that patients may be disadvantaged by not having enough treatments, but this statement is not balanced by considering the possible harms of additional treatment.
The IVAN14 study—comparing safety and efficacy of Lucentis to Avastin—reports a similar level of serious harm at about 4%–7% of patients. The HARBOR8 study found 2.6%–3.6% risk of serious harm to the eyes, with serious harm to general health developing in about 4% of those treated with Lucentis. Our presentation of HARBOR 12-month data shows the harms are greater with more injections, so much so that the harms exceed the benefits of the six additional injections in the first year. This is contrary to HARBOR’s conclusion that Lucentis ‘dosed monthly provided optimum results in patients with wet AMD,’ and seems to take no account of the additional harms. We did not access any unpublished HARBOR data and so cannot assist patients in deciding the optimum number of injections or how long treatment ought to be given. We feel that perhaps our presentation ought to be considered alongside AURA’s observation that following inception of monthly treatment vision falls from day 120, which would be after a fifth monthly injection. This may be a pointer that suggests the average of nine Lucentis injections in total10 may be supraoptimal.
We feel expressing information as an icon array improves clarity on material outcomes of MARINA and HARBOR. The pictographs show the information in an unbiased and easy-to-understand17 form. Each dot on an icon array represents the experience of each of 1000 patients. When an event occurs frequently (>50% of those studied) the indicator colour surrounds the dot rather than fills it. An icon array requires no mathematical training to understand and improves perception of likelihood in people with lower numerical aptitude.18
The impression gained from viewing the icon array is more representative of the likely risk and benefit than information from other sources.
Icon arrays improve accuracy of estimation of relative risk reductions when added to numerical descriptions without increasing perceived seriousness of risk19 although others found icon arrays increased the perception of seriousness.20 The Factarray app allows all benefits and all harms to be grouped in single colour. This is done in figure 1 benefits in green and harms in red but these can be individualised in different colours to avoid suggesting each benefit (or harm) is of equal weight by using different colours for each benefit or harm—see figure 2.
Perception of likelihood using a 1-in-X format is assimilated faster and yields higher perceived likelihoods and appears to be the easiest format to interpret. The effect of adding graphs on perceived likelihood primarily assists people with lower numerical aptitude.15
A key point of this communication is that the decision over treatment is for the patient to make, and each individual will balance risk against benefit from their own perspective. When we used figure 2 as part of our consent process, an audit21 showed appointments for clinical assessment decreased by 40% and there was a 27% reduction in the number of intraocular injections given. We felt our patients may have chosen to forgo any benefit of additional anti-VEGF injections, and decided instead to prioritise reducing the risk of adverse events: ocular injury, myocardial infarction, heart failure and cerebrovascular accident instead.
Jawetz22 recognised four phases in the history of a drug:
Initial optimism causing heavy usage.
High-level usage.
Low use because of disappointment from unexpected consequences.
Finally, stabilisation at a moderate usage level.
Some 12 years since being introduced, anti-VEGF medication for nv-AMD seems to us to currently be between phases 1 and 2. Setting out the balance of risk and benefit more clearly in this way may help patients in determining their own preference for anti-VEGF treatment.
We also hope to stimulate other authors to re-evaluate their existing trial data in order to establish the balance of benefit and risk; injection by injection. It may then be possible to use this information to allow patients to determine, more precisely than we have been able, their own optimum number of injections; where benefit ceases, from their perspective, to exceed risk and what the factors are which alter that point.
Acknowledgments
The authors gratefully acknowledge the assistance of Paul Newcombe of MRC Statistics Unit, Cambridge University, for reviewing this manuscript and suggesting improvements.
Footnotes
Contributors Conception or design of the work: LC, BR, JW, ST. Data collection: LC, BR. Data analysis and interpretation: LC, BR, JW, ST. Drafting the article: LC. Critical revision of the article: LC, BR, JW, ST. Final approval of the version to be published: LC, BR, JW, ST.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.