Article Text

Abstract
Objective Charles Bonnet syndrome (CBS) is defined as an occurrence of visual hallucinations (VHs) in the absence of any psychiatric/neurological disorder. Significantly reduced vision due to age-related macular degeneration (AMD), cataract or glaucoma is the most common cause for CBS. Aim of this randomized controlled study was to assess whether additional treatment by a psychiatrist is beneficial for patients with CBS.
Methods and Analysis Patients with visual acuity of 0.5 LogMAR or worse in the better eye were screened. Instruments used were an interview asking about details of the VH, a mental test and a questionnaire on quality of life. Patients with CBS were randomised into two groups: in group 1, a patient-doctor consultation was performed by an ophthalmologist, and in group 2 a consultation and, if needed, additional medical assessment and treatment was given by a psychiatrist.
Results 4900 patients were screened. 390 patients met the inclusion criteria and among these a CBS prevalence of 34 patients (8.7%) was found. The female-to-male ratio was 4:1 and the average age was 79.3 ± 9.7 years. Four different types of VH were observed: 41% humans (n=14), 32% geometrical shapes/patterns (n=11), 15% plants (n=5) and 12% animals (n=4). The change in quality of life in patients with CBS was not significantly different in both groups (p=0.727, ophthalmologist: n=18, psychiatrist: n=16).
Conclusion It is essential for medical staff involved with patients suffering from severe vision loss to be aware of CBS. This will help to better identify and interpret symptoms and could also lead to a more adequate treatment for affected patients.
Discussion It is essential for medical staff involved with patients suffering from severe vision loss to be aware of CBS. This will help to better identify and interpret symptoms and could also lead to a more adequate treatment for affected patients.
- clinical trial
- degeneration
- macula
- pathology
- physiology
- psychophysics
- public health
- visual perception
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with severe loss of vision (eg, due to age-related macular degeneration, cataract, glaucoma) may suffer from visual hallucination (VH).
VHs are often associated with mental illness and patients are afraid to tell medical staff about it.
What are the new findings?
This is the first randomised controlled study which shows the quality of life for patients with Charles Bonnet syndrome (CBS) after a discussion with a psychiatrist or with an ophthalmologist.
This paper provides all known diagnostic, inclusion and exclusion criteria which can be found in current literature.
A relative high prevalence of CBS could have been found in this Austrian hospital.
How might these results change the focus of research or clinical practice?
Increased awareness of CBS is necessary for medical staff and patients with vision loss. This will make it easier to identify and interpret symptoms correctly and also leads to adequate information and therapy for affected patients.
Introduction
Charles Bonnet, a Swiss philosopher, biologist and natural scientist, reported in 1760 the case of his grandfather, who had visual hallucinations (VHs).1 The patient was 89 years old, mentally and physically fit, suffering from bilateral cataracts and had VH describing people, birds or houses. The patient was aware of the fact that these hallucinations were unreal.2–6
Georges des Morsier gave the name ‘Charles Bonnet syndrome’ (CBS) to VH, which occur in elderly, mentally fit patients.6 Much later, different authors suggested that VH in patients with CBS occur due to vision loss caused by ophthalmological diseases, such as age-related macular degeneration (AMD), other retinal diseases, cataract or glaucoma.4 5 7
Literature about CBS shows a large scale of diagnostic, inclusion and exclusion criteria. There is no commonly applied definition about CBS but most authors agree that patients have eye pathologies but no psychopathological disease (eg, dementia, psychosis or other neurological disease), have full insight that VH are unreal and VH are complex (eg, objects, faces, animals, plants or figures), repetitive and disappear when the eyes are closed, and there are no hallucinations affecting other sensory modalities.5–13
The current literature states that there are many different hypotheses about pathophysiology of CBS. VH may result from disorders in the visual cortex, visual perceptual disorders, overactivity in cortical areas or ageing.4 13 15 ,19
Patients fear being believed to be mentally ill, so they do not tell medical staff or even their relatives about their symptoms.21
Due to a lack of randomised controlled trials (RCTs), no evidence-based treatment for patients with CBS is available. It is presumed that VH would disappear with a better vision (eg, cataract surgery). Cox and Ffytche showed in 2014 that about one-third of patients with CBS are distressed from their VH.21 Better information and awareness and an informative medical consultation may have a significant impact treating patients with CBS.
This study is a RCT of patients with CBS, using concrete diagnostic criteria. The intention of the authors was to assess the potential beneficial effect of an additional psychiatric evaluation (compared with a consultation between patient and ophthalmologist) for patients suffering from CBS.
Patients and public involvement
Informed consent to participate in the trial was obtained from all patients prior to enrolment. Once this study is published, patients will be informed with an information sheet. Patients can choose if they wish to be informed about the study outcome or not, and how they want to receive the results (eg, by telephone or email).
Diagnostic and inclusion and exclusion criteria were defined using the current literature:
All patients participating in the trial had to have a visual acuity of 0.5 LogMAR7 or worse in the better eye and a minimum age of 55 years. To give clear guidance for our data, different tools (guided interview, quality-of-life scale, minimental-state examination) for diagnosing CBS were used.
Using the modified Telephone Interview for Cognitive State (TICS-m) it was ensured that patients with CBS:
Have no mental pathologies such as dementia, psychosis or any other neurological diseases.6 8–11
Have a normal cognitive state.8 10
Are not able to control the VH.8
Know that the VH are not real.5 7 10–12 22
Are usually older.9 10
Have significantly reduced visual acuity due to bilateral ocular pathology.9 10
Additionally there are no:
Auditory or olfactory hallucinations.5 7 8 11 22
Other abnormalities such as delusions.5 7 8 11 12 22
The North East Visual Hallucination Interview (NEVHI) gathered data regarding the description of VH associated with CBS:
Disappear when the eyes are closed.8
Are repetitive.8
Are complex (eg, objects, geometrical patterns, faces, shapes, figures, scenes, animals or plants).4 7 10–12 15 23 24
Furthermore, we excluded patients who were on dopamine agonist medication, patients with a temporal lobe epilepsy, a moderate to severe Alzheimer’s dementia, a present chronic alcohol/drug abuse or a bad cognitive state.
Patients with a visual acuity of 0.5 LogMAR or worse in both eyes were screened at the Department of Ophthalmology in Hanusch Hospital, Vienna asking them a standardised question: 22 25–28
‘Sometimes people who have an eye disease with bad vision see images or hallucinations that are actually not real or see things that other people do not see. This is a known condition called CBS. It happens to people who are of sound mind and have no mental or psychiatric illness. Have you ever experienced any VH?’
If patients responded in the affirmative, the patient was asked whether he/she would like to participate in the trial.
Patients were asked to describe and draw the VHs. Furthermore, their medical history was taken in detail. In order to check the exclusion criteria, standardised tests, such as the NEVHI,29 the Satisfaction with Life Scale (SWLS)30 and the TICS-m,31 were used to assess VH, the quality of life and possibly dementia.
All patients were allocated into two groups using randomisation by minimisation with the online randomisation tool ‘QMinim Online Minimisation’.
Variables for randomisation were: visual acuity: worse than 1.0 LogMAR or 0.50–1.0 LogMar, and if patients had significant problems due to the VH, or if the VH were not causing a reduction in quality of life.
The control group had a face-to-face interview with their ophthalmologist explaining the nature of CBS. Patients in the study group received a detailed clinical exploration, and if deemed useful, a medical therapy by a psychiatrist.
After 3 months of the first visit, patients were interviewed again with the NEVHI and the SWLS to assess, if there was a change concerning their CBS symptoms and in quality of life.
Results
4900 patients were screened, of which 390 patients with a visual acuity of less than 0.5 LogMAR in the better eye were found. Simple VHs such as floaters were reported in 18.5% (n=72). In total, 11.8% (n=46) had complex VHs such as seeing people or faces (n=14), geometrical patterns or figures (n=11), plants (n=5) and animals (n=4). Twelve patients with complex VHs were excluded due to following reasons: four patients had a reduced state of cognition (less than 33 points at the TICS-m), three patients had a visual acuity of better than 0.5 LogMAR (on testing for trial entry), two patients had a moderate to severe Alzheimer’s dementia, and one patient had temporal lobe epilepsy, medication with dopamine agonists or was not willing to participate. Therefore, the prevalence of the CBS patients with a visual acuity of less than 0.5 LogMAR at our department was 8.7% (n=34).
Table 1 shows demographic data of all included patients with CBS (n=34) compared with the entire population (n=390). Of the 34 patients with CBS, 28 were female and 6 were male, respectively. Mean age was 79.3 years with a range from 55 to 97 years and an SD of 9.7 years. Figure 1 shows examples of VHs drawn by different patients.
The demographic data of all patients with CBS (n=34) compared with the entire population (n=390)

Examples of visual hallucinations drawn by different patients.
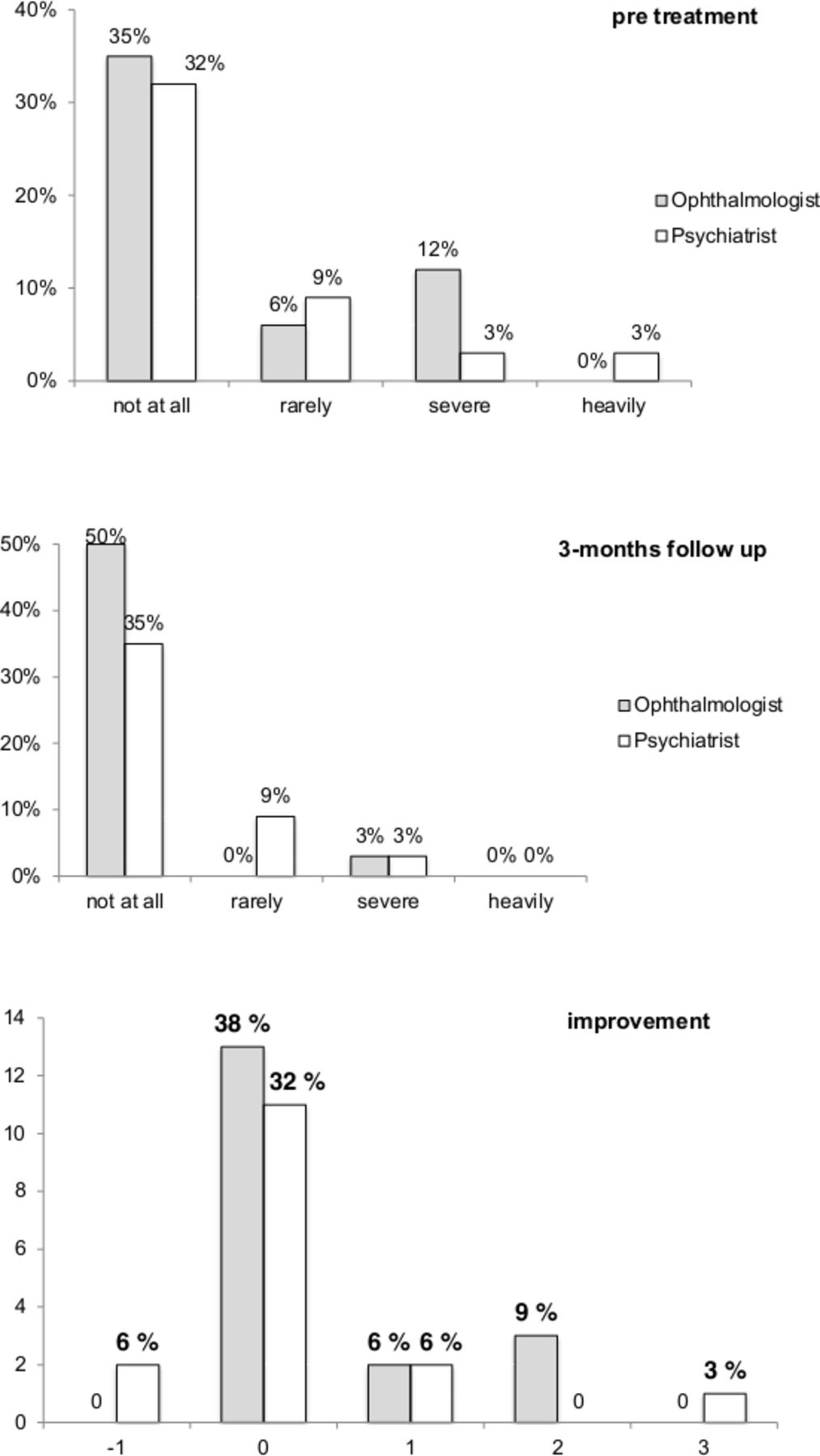
After randomisation by minimisation, 18 patients had a face-to-face consultation with an ophthalmologist (control group) and 16 patients received further exploration and possible medical treatment by a psychiatrist (study group). In six cases in the study group medication was offered to the patients: three declined, two received Sertraline and one patient received Trittico (both selective serotonin reuptake inhibitors).
Figure 2 shows the psychological strain before and after treatment. There was no statistically significant difference found between the control and the study group (p=0.727).

{kind=link}
{kind=link}
Psychological strain before and after treatment.
Discussion
CBS is defined by the occurrence of VH in the absence of any mental disorder. Elderly patients with reduced visual acuity due to ophthalmic disease are most affected. Conditions often associated with the syndrome are AMD, cataract and glaucoma. Existing data on the syndrome’s prevalence in Europe reveals diverse results.
The aim of this study was to evaluate, if additional treatment by a psychiatrist is beneficial and also to assess the prevalence of CBS in patients with low visual acuity.
Most of our patients with CBS were relieved to learn that they are not mentally ill and there is a known syndrome for their symptoms. However, to date, there is no approved medical treatment for patients suffering from CBS. Our attempt to compare a discussion with an ophthalmologist and a psychiatrist showed that almost all patients felt more worried about losing their eyesight because of their eye disease rather than about having VH.
The prevalence of the CBS at our department was relatively low in comparison to other studies. In Europe, Teunisse et al,7 Ffytche and Howard14/Cox and Ffytche21, Santhouse et al,20 Cohen et al,27 Lannon et al,32 Abbott et al23 or Jackson et al25 showed a higher prevalence of CBS. These differences could be due to rather vague diagnostic, inclusion and exclusion criteria. Therefore, it is not surprising that the estimated number of not reported cases of CBS is high. In this study, we excluded patients with psychiatric/neurological pathologies (eg, dementia or Parkinson’s disease) and we differentiated between simple and complex VHs. The prevalence of CBS would be much higher if these exact criteria had not been considered.
In the literature, different criteria for CBS are mentioned, but currently there are no standardised diagnostic criteria for CBS. Visual acuity as an influencing factor for development of CBS is often discussed. With regard to the study of Teunisse et al,7 we also chose the limit of visual acuity for patients to be screened at 0.5 LogMAR. Due to our results of patients with CBS compared with the entire population, we assume that patients with CBS may sometimes have better visual acuity, potentially 0.5–0.70 LogMAR. In a future trial it could be worth considering using different groups of visual acuity and a longer period of observation to find out if a loss of visual acuity causes VH or in reverse, an increase of visual acuity can stop VH, such as in cataract patients after surgery.
Additionally, we found that our demographic data, such as sex or age distribution, were similar to other studies.
Due to a lack of RCTs, there is no evidence-based treatment for patients with CBS who suffer from VH. In this study, clearly defined criteria for diagnosing a CBS were used and patients were randomised in two groups to find out whether a consultation with a psychiatrist is a potential benefit for patients with CBS.
With the limitation of small sample size in the study and control group, we show that competent advice and explanation to patients with CBS is essential. We were not able to show an added benefit from psychiatric evaluation.
Conclusion
Summing up, patients had a relevant benefit from learning about CBS and they were relieved that no mental illness is involved. Furthermore, prevalence of CBS strongly depends on the inclusion and exclusion criteria. Although the face-to-face consultation with an expert is of great importance, an additional psychiatric therapy showed no benefit for patients involved in our study group. However, in several cases the underlying cause of VH is not CBS and these patients may benefit from an interdisciplinary working with psychiatry and neurology. It is essential for people involved with patients suffering from severe vision loss to learn more about CBS. This will make it easier to identify and interpret symptoms correctly and might also lead to a more adequate information and therapy for affected patients. For further studies precise and standardised diagnostic criteria should be defined.
References
Footnotes
Contributors BD was responsible for the study conception and design, data acquisition, analysis, interpretation and writing of the manuscript. MK and LS were concerned with data acquisition and interpretation. NH and OF had substantial contribution in the study conception and design. All authors revised and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval All the research and measurements followed the tenets of declaration of Helsinki and the local ethics committee approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.