Article Text

Abstract
Background/Aims The classification of retinal detachment is currently still based on many objective criteria such as duration of symptoms and funduscopic macular status, which leaves some important questions unanswered. The most important factor is the macular status, which is determined using direct or indirect ophthalmoscopy. Optical coherence tomography (OCT) has become a standard tool in clinical practice and enables detecting the exact extent of subretinal fluid in macula-off/on retinal detachment. We introduce a new and simple OCT-based grading system for macular detachment to provide a basis for further investigations to determine the optimal timing for surgery.
Methods We retrospectively included 155 patients who were treated for retinal detachment. We defined the extent of the macular detachment in six stages based on the Early Treatment Diabetic Retinopathy Study (ETDRS) grid of the OCT scan.
The outermost ring of the ETDRS grid was defined as zone 1, the middle ring as zone 2 and the inner ring as zone 3. Only zone 3 differed in the retinal detachment height grades (grade a <250 µm vs grade b >250 µm). Retinal detachment heights that could not be measured were considered grade 4 (ungradable) detachments.
Results Forty-seven patients had no macular involvement (grade 0). Regarding macular detachment, 14 patients had grade 1, 20 had grade 2, 9 had grade 3a, 29 had grade 3b and 36 had grade 4.
Conclusion The newly developed OCT grading system for macular involvement following retinal detachment is a crucial tool to objectively classify a retinal detachment in order to be able to make better statements in the future, like for defining the optimal time for surgical intervention. A secondary benefit of this grading system would be that it improves predicting postoperative visual acuity.
- retina
- vitreous
- macula
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Until now, no OCT based objective grading system is available to classify a retinal detachment.
What are the new findings?
We introduce a new grading system for determining the influence and extent of macular detachment seen in preoperative optical coherence tomography (OCT) evaluation in relation to the postoperative visual outcome and timing of surgical intervention.
How might these results change the focus of research or clinical practice?
This new OCT grading system is standardised and could be a useful tool for all upcoming studies relating to retinal detachment.
Such uniform OCT grading system could harmonise all the studies for retinal detachment and make a comparison between these studies possible.
Introduction
Rhegmatogenous retinal detachment (RRD) is the most common vitreoretinal emergency and can lead to blindness if left untreated. Risk factors for retinal detachment are myopia, ocular trauma, cataracts and other ocular surgeries.1–3
Most surgeons have difficulty determining the optimal surgical timing that will yield the best visual results for patients with RRD.4 Preoperative status of the macular detachment is the most important prognostic indicator for visual recovery after surgical repair of RRD.
In cases of retinal detachment, macular involvement has been historically determined using direct or indirect funduscopy. However, optical coherence tomography (OCT) has recently become more important and is a standard tool in the clinical routine of most ophthalmologists.5 OCT-based classification of the macular involvement is ideal for preoperatively evaluating patients with retinal detachment and could help identify the optimal timing for surgical intervention. A standardised and accurate OCT classification of the macular involvement would also provide a basis for comparing retinal detachment studies.
Several studies investigating factors that affect visual outcomes have identified other preoperative findings such as visual acuity, age and comorbidities.6–8 Other investigations have identified the time between symptom onset and surgery as another important predictive factor.9
Macula-off detachment is commonly thought to have a worse visual prognosis than that of macula-on detachment.10 Specifically, macular detachment height and duration have been found to be major predictive factors for postsurgical visual outcomes.11
For retinal detachments with macular involvement, primary anatomical success may not yield good visual outcomes, and the functional results vary greatly.11 12 Accurately evaluating the preoperative macular involvement using OCT examinations enables better determining the optimal timing for surgical intervention. This means more precisely predicting patients’ visual recovery.
In the current study, we designed a new grading system that can be easily applied in everyday clinical practice to determine the influence and extent of the macular detachment seen in the preoperative OCT evaluation relative to the postoperative visual outcome and surgical intervention timing. Additionally, this consistent OCT classification enables comparing the results of retinal detachment studies.
Subjects and methods
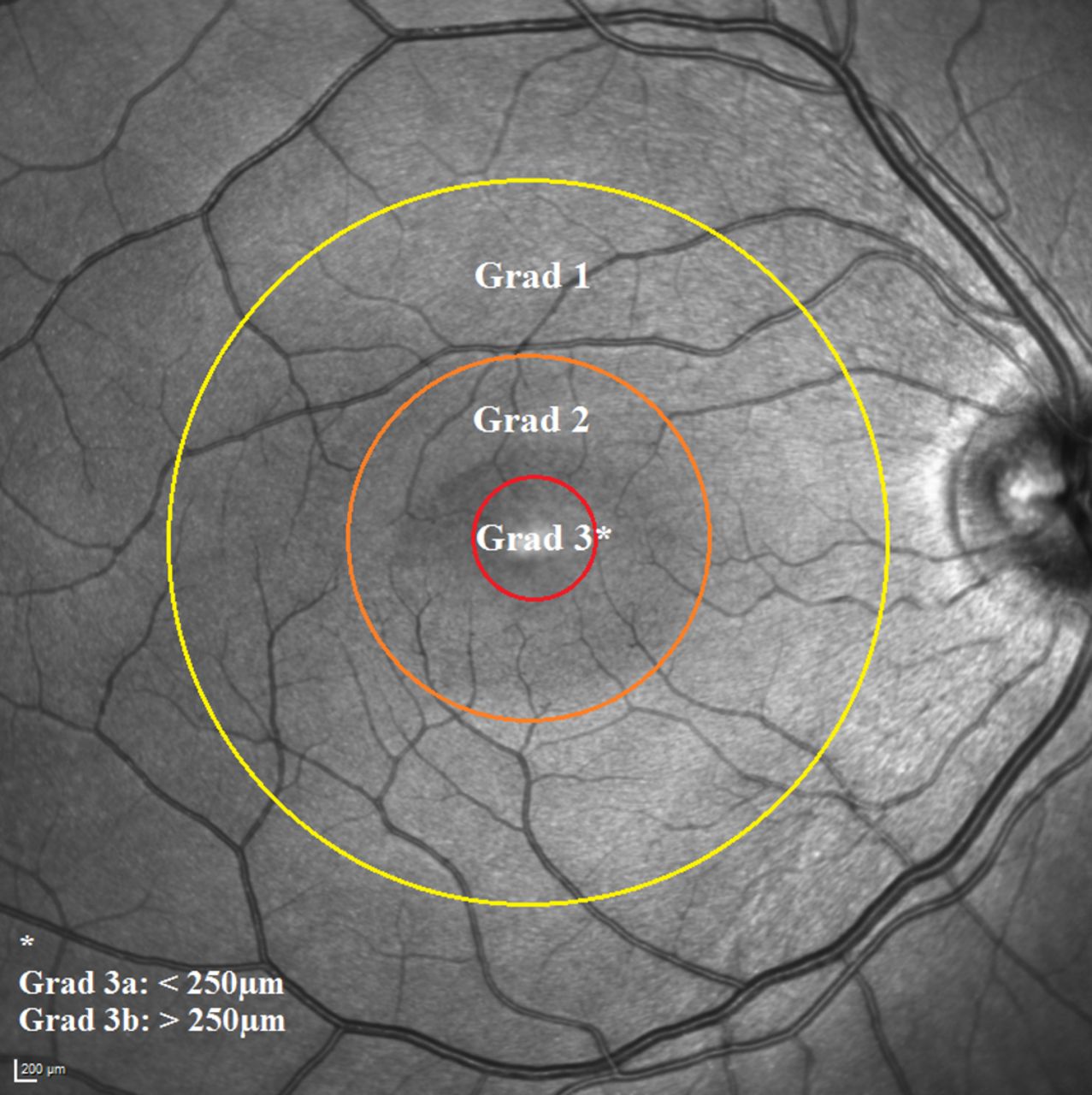
We included all patients with retinal detachment treated in the Eye Clinic, Sulzbach, Germany, between January 2015 and February 2017. Only patients with a primary retinal detachment were included in this analysis. All patients underwent a routine volume scan of the macular region with a spectral domain OCT (Heidelberg Engineering, Heidelberg, Germany). To evaluate the macular detachment, we introduced a new grading system based on the Early Treatment Diabetic Retinopathy Study (ETDRS) chart from the OCT evaluation (figure 1). The middle of the ETDRS chart was automatically centred on the fovea; if it was not centred on the fovea, we adjusted it manually.

Optical coherence tomography grading based on the Early Treatment Diabetic Retinopathy Study grid.
The Heidelberg Spectralis OCT has an integrated ETDRS grid in the results/analysis of every macular volume scan. We used this simple grid pattern to evaluate the macular involvement in cases of retinal detachment. We labelled the outer ring of the ETDRS grid as zone 1, the middle ring as zone 2 and the inner ring as zone 3. If the subretinal fluid was outside the ETDRS grid, we called this a grade 0 macular detachment (no macular involvement). Cases with subretinal fluid in one of these zones or significant retinal elevation were considered macula-off retinal detachments of grades 1, 2 or 3. In zone 3, we distinguished between low macular detachment (<250 µm=subcategory a) and high macular detachment (>250 µm=subcategory b).
The 250 µm were determined arbitrarily, as there is simply too little data in the literature on this subject. We think that this is very meaningful for such a sensitive device like OCT.
If the retinal detachment height was too elevated to be seen centrally on the OCT (>2000 µm), it was determined to be ungradable or a grade 4 detachment.
All retinal detachment cases in this study were treated via primary 23 g vitrectomy within 48 hours of admission. The vitrectomy was performed with a standard 23 g transconjunctival three-port vitrectomy (EVA, DORC, Zuidland, The Netherlands). In all cases, a full vitrectomy was performed after a vitreous detachment, and the vitreous base was extensively shaved under indentation. In all cases, we used Octaline to obtain a full retinal reattachment after a fluid-air exchange. The use of Octaline is a personal preference, as we personally believe it results in fewer retinal folds and metamorphopsia. All retinal breaks were treated with endolaser coagulation, and the surgery ended with a gas endotamponade. We had 61 pseudophakia eyes and 94 phakia eyes in our study. In 15 cases, we performed a combined phacovitrectomy. None of our patients had a cataract surgery within the first 3 months. We excluded all cases that underwent buckle surgery or silicon oil tamponade.
To evaluate the success of the surgery, we examined patients at 1 and 3 months postsurgery, to determine the best-corrected visual acuity (BCVA), the change in BCVA and the retinal status (attached, detached or proliferative vitreoretinopathy).
Statistical analysis
For the statistical analyses, we performed a Wilcoxon rank-sum test under the hypothesis that the BCVA would be better after surgery than before. P values <0.05 were considered to be statistically significant.
Patient involvement
Patients were not directly involved in the study, as the study was retrospective.
Results
This retrospective consecutive case series included all patients with a retinal detachment who had preoperatively undergone an OCT volume scan with a spectral domain OCT (n=155 patients). The mean patient age was 61.26±11.64 years. Most patients received a tamponade with SF6 (57.42%) or C2F6 (38.71%).
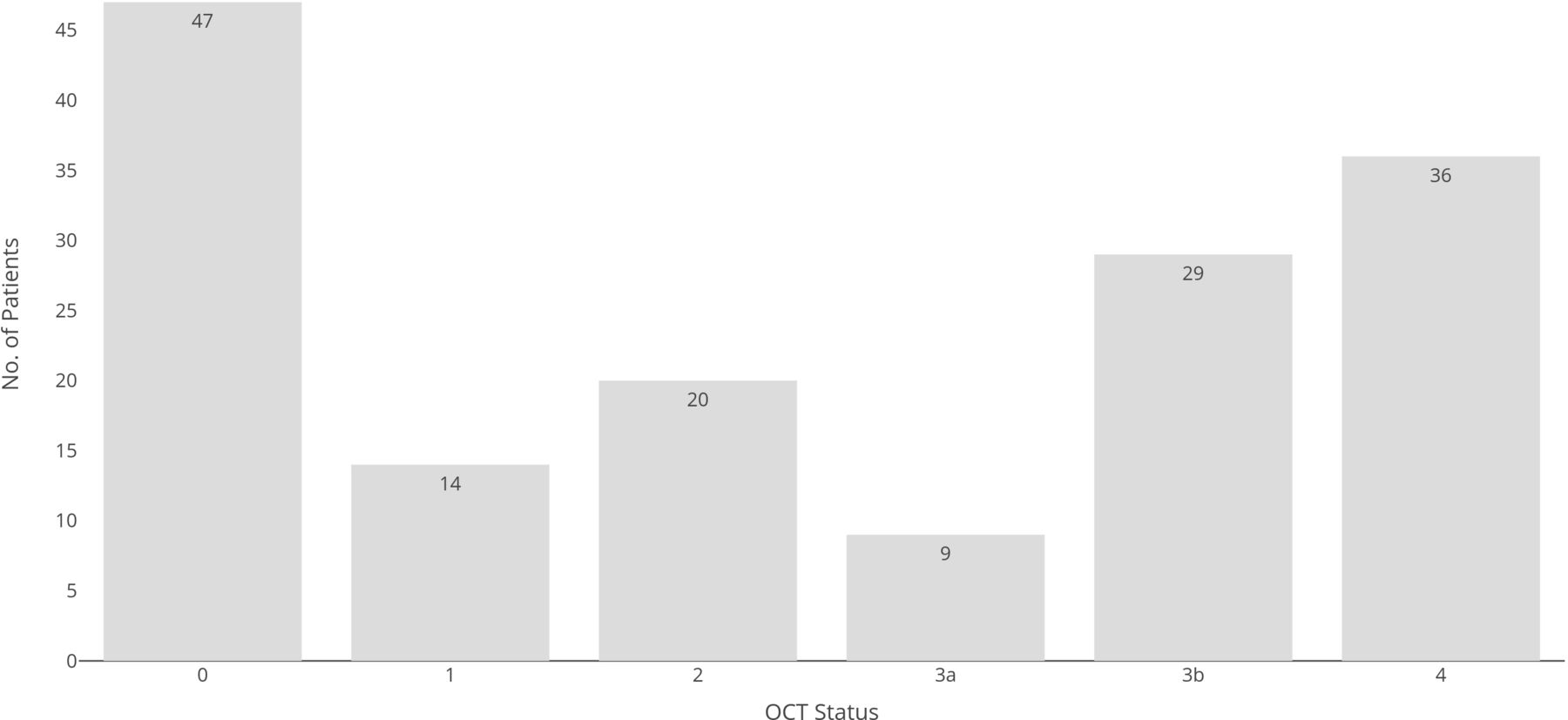
Forty-seven patients (30.3%) had no macular involvement (grade 0). Fourteen patients (9.0%) had grade 1 macular detachment, meaning that only the outer ring of the ETDRS grid was detached on the OCT volume scan. Twenty patients (12.9%) had grade 2 macular detachment. Nine patients (5.8%) had grade 3a and 29 patients (18.7%) had grade 3b macular detachment, meaning that the central 3 mm of the ETDRS grid was detached by >250 µm. In 36 patients (23.2%), the macular elevation was too high to accurately measure because of the height of the bullous detachment (grade 4=ungradable; figure 2).

Numbers of patients per optical coherence tomography (OCT) grade.
The preoperative mean BCVA decreased as the macular involvement grade increased. The BCVA values were 0.23±0.18 logMar (Snellen 20/34) for grade 0; 0.30±0.15 logMar (Snellen 20/40 for grade 1; 0.27±0.26 logMar (Snellen 20/37) for grade 2; 0.48±0.33 logMar (Snellen 20/43) for grade 3a; 0.78±0.36 logMar (Snellen 20/120.51) for grade 3b and 0.96±0.43 logMar (Snellen 20/182) for grade 4. The mean preoperative BCVA for all groups was 0.49±0.41 logMar (Snellen 20/62).
The mean postoperative BCVA per group after 1 month was 0.33±0.23 logMar (Snellen 20/43) for grade 0; 0.81±0.54 logMar (Snellen 20/130) for grade 1; 0.32±0.24 logMar (Snellen 20/42) for grade 2; 0.46±0.32 logMar (Snellen 20/58) for grade 3a, 0.54±0.37 logMar (Snellen 20/70) for grade 3b and 0.59±0.30 logMar (Snellen 20/78) for grade 4.
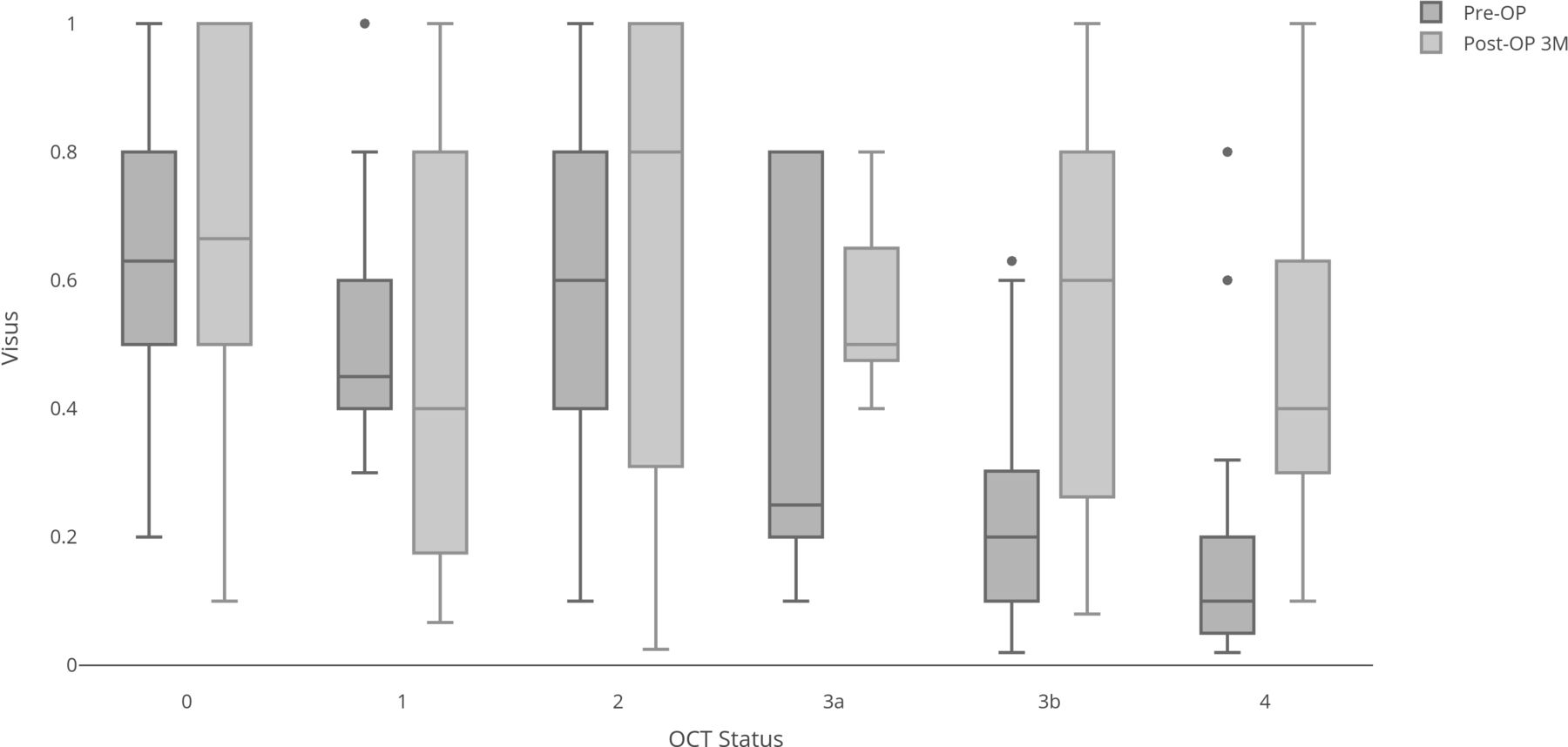
The postoperative mean BCVA per group after 3 months was 0.22±0.24 logMar (Snellen 20/33) for grade 0; 0.46±0.41 logMar (Snellen 20/58) for grade 1; 0.32±0.51 logMar (Snellen 20/42) for grade 2; 0.26±0.11 logMar (Snellen 20/36) for grade 3a; 0.33±0.31 logMar (Snellen 20/43) for grade 3b and 0.37±0.24 logMar (Snellen 20/47) for grade 4 (figure 3).

Visual outcome per group.
The preoperative and postoperative BCVAs differed nearly significantly for patients with a grade 3b macula-off retinal detachment (p=0.07), meaning that a high macular detachment of >250 µm with an initial visual acuity of 0.78±0.36 logMar (Snellen 20/121) showed the best surgical improvement to 0.54±0.37 logMar (Snellen 20/69), which is near reading-level BCVA. The improvement remained significant compared with that of the preoperative status after 3 months (p<0.01) and that of grade 4 after 3 months (p<0.01; figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Visual outcome after 3 months postsurgery. OCT, optical coherence tomography.
Discussion
The classification of retinal detachment is currently still based on many objective criteria such as duration of symptoms and funduscopic macular status. Patients often cannot remember the exact time of onset of symptoms and the process of retinal detachment varies greatly. Due to the large number of objective disturbing factors, a difficult comparability results and some questions remain unanswered. The optimal timing for surgical intervention with the best visual outcome in patients with retinal detachment still remains uncertain.9 10 12–15 This new grading system is the first OCT-based classification for preoperatively evaluating the macular region during retinal detachment. This new objective grading system is easy and fast to use and could be a new preoperative standard in clinical routines and studies.
OCT technology enables detecting a small amount of subretinal fluid that can potentially elude fundoscopic evaluation. This raises the question of ‘How off is off?’, and what amount and duration of subfoveal fluid or other preoperative signs are relevant to the postoperative visual outcomes and indicate the best time for surgical intervention.
Previous studies mainly considered only the symptom duration or the time until surgery and only differentiated between macula-on and macula-off detachments, while the extent or intensity of the subretinal fluid was not or was only slightly considered.16–18 Some publications described the preoperative and postoperative retinal changes in patients with macula-off retinal detachment, but no standardised classification exists for macula-on or macula-off detachments.19–21
Macula-off retinal detachment is commonly thought to lead to lower postoperative visual acuity and must be re-evaluated using this precise OCT classification. Our results showed that a small amount of subretinal fluid (grade 3a) can still result in good postoperative visual acuity. Even a centrally detached macula with a detachment of >250 µm and a bad initial BCVA can benefit significantly from surgery. Therefore, our results suggest that even a grade 3b macula-off detachment should undergo surgery as soon as possible.
In retinal detachment studies, the macular region is currently evaluated via funduscopic classification. Most older studies showed that delayed surgery led to significantly lower postoperative visual outcomes.12 22 23 Frings et al showed that surgery within the first 3 days postdetachment had better outcomes than did surgery between 10 and 30 days after symptoms appeared.5
Our data demonstrate that even patients with a distinctive detached macula (grades 3b and 4) have significant gains in visual acuity up to reading vision. This is because all retinal detachments undergo surgery within the first 24–48 hours after presentation, most within the first 12 hours. Our data also suggest that even macula-off retinal detachments should be treated as soon as possible, and timely interventions have positive psychological effects for the patient.
We found that a small amount of subretinal fluid (grade 3a) directly under the fovea did not strongly influence BCVA. Previously, only Matsui et al postulated a lower visual outcome for central macula detachments higher than 1000 µm in the OCT.16 Our data indicate that a 250 µm foveal detachment significantly affects the initial BCVA but can still lead to an improved BCVA if treated early. However, there is very little literature on the amount of subretinal fluid associated with retinal damage and therefore our work is very important as this factor is not considered in current studies. Furthermore, it should be noted that the macular detachment plays an important role, and the structural changes in the retina in the OCT already have an influence on the outcome.24
Interestingly, our work showed that patients with a grade 1 retinal detachment sometimes had a worse outcome than patients with higher grades. The fact that all patients were operated within 48 hours may explain these unexpected results. Therefore, we believe that future multicentre studies will play an important role in better interpreting the results.
Certainly, it would be important in the future to include an even larger number of patients in order to have a more balanced group distribution of the different stages, which would allow a better significance. A further limitation of our study is certainly the short follow-up period and the fact that we did not include patients who did not receive OCT preoperatively, in order to better demonstrate the strengths of the OCT grading versus the classic observer. We are aware of the fact that the duration of symptoms is seen in other studies as a predictive factor for the outcome. However, the duration of symptoms is often very subjective and therefore we believe that an objective grading system at the initial presentation of the patient is useful.
Retinal surgeons need a more precise method for determining the best time for surgery. Knowing the exact extent of the subretinal fluid and time for the surgical intervention is crucial. One crucial factor in all these studies is that all patients with a fulminant progress of the retinal detachment had earlier consultations with an ophthalmologist than did patients with slow and shallow subretinal detachment, which may deeply affect visual outcome results.
This new uniform OCT grading system is standardised and could be useful for upcoming studies on retinal detachment to enable making between-study comparisons.
References
Footnotes
Contributors KB, KJ, PS and PW made substantial contributions to the study conception and design. PW, MA, AK, SZ, A-MS and SL made substantial contributions to acquiring, analysing and interpreting the data. All authors have been involved in drafting the manuscript or revising it critically for important intellectual content and have approved the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The local ethics committee approved this retrospective consecutive case study, which was performed in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.