Article Text

Statistics from Altmetric.com
In 1999 the World Health Organization and the International Agency for Prevention of Blindness announced a joint programme to eliminate unnecessary blindness. The programme is called “Vision 2020—the right to sight”.1 Key to this initiative is the provision of sufficient, successful, and sustainable cataract services for all communities. The questions that therefore arise include: what is a sufficient; what is a successful; and what is a sustainable cataract service?2 Two articles in this issue of the BJO from Korea3 and Nepal4 evaluate cataract services using a variety of performance indicators—cataract surgical coverage, barriers to access, and outcome of surgery.
How many cataracts need to be operated?
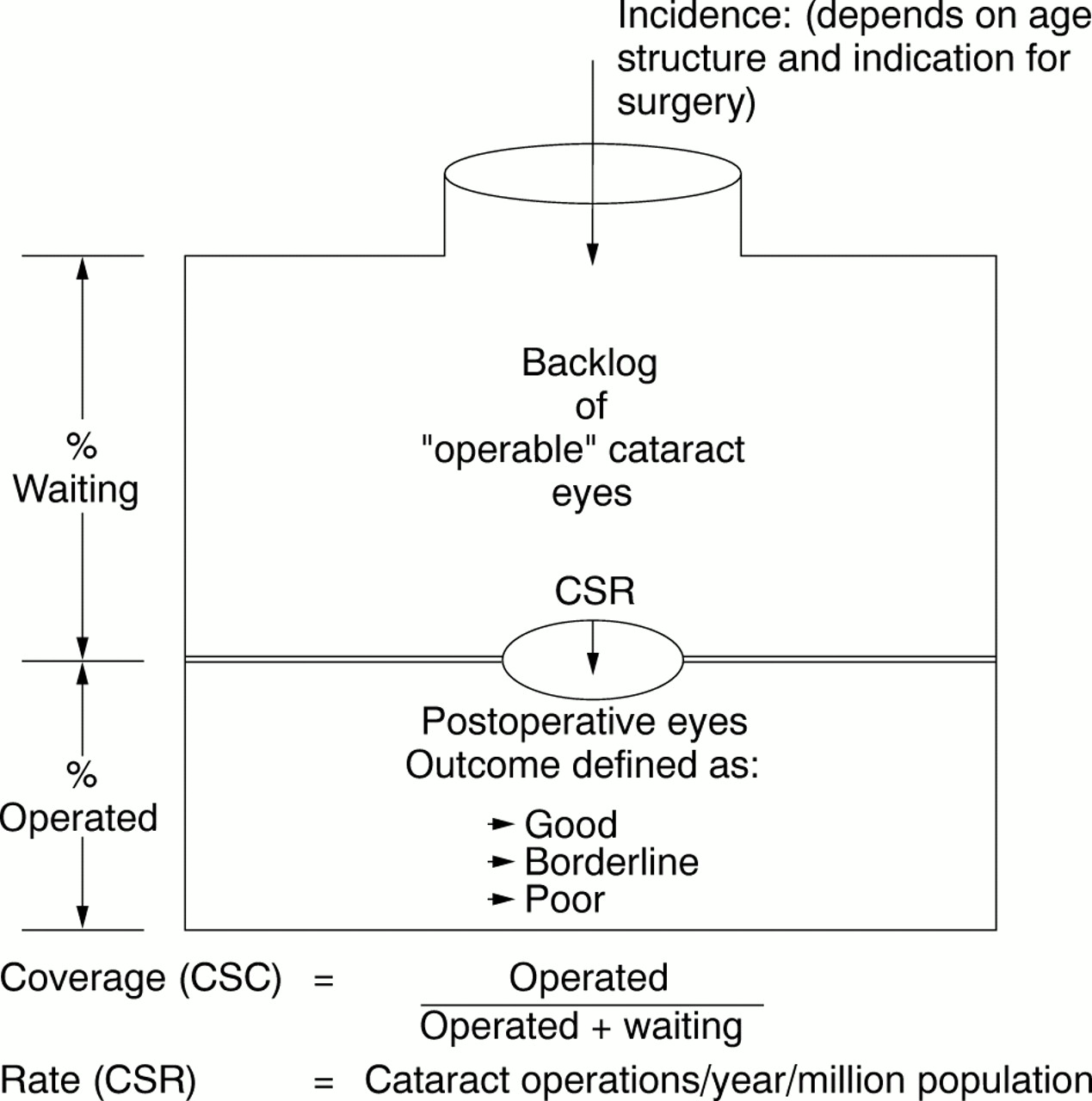
The aim of a cataract service is to operate on sufficient cataracts each year (cataract surgical rate; CSR), so that everyone with “operable” cataract (visual loss justifying surgery) can receive surgery if they wish (100% coverage). The cataract surgical coverage is defined as the proportion of patients (or eyes) with “operable” cataract, who have already received surgery. As reported in the paper from Korea, coverage varies according to the level of visual acuity used to indicate surgery, being 78% in people less than 6/60 and 55% for less than 6/18. Coverage surveys from other parts of the world have reported: Malawi <15%,5 Paraguay 36%,6 and Karnataka State, India 40%7 for bilateral <6/60 due to cataract. There is as far as I am aware no report from industrialised countries.
The CSR is the number of operations performed in a year for a given population (usually expressed as ops/year/million population) Rates vary from 6300 in Australia8 to 100 in Nigeria.9 Figure 1 schematically shows statistics used to evaluate and audit cataract services.

{kind=link}
Analysis for cataract services per million population.
The World Health Report10 estimates that approximately 20 million people are bilaterally blind (less than 3/60 in the better eye) from age related cataract. However, there are at least 100 million eyes with cataract causing a visual acuity less 6/60 and this number is increasing due to population growth and increasing life expectancy.2 The incidence of cataract blindness is unknown, but Minassian estimated that for India alone 3.8 million people become blind from cataract each year,11 and globally at least 25 million eyes become <6/60 due to cataract each year.
To reduce the backlog (or waiting list), the number of cataract operations performed each year must at least equal the incidence of operable cataract, where the definition of “operable” will vary depending on the level of acuity at which cataract surgery is routinely performed. Most ophthalmologists in developing countries agree that cataract extraction with an intraocular lens is indicated in any eye with a visual acuity less than 6/60, and in industrialised countries the indication for surgery is often around 6/12 to 6/24. The lower the indication for surgery the higher the CSR required to achieve a good coverage. Taylor8 has estimated that the CSR has to increase 2.5 times as one moves the indication for surgery from <6/60 to <6/24, and five times if it goes to <6/12.
At present an estimated 10 million cataract operations are being performed each year in the world. The author's estimates for the cataract surgical rate in various regions of the world are given in Table 1. North America is 5500 and Western Europe averages around 4000. In the middle income communities of Latin America and parts of Asia the rate is between 500 and 2000, and in most of Africa, China, and the poorer countries of Asia the rate is often less than 500.
Cataract surgery statistics estimates for 1999
There are various reasons for low cataract surgical rates, some due to low patient demand (characterised by low CSR with no waiting lists) and some due to inadequate service delivery (characterised by long waiting lists). Minassian12 has reported a backlog of 2.4 million people in England and Wales with <6/12 vision bilaterally due to cataract. Further analysis would suggest that the current CSR (estimated at 3800) needs to increase by 50% to keep pace with the incident cases of <6/12 bilateral cataract.
What are the results?
In order to measure the results of cataract surgery it is necessary to define outcome. Patient satisfaction and quality of life measurements have been used; however, they are time consuming and not suitable for ongoing monitoring of results by the cataract surgeon. The WHO Prevention of Blindness Programme defines outcome in terms of visual acuity, which can be assessed with full spectacle correction (“best vision”), or with available correction (“functioning vision”). Good outcome is defined as 6/6–6/18, borderline outcome as <6/18–6/60, and poor outcome as <6/60.13 These broad categories can be further subdivided—for example, 6/6 excellent, 6/9 very good, etc. This definition is simple and easy to use. The purpose is to encourage surgeons to monitor their own results—self audit over time, not comparison between surgeons or institutions. The period from surgery when acuity is measured will obviously affect the results, and this should therefore be standardised for an individual situation so that trends over time can be reviewed.
Studies from developing countries into outcome can be divided into clinical trials/selected series, routine hospital based data, and long term population based studies. The results from clinical trials and individual series are usually very good with poor outcome being found in less than 5% of cases.14 ,15 However, routine hospital based reports and long term population based studies have shown that the results are not as good as expected. Poor outcome (<6/60) is often found in more than 10% of eyes with IOLs and many more if an IOL has not been used.8 ,16 The findings for “poor outcome” in the two papers in this issue are summarised in Table2.
Summary of poor outcome of cataract surgery from two studies in this issue
In order to improve results we need to know the causes for “poor outcome.” These can be classified as:
those due to pre-existing eye disease
those due to surgical or early postoperative complications
those due to uncorrected refractive error
those due to long term surgical sequelae.
The two papers in this issue demonstrate the advantage of surgery with an IOL, and the need for care in correcting refractive error after surgery. The Nepal study identifies poor surgical technique in “eye camp” patients.
Naturally poor acuity experienced by patients following surgery will affect the demand for cataract surgery by the community. There seems little doubt that the poor results due to lost aphakic spectacles, and surgery by inexperienced personnel under inadequate conditions are still having a negative impact on people's perceptions of cataract surgery. Hopefully, competently performed IOL surgery in good facilities will begin to demonstrate that cataract surgery can be a very effective procedure with a high success rate in developing countries.
How can cataract services be made sustainable?
To eliminate unnecessary blindness from cataract we need ongoing services which year by year will deal with the new cases. Therefore Vision 2020 is about “sustainable services” rather than one-off campaigns targeting “backlog.” Sustainability implies the ongoing availability of adequate resources—people and funding.
Throughout the world eye care and, particularly, the cost of managing cataract is becoming a major part of health costs. Someone has to pay—governments, health insurance companies, the patient, or a donor. The cost of a cataract procedure is made up of various components including the cost of consumables, salaries, overheads, and a proportion of the depreciation cost of the infrastructure, instruments, and equipment. There are also significant indirect costs incurred by the patient for transport, time lost from work, food, etc.
In an effort to achieve sustainability the cost of cataract surgery should be kept as low as possible without jeopardising the outcome of surgery. Ophthalmologists, managers, and the ophthalmic industries are all important in determining what a cataract costs society and the individual. At the moment “Western” cataract surgery is too expensive for most of the world, and probably also for Western countries. Worldwide, 10 million cataract operations are done each year, but there is a need to do at least 30 million per year for the indefinite future. Economy of scale should bring lower costs. A first step is to minimise the cost of consumables through bulk purchase of “value for money” sutures, IOLs, and medicines. The second step is to increase productivity so that the relative cost of salaries and overheads per cataract procedure is reduced. Through efficient use of only essential consumables and good productivity the cost in developing countries can on average be kept to less than £50 per operation. However, this cost is still too high for many patients and therefore some form of subsidy may be required. Various cost recovery systems have been developed to generate income from paying patients (India), sale of spectacles (Africa), and other less essential eye services (Latin America). The aim is to make programmes self reliant for the running costs of a cataract surgical service, and use external (donor) support for training, new equipment, and other development costs.
A critical question to be addressed by Vision 2020 in Africa is the issue of “sustainable human resources.” At present there are insufficient eye surgeons and support staff, a paucity of good training programmes, and inadequate remuneration and motivation for nationals who want to work in their own countries of Africa. Innovative thinking stressing “north-south-north” and “south-south” partnerships rather than “one way north-south” projects is required by donor organisations and Western eye care professionals into how African eye care staff and training programmes can be supported. For example, India in many ways is far better placed to assist Africa in terms of appropriately trained personnel and training programmes than is Europe or North America.
Conclusion
Unless an affordable, easily usable prevention becomes available the only method to reduce cataract blindness is surgery. For Vision 2020 to become a reality it will be necessary:
to perform worldwide more than 30 million cataract operations every year (varying from 2000 to 6000 cataract operations per million population)
to improve the results of surgery (<6/60 rate of <5%), through ongoing monitoring and remedial action to deal with avoidable causes
to encourage professional groups and ophthalmic industry to make cataract surgery affordable for all sectors of society.
The challenge of “Vision 2020—the right to sight” is daunting, but doesn't vision sometimes require making ideas a reality? Vision 2020 will be achieved if people involved in eye care catch the “vision” for themselves and decide to make it a reality for the people they serve.