Article Text

Abstract
Objectives: To investigate the appropriateness of patients attending an Accident & Emergency (A&E) department of an eye hospital, identify reasons for inappropriate use and propose recommendations in improving the provision of ophthalmic A&E care.
Methods: A prospective questionnaire-based survey of consecutive patients who presented to the A&E department over a 7-day period was conducted. Patient demographic data, reason for attending from the patients’ perspective, diagnosis, duration of symptom and management outcome were recorded. The diagnoses were grouped into acute and non-acute, and into those which were considered suitable to be seen in a primary care setting by specialist trained community general practitioners (GPs) or optometrists.
Results: 560 completed questionnaires were evaluated; 171 cases (30.6%) were considered as non-acute and 210 (37.5%) were considered suitable to be seen by specialist trained community GPs or optometrists. 352 patients (62.8%) had symptoms for 1–6 days, 144 (25.7%) had symptoms for 1–4 weeks and 64 (11.5%) had symptoms for >1 month before presentation; in the latter two groups, 52 of the 208 patients (25%) were diagnosed with non-acute conditions. “Great concern” was the most common reason for attending the casualty department. 350 patients (62.5%) were discharged on the day of presentation.
Conclusions: A significant number of patients who attend ophthalmic A&E departments have non-urgent conditions that could be managed satisfactorily in a primary care setting by specialist trained GPs or optometrists outside the hospital casualty department. Improvement in education of patients, the provision of specialist ophthalmic training for GPs and optometrists, and expansion of outpatient services are needed so that casualty remains a genuine emergency service.
Statistics from Altmetric.com
In the UK, emergency eye care for ophthalmic complaints is provided both by general accident and emergency (A&E) departments and by dedicated eye casualty departments. There are differences in the way they operate, which is determined by the needs of the local community, size of the population and the resources available to the local primary care trusts (PCTs). Some eye units—especially dedicated eye casualty departments—can offer direct access through a walk-in service. Not all ophthalmic complaints that present to A&E can be considered as real emergencies. Although previous studies have shown that ophthalmic casualty departments provide a service that exceeds its defined functions, with 50–70% patients attending classified as non-urgent, little is known about why these patients attend.1–4 By contrast, studies which have looked at inappropriate use of general A&E departments have cited anxiety, depression, convenience and accessibility as reasons for opting to attend A&E rather than their general practitioners (GPs).5 6 To reduce the burden on ophthalmic casualty departments, it has been suggested that specialist trained GPs and optometrists should see these patients in the primary care setting and ophthalmic nurse practitioners (ONPs) should take on an extended role in the secondary setting.1 7
The aims of this study were: (1) to investigate the numbers of patients with ophthalmic complaints presenting to the casualty department of a dedicated eye hospital; (2) to examine the reason for attending from the patients’ perspective; and (3) to make recommendations on improving the service.
METHODS
This prospective exploratory study comprised a questionnaire-based survey of consecutive patients who attended the A&E department at Moorfields Eye Hospital over a 7-day period in May 2005. Moorfields is a specialist eye hospital which receives referrals from local PCTs in the London region and nationally from district general hospitals or other eye hospitals, both in the UK and from abroad. The A&E department operates a dedicated 24 h walk-in service and on average sees >60 000 patients per year. The survey was conducted between 08.00 and 19.00 h to reflect the busiest time of the casualty department, which would allow us to determine the most likely reasons for patients attending and to develop ways of improving the delivery of A&E services where it is most needed. The inclusion criteria included all the patients who attended A&E over the designated time period each day.
Study design
Patients were initially triaged and those with conditions that were suitable to be managed by an ONP as set out by Moorfields A&E policy—for example, superficial corneal foreign bodies—were treated and discharged. Patients with conditions not suitable for the ONP were triaged into urgent and non-urgent cases and allocated into separate trays before being seen by the casualty ophthalmologist. Examples of urgent cases included chemical injury and acute angle closure glaucoma; non-urgent cases included blepharitis and posterior vitreous detachment (PVD). Priority was given to those with urgent ophthalmic complaints to be seen first.
After triage, patients were given an anonymous questionnaire to fill out in the waiting room and were instructed to complete the form fully. They were given the opportunity to ask the ONP or clinic clerk questions relating to the questionnaire while waiting to be seen by the doctor. The following data were collected from the completed questionnaires: patient demographic characteristics, duration of symptoms, reason for attending from the patients’ perspective, diagnosis, source of referral and management outcome. To analyse the urgency of patients attending casualty, they were asked to indicate on the form whether they had had their symptoms for 1–6 days, 1–4 weeks or >1 month. After being assessed and treated by the casualty ophthalmologist, patients were either discharged, a follow-up appointment in A&E was arranged or they were referred to another subspecialty service.
To decide on the appropriateness of each attendance, the diagnoses were subdivided into acute and non-acute by the authors: acute conditions were those considered appropriate to be seen in the casualty setting whereas non-acute conditions were considered more appropriate to be seen in a primary care or routine outpatient setting. This classification was done separately after the questionnaires had been completed by the patients. Irrespective of the diagnosis classification, they were also grouped into those conditions that were suitable to be seen by specialist trained GPs or optometrists.
Analysis of data
Descriptive statistics were used to analyse the outcome variables. We sought to analyse the association between patients’ symptoms and their ocular diagnoses, and also to propose recommendations in improving the delivery of the A&E service.
RESULTS
Patient demographic characteristics
A total of 833 patients attended over the study period; 560 (67.2%) completed the questionnaires fully so were included in the analysis and 273 (32.8%) were excluded because of incomplete data entry or because they did not want to participate. Two hundred and ninety-seven patients (53.1%) were attending casualty for the first time while 263 (46.9%) had attended previously; we did not collect data on the reasons for patients re-attending. The peak time of arrival was between 10.00 and 11.00 h, which constituted 16.5% of the total number of patients per study day. The demographic characteristics of the patients are shown in table 1.
Reasons for attending
The list of ocular conditions encountered is shown in table 2; 171 cases (30.6%) were considered to be non-acute.
Three hundred and fifty-two patients (62.8%) had had symptoms for 1–6 days, 144 (25.7%) for 1–4 weeks and 64 (11.5%) for >1 month before presentation; in the latter two groups, 52 of the 208 patients (25%) were diagnosed with non-acute conditions.
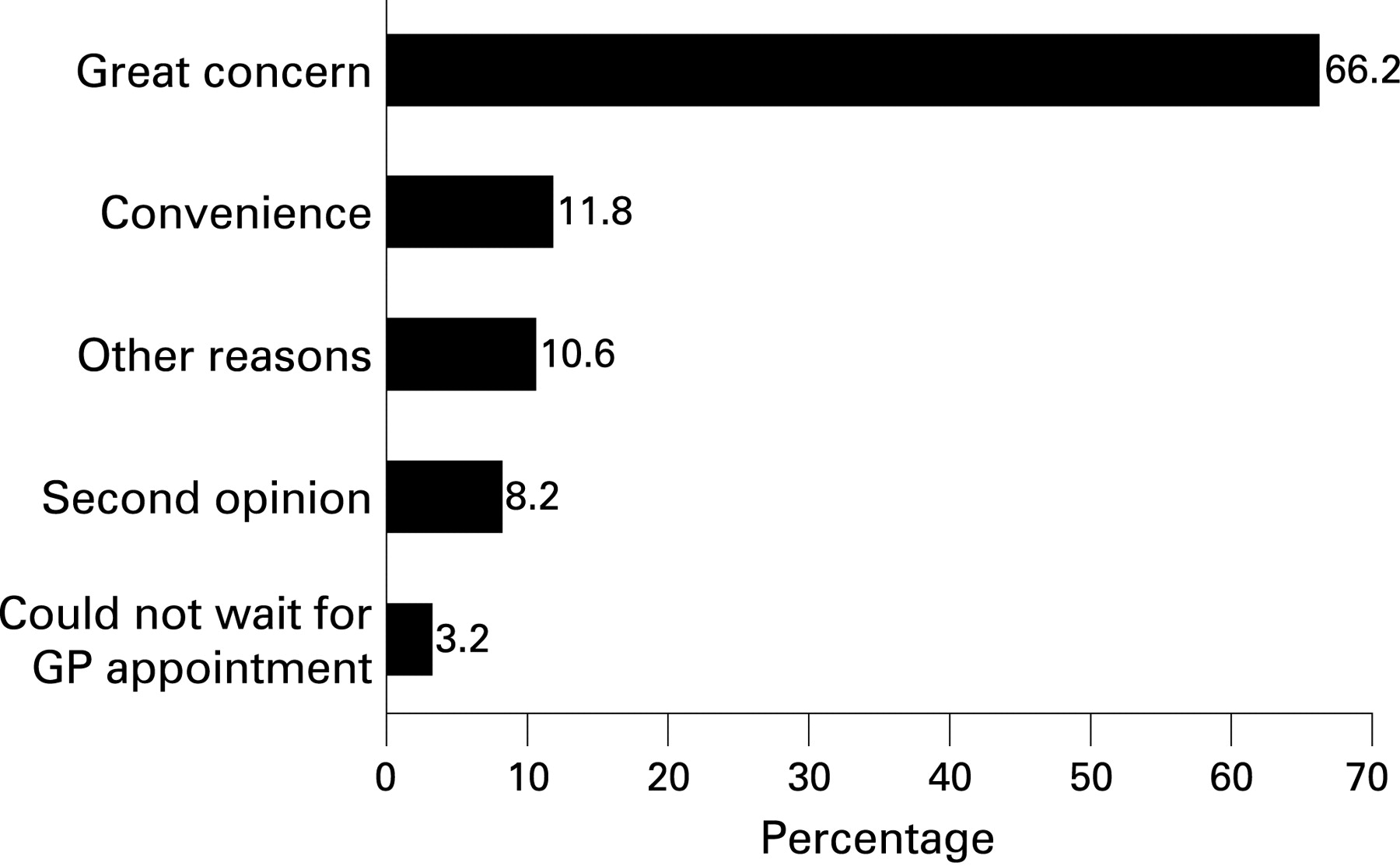
The reasons for patients attending the A&E department are shown in fig 1. A total of 210 cases (37.5%) were considered suitable to be seen by specialist trained GPs or optometrists (table 2), 160 (28.6%) with non-acute diagnoses and 50 (8.9%) with acute diagnoses of conjunctivitis. In this study, PVD was considered not suitable to be seen by primary care practitioners.
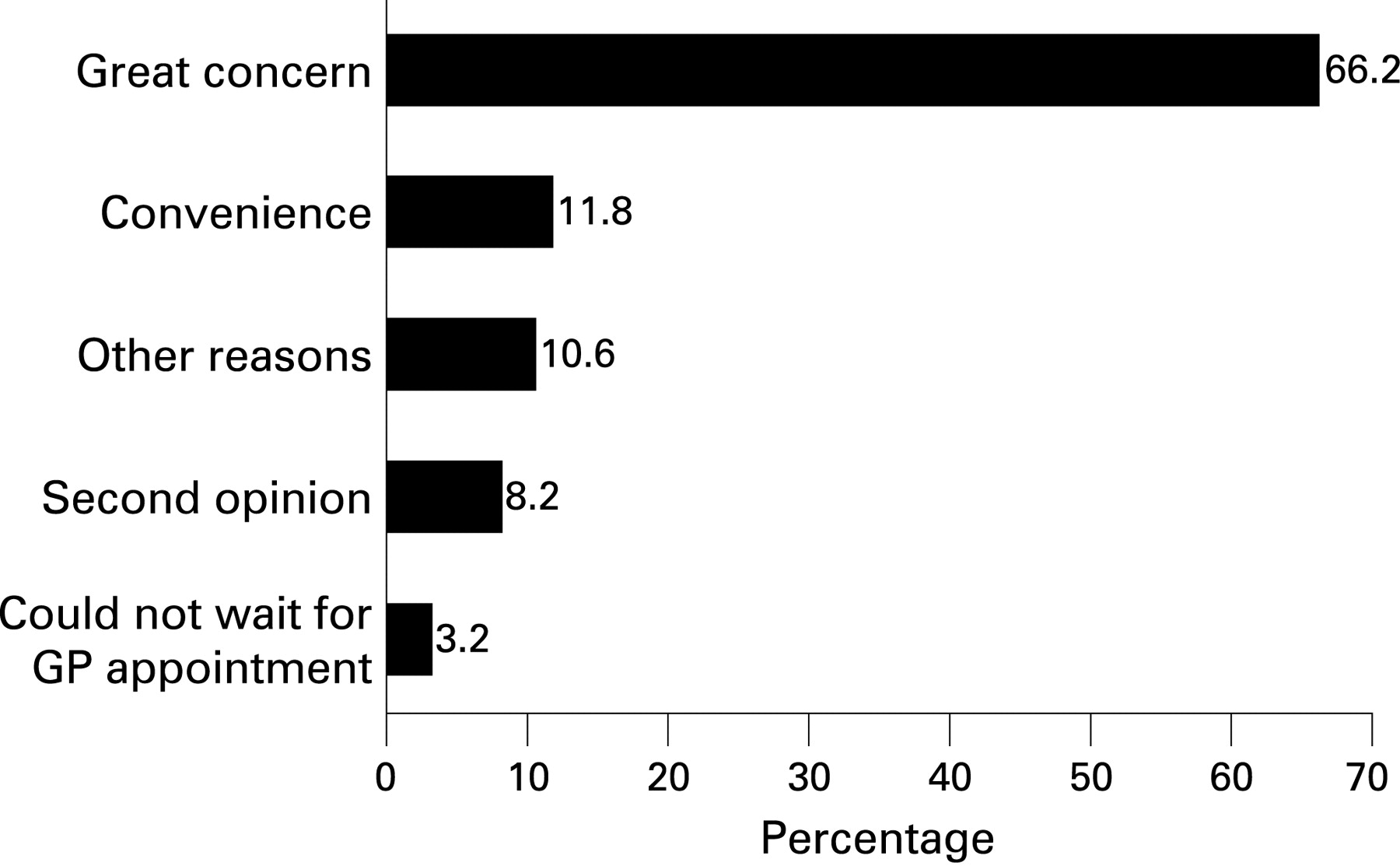
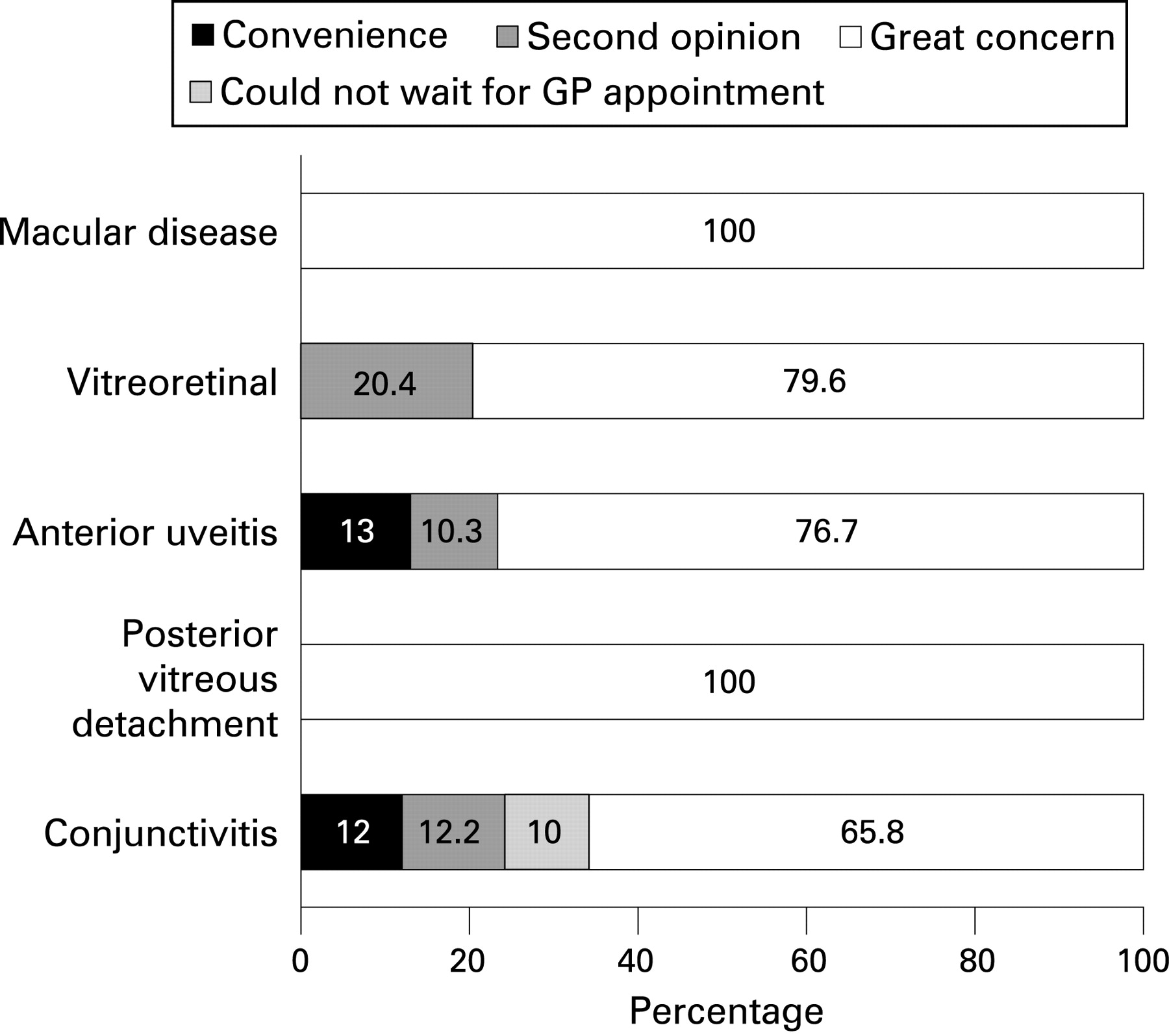
The reasons for attending for some of the common conditions encountered in casualty in both diagnostic groups are shown in figs 2 and 3, respectively. Although “great concern” was the most common reason, “convenience” and “unable to wait for a GP appointment” were more common in non-acute than acute conditions. Furthermore, there were 127 (74.2%) “greatly concerned” patients with non-acute conditions who had had symptoms for weeks or even months before attending. In total, 350 patients (62.5%) were discharged on the day of presentation with no further follow-up, 40 (7.2%) had an A&E follow-up appointment, 60 (10.8%) were referred to the primary care clinic and 109 (19.5%) were referred to other subspecialty clinics in the hospital.


{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The results of this study show that over 30% of patients who attend a dedicated ophthalmic A&E department consist of non-acute cases, which is in agreement with other published studies.1–3 Despite the desire to encourage patients with “non-urgent” complaints to be seen at a primary care level, the high percentage of inappropriate use is reflected by a multitude of different patient-related factors found in this study. The “great concern” expressed by patients as the main reason for attending was due to stress and anxiety created by the fear of visual loss and blindness, or the disfiguring nature of certain eye conditions such as conjunctivitis and uveitis. This explains why self-referrals formed the largest group of attendance, with GPs and community optometrists and referrals from other hospitals contributing smaller proportions.
A large number of patients had attended the A&E department previously; it was unclear from this study whether some patients re-attended because of previous advice by A&E—for example, those who had been diagnosed with anterior uveitis had new symptoms or those who were already a patient at Moorfields were told to return to A&E if they had new symptoms. In addition, some patients with a non-acute condition such as blepharitis might not have had their condition fully explained to them initially to allow them to self-manage when their symptoms worsened. Other factors such as increasing age, living locally and psychiatric comorbidity have all been reported as potential reasons for frequent attenders.8 9
Eye disease can produce anxiety levels similar to those seen in patients with systemic conditions such as melanoma, acquired immunodeficiency syndrome and bone marrow transplantation.10 This perception was found to apply to both acute and non-acute conditions because it is difficult for patients themselves to identify which conditions are serious by their signs and symptoms and therefore the need to seek specialist advice urgently rather than seeing their GP or optometrist.10 11 This could explain why over 50% of patients with chalazion, dry eyes and blepharitis expressed great concern when they presented to the casualty department (fig 3). Despite this, a large number of patients with non-acute conditions had symptoms for weeks to months before presenting, indicating that the degree of concern was less than in those with acute conditions.
“Convenience” and “could not wait for GP appointment” were more common with non-acute disorders. Possible reasons were the convenience of the 24 h walk-in A&E service that Moorfields operates or that patients wanted to bypass the waiting time for an outpatient appointment when their condition needed referral. Ten percent of patients with conjunctivitis reported that they could not wait for a GP appointment as a reason for attending, which suggests that they probably knew their condition was not sight-threatening. However, 12.2% of patients sought a second opinion because their conjunctivitis had probably failed to improve after seeing their GP or optometrist. Thirteen percent of patients with anterior uveitis attended because of “convenience”; some patients may have attended Moorfields in the past or they were existing Moorfields patients who had run out of medication and needed a repeat prescription. This suggests that some patients do not view ophthalmic casualty as a place for emergencies only but also for obtaining prompt treatment and second opinions for non-sight threatening complaints because of convenience and accessibility. These findings are comparable to those studies published on inappropriate attenders to general A&E departments, which could account for 20–80% of total visits.6 Proper patient education could be an important factor in reducing the number of non-acute cases attending A&E, and it would also help to empower patients in making appropriate decisions with self-management when their symptoms deteriorate.
More than 8% of patients came for a second opinion, and it was interesting to note that this applied to non-acute conditions such as dry eyes and blepharitis as well as acute conditions. Patients with anterior uveitis and conjunctivitis wanted a second opinion because their condition had not improved with treatment given by their GP or optometrist. Patients with vitreoretinal problems such as retinal detachment were referred to Moorfields because of the lack of a vitreoretinal subspecialty in some hospitals.
To reduce the high percentage of inappropriate attenders to A&E, changes might be required in the way ophthalmic care is delivered in the UK. Utilisation of existing resources and enhancing the role of allied ophthalmic professionals would assist in achieving this goal. The use of ONPs in hospitals has been invaluable in reducing the workload of ophthalmic A&E departments.1 12 13 Indeed, it has been suggested that emergency nurse practitioners may be better at assessing ophthalmic emergency conditions than junior doctors in general A&E departments.14 Many ophthalmic units employ a triaging system to prioritise cases on arrival to reduce waiting time and ensure emergency conditions are seen first. It might be possible to inform patients at triage that their complaint is non-urgent and that they should see their GP or optometrist first before attending casualty; this will result in a reduction in waiting times and an increase in efficiency. However, this could only happen if GPs are properly trained to deal with eye complaints, as it has been shown that over 50% of GP referrals to the ophthalmic A&E department do not constitute true emergencies.2
Hospital optometrists have been found to be competent in working in an A&E setting15 and, in addition, the Department of Health in the UK has recently granted suitably trained optometrists the rights to extend their therapeutic prescribing powers in the form of Additional Supply, Supplementary and, more recently, Independent prescribing.16 To gain these qualifications, further specialist training in the form of practice-based learning in an ophthalmic A&E department is required, and this will allow optometrists—both hospital and community—to have an extended formulary of topical agents to manage non-sight threatening conditions such as dry eyes and superficial eye injuries. The experience acquired in an A&E environment is important because it allows full exposure to different ocular conditions so that only cases that need to be seen in casualty are referred. Studies such as the Camden and Islington Anterior Eye Diseases Scheme, which used accredited optometrists to assess patients, found that 23% of patients were discharged without treatment and only 4% of patients needed referral to the hospital.17 In our study nearly 40% of cases were considered suitable to be seen by GPs or community optometrists if they were appropriately trained. For optometrists to take on this extended role they should be encouraged to gain Additional Supply status. Furthermore, over 60% of patients in our study received treatment and were discharged on the same day, which means conditions such as PVD—though not considered suitable to be seen in a primary care setting in this study—could have been seen by community optometrists.
Additional funding from the NHS will need to be in place to allow optometrists and GPs to gain additional training, and also to recruit ophthalmologists to teach and train allied professionals. The formation of a list of nationwide specialist trained GPs and optometrists would help in allowing colleagues to identify which practitioners are accredited to see patients with ophthalmic problems. Patients will also need to be educated and encouraged to see their local accredited practitioner initially for any ocular complaint and feel confident that referral to hospital will only be made if needed.
Improvements can also be made within the Hospital Eye Service: one option involves seeing genuine emergency cases only in casualty and “non-casualty” cases being seen locally by specialist trained GPs and optometrists. Another option is to set up a joint hospital optometrist and ONP-led clinic to manage non-urgent cases within the A&E department; this would allow ophthalmologists to concentrate on the treatment of genuine emergency cases. However, these suggestions may only be applicable for a dedicated casualty department such as the one at Moorfields.
One limitation of the study was the exclusion of over 30% of the questionnaires because of incomplete data entry or because patients did not wish to participate, which invariably would have affected the outcome. The reasons for incomplete data entry might be insufficient time to complete the questionnaire, as most patients would have waited for a period of time before being seen in casualty. Because of time constraints, it was also not feasible for the clinic clerk to check each individual form properly before the patient left the hospital. It is also important to point out that this study was performed in a large urban 24 h ophthalmic casualty unit and the results may not be representative of other dedicated eye casualty units in the UK. Further studies are required to look at the effectiveness of these proposals in alleviating the large proportion of patients with non-acute conditions who attend A&E departments. Nevertheless, the results of this study show that a large percentage of patients who attend ophthalmic A&E departments are non-urgent cases which could be managed adequately in a primary care setting.
Acknowledgments
The authors thank the staff in Moorfields A&E department for their help with this audit.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.
Ethics approval: Local research ethics committee approval was sought prior to the start of the study and informed consent was obtained.
Linked Articles
- Primary survey