Article Text

Abstract
Objective To indirectly compare aflibercept, bevacizumab, dexamethasone, ranibizumab and triamcinolone for treatment of macular oedema secondary to central retinal vein occlusion using a network meta-analysis (NMA).
Design NMA.
Data sources The following databases were searched from January 2005 to March 2013: MEDLINE, MEDLINE In-process, EMBASE; CDSR, DARE, HTA, NHSEED, CENTRAL; Science Citation Index and Conference Proceedings Citation Index-Science.
Eligibility criteria for selecting studies Only randomised controlled trials assessing patients with macular oedema secondary to central retinal vein occlusion were included. Studies had to report either proportions of patients gaining ≥3 lines, losing ≥3 lines, or the mean change in best corrected visual acuity. Two authors screened titles and abstracts, extracted data and undertook risk of bias assessment. Bayesian NMA was used to compare the different interventions.
Results Seven studies, assessing five drugs, were judged to be sufficiently comparable for inclusion in the NMA. For the proportions of patients gaining ≥3 lines, triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2 mg had a higher probability of being more effective than sham and dexamethasone. A smaller proportion of patients treated with triamcinolone 4 mg, ranibizumab 0.5 mg or aflibercept 2 mg lost ≥3 lines of vision compared to those treated with sham. Patients treated with triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2 mg had a higher probability of improvement in the mean best corrected visual acuity compared to those treated with sham injections.
Conclusions We found no evidence of differences between ranibizumab, aflibercept, bevacizumab and triamcinolone for improving vision. The antivascular endothelial growth factors (VEGFs) are likely to be favoured because they are not associated with steroid-induced cataract formation. Aflibercept may be preferred by clinicians because it might require fewer injections.
Systematic review registration Not registered.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Important topic area, with significant policy implications.
-
Robust method used to identify studies.
-
Network meta-analyses are based on a number of assumptions.
-
Network meta-analysis is the best method to compare interventions in the absence of head-to-head trials.
Introduction
Central retinal vein occlusion (CRVO) dramatically reduces an individual's functioning and quality of life.1 It is estimated that the 15-year cumulative incidence of CRVO is 0.5%.2 Visual loss is caused by thrombosis of the central retinal vein which leads to a rise in venous pressure and an increase in vascular endothelial growth factor (VEGF), consequently causing an increase in vascular permeability. Macular oedema subsequently ensues with varying degrees of ischaemia and neovascularisation. Although CRVO is generally classified as ischaemic or non-ischaemic, ischaemia should be regarded as a spectrum.3 Cases with ischaemia carry a considerably worse prognosis as, in around one-third of them, neovascular glaucoma, the most devastating complication of CRVO, may develop.4
CRVO is more common in older people with risk factors such as diabetes, hypertension or hyperlipidaemia, but can occur in young people with inflammatory disorders. Hayreh et al, in a 27-year cohort study, found that only 13% of people with CRVO were under 45 years of age.3 In 95% of cases, CRVO affects only one eye.3 However, visual loss in this already comorbid patient group significantly compounds their already impaired functioning and quality of life. Patients can lose confidence, struggle with daily activities and become increasingly dependent on friends and family.1
For many years, laser photocoagulation was the only effective therapeutic strategy that could be used in the management of patients with CRVO. It was only useful for reducing the risk of neovascular glaucoma, but not effective for the treatment of macular oedema in CRVO.5 Over the past decade, a number of drugs to treat macular oedema have been introduced, including the steroids, triamcinolone and dexamethasone, and the anti-VEGFs, ranibizumab, bevacizumab, pegaptanib and aflibercept. Dexamethasone, ranibizumab and aflibercept have been assessed in large commercially funded trials.6–13 Bevacizumab was originally developed as an anticancer drug and has been found to be effective in treating macular oedema secondary to age-related macular degeneration,14 diabetic macular oedema,15 branch retinal vein occlusion16 and CRVO.17 Like triamcinolone, bevacizumab is used off license in the eye. Ranibizumab is derived from the same parent molecule of the bevacizumab monoclonal antibody and was developed and commercially marketed specifically for use in the eye.
In the UK, the National Institute of Health and Care Excellence (NICE) has recommended the use of dexamethasone, ranibizumab and aflibercept for the treatment of macular oedema secondary to CRVO in separate appraisals.18–20 Therefore clinicians have three NICE-recommended treatments for CRVO without head-to-head trials or clear guidance in which one may be best for their patients. On this basis, the aim of this study was to indirectly compare, in a network meta-analysis (NMA), the clinical effectiveness of aflibercept, ranibizumab, bevacizumab, dexamethasone and triamcinolone for the treatment of macular oedema secondary to CRVO.
Methods
Information sources and search strategy
To identify suitable studies, initially for a systematic review of treatment of macular oedema after CRVO (submitted for publication), the following databases were searched from January 2005 to March 2013: MEDLINE, MEDLINE In-process, EMBASE (all via OVID); CDSR, DARE, HTA, NHSEED, CENTRAL (all via The Cochrane Library); Science Citation Index and Conference Proceedings Citation Index-Science (via Web of Knowledge). The MEDLINE search strategy is shown in the online supplementary appendix 1. This search strategy was modified for other databases. In addition to the bibliographic database searching, supplementary searches were undertaken to look for recent and unpublished studies in the WHO International Clinical Trials Registry Platform and ophthalmology conference websites (American Academy of Ophthalmology, Association for Research in Vision and Ophthalmology from 2010 to 2012).
Study selection
Only randomised controlled trials which included patients with macular oedema secondary to CRVO were included. It was acceptable for a study to include branch retinal vein occlusion and CRVO provided that the CRVO group was reported separately. The following drugs were included: dexamethasone, triamcinolone, ranibizumab, bevacizumab and aflibercept. Pegaptanib was not included because it is not used routinely in clinical practice. Only doses that are used in clinical practice were included. Studies had to report at least one of the following outcomes: proportions of patients gaining ≥3 lines from baseline to 6 months, proportions of patients losing ≥3 lines from baseline to 6 months and the mean change in best corrected visual acuity (BCVA) from baseline to 6 months.
Risk of bias assessment
The Cochrane Collaboration's tool was used for assessing risk of bias.21 The trials were graded (unclear, high or low risk of bias) based on: (1) sequence generation, (2) allocation concealment, (3) blinding of outcome assessor, (4) incomplete outcome data and (5) selective outcome reporting.
Study selection and data abstraction
Two authors independently assessed the eligibility and methodological quality of the studies identified during the literature search. Two authors extracted and compared the data. For each study identified that met the selection criteria, details on study design, study population characteristics, intervention, outcome measures and study quality were extracted. Discrepancies were resolved by consensus through discussion. Studies were assessed for comparability based on the populations included, trial arms, outcome measures and duration of follow-up. Common comparators were identified from the trials and a network diagram was created.
Summary measures
The primary measures of treatment effects were relative risk (RR) for the proportions of patients gaining ≥3 lines of vision, proportions of patients losing ≥3 lines of vision and the weighted mean difference (WMD) for mean change BCVA. We used the following methods to calculate SDs when incompletely reported: (1) contact with the corresponding author or (2) estimation of the SD on the basis of the sample size, median and range as suggested by Hozo et al22 or on the basis of the sample size and p value.
In one trial (SCORE),23–36 6-month data were not available because patients were followed up every 4 months. For the dichotomous outcomes, that is, proportions of patients gaining and losing ≥3 lines, we averaged 4 and 8-month data to get the 6 months follow up data. For the third outcome, that is, mean change BCVA, again data from two time-points were used. The weighted mean and SDs for each treatment arm were calculated using the mean and SDs of two time-points.
Data synthesis and model implementation
Bayesian NMA37 ,38 was used to compare the different interventions. NMA is a generalisation of meta-analysis methods because it allows comparisons of agents not addressed within individual primary trials. Bayesian statistical inference provides probability distributions for treatment effect parameters (RR and WMD), with 95% credible intervals (95% CrI), rather than 95% CIs (95% CI). A 95% CrI can be interpreted as there being a 95% probability that the parameter takes a value in the specified range.37 ,38
All analyses were conducted using a Bayesian Markov Chain Monte Carlo (MCMC) method and fitted in the freely available Bayesian software, WinBUGS V.1.4.3.39 Two Markov chains were run simultaneously using different initial values. Convergence to a stable solution was checked by viewing plots of the sampled simulations and using the Brooks-Gelman-Rubin diagnostic tool.40 Convergence was found to be adequate after running 20 000 samples for both chains. These samples were then discarded and a further 70 000 sampled simulation was then run, on which the results were based. We also calculated the probability of treatment being the most effective (first best), the second best, the third best and so on, and presented the results graphically with rankograms.41
Like standard meta-analysis comparison, an NMA can be either a fixed-effect or a random-effect model. We used the Bayesian Deviation Information Criterion (DIC) to compare fixed-effect and random-effect models. The most appropriate NMA model can be identified as the one with the lowest DIC. The DIC measures the fit of the model while penalising it for the number of effective parameters. The fixed-effect model was chosen because of the small number of trials available for each comparison, and difficulty in estimating between studies variance, if random-effect model, was implemented, and the difference in DIC was less than 5.
Results
Study selection and characteristics
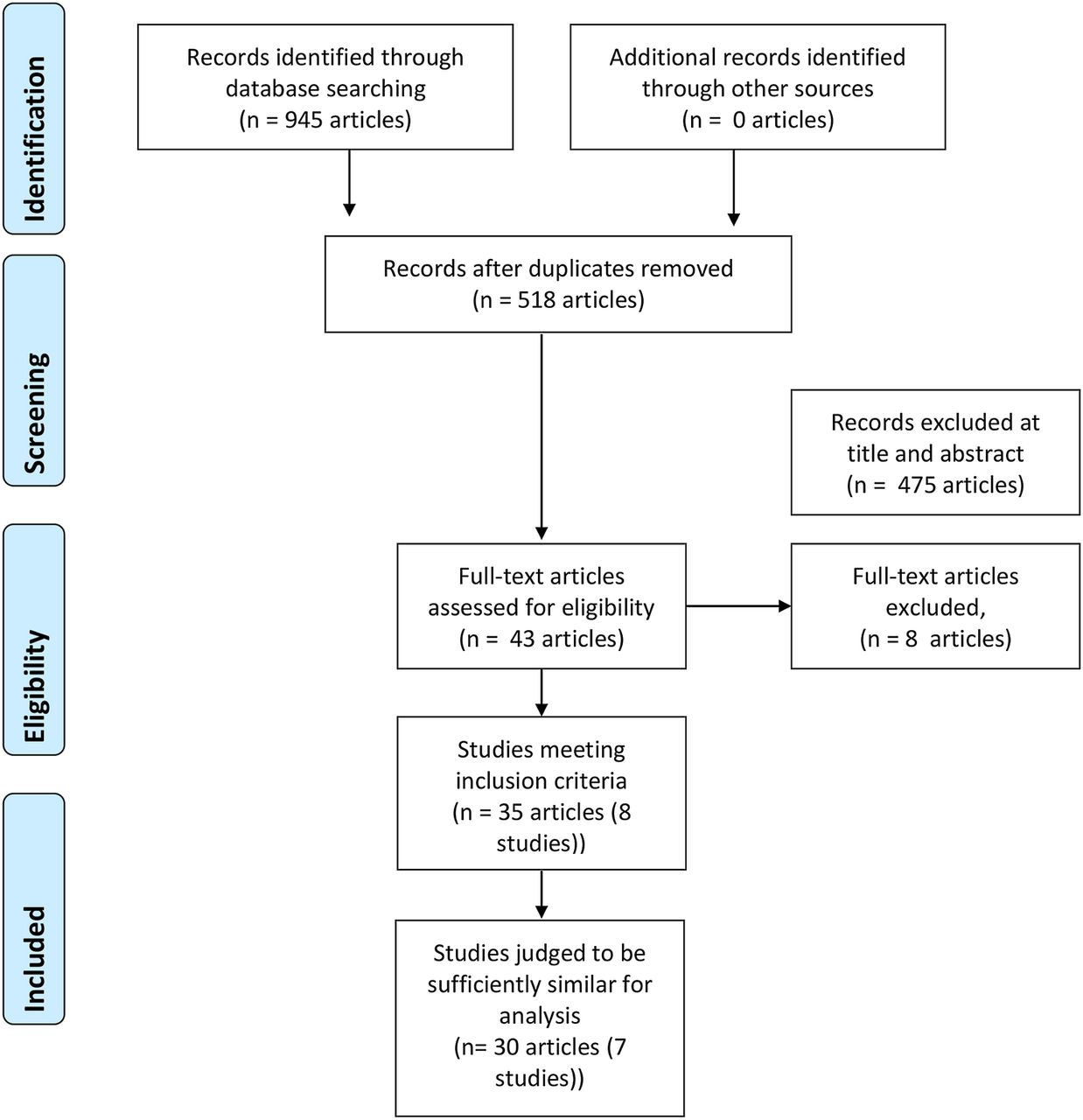
The literature search identified 945 articles, as shown in figure 1. Seven studies were judged to be sufficiently comparable to be included in the NMA. Tables 1 and 2 present the characteristics and results of the included trials. Two studies11–13 compared aflibercept 2 mg against sham; two identical studies6–8 compared dexamethasone 0.7 mg (Ozurdex) against sham; one study9 ,10 compared ranibizumab 0.5 mg against sham; one study42–44 compared bevacizumab 1.25 mg against sham and, finally, one study23–36 compared triamcinolone 4 mg against observation. Sham or observation was used as the common comparator. The number of included participants varied from 6042–44 to 437.6–8 Most studies required patients to be treatment naïve and have macular oedema with retinal thickness measuring at least 250 or 300 μm on optical coherence tomography. Sham injection was undertaken by placing a needleless syringe on the eye. All studies, except for Epstein et al,42–44 were multi-centre, international studies. Most studies had an extension phase after the primary outcome, but this was not included in the NMA.
Baseline characteristics and results of all included studies
Baseline characteristics and results of included trials

Study selection flow diagram.
The sufficiently comparable studies were combined into a network analysis based on a common comparator. The network for the proportions of patients gaining ≥3 lines is shown in figure 2. This network is the same for the other two outcomes, but without dexamethasone, because the trial did not report these outcomes.

Network of randomised controlled trials comparing different treatments for proportions of gaining three or more lines of vision.
Risk of bias of included trials
Risk of bias is shown in table 3. Included studies were generally of high quality, with all studies being judged to be of low or unclear bias for all criteria. The non-commercially funded bevacizumab trial had fewer patients and, inevitably, results had wider CIs.42–44 In no study does it appear that patients were asked at the end of the trial which arm they thought they had been assigned. It is unclear how many could distinguish injections (intervention arm) from punctureless pressure (sham arm).
Risk of bias
Effects of interventions on proportions of patients gaining ≥3 lines
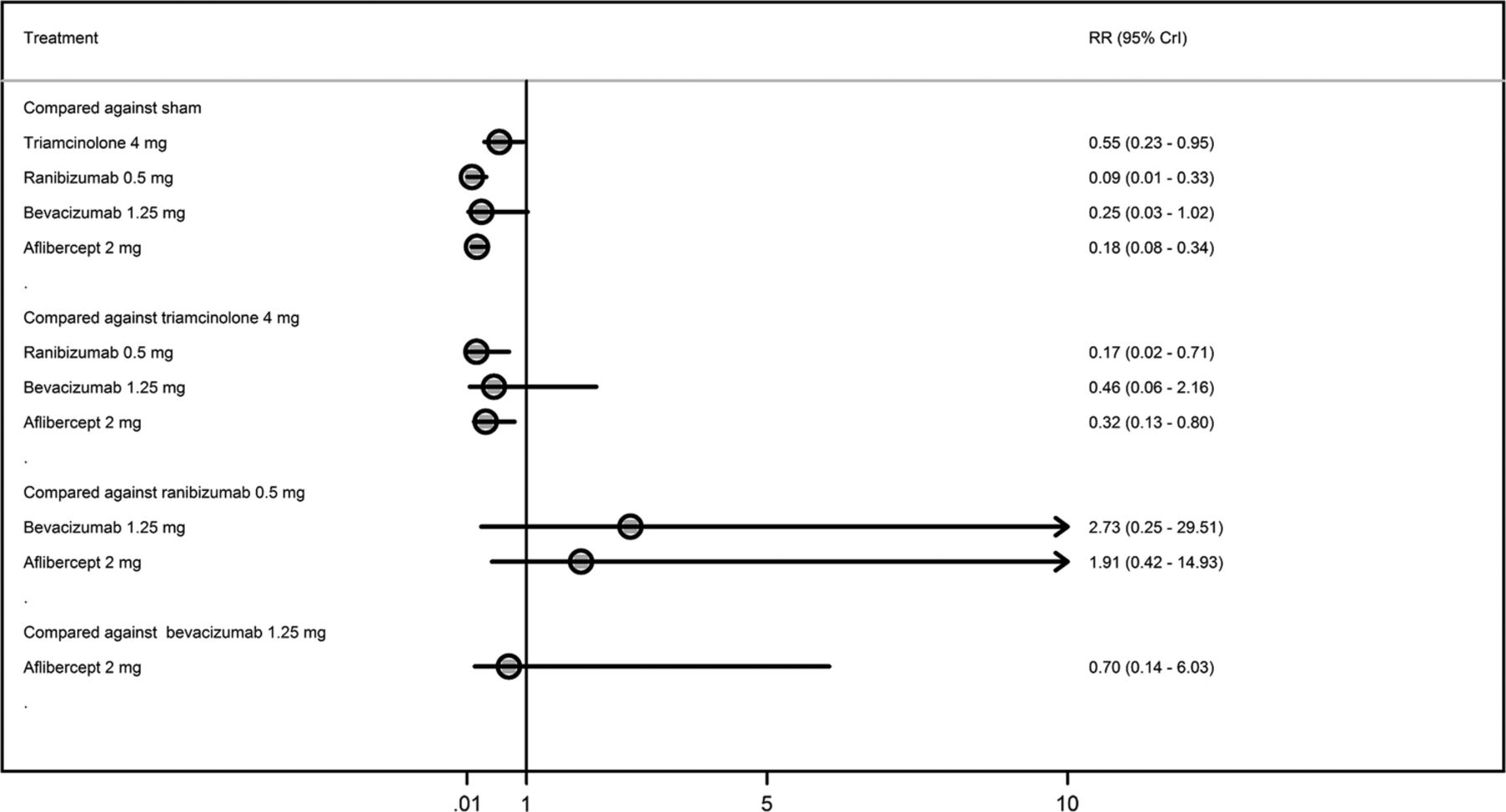
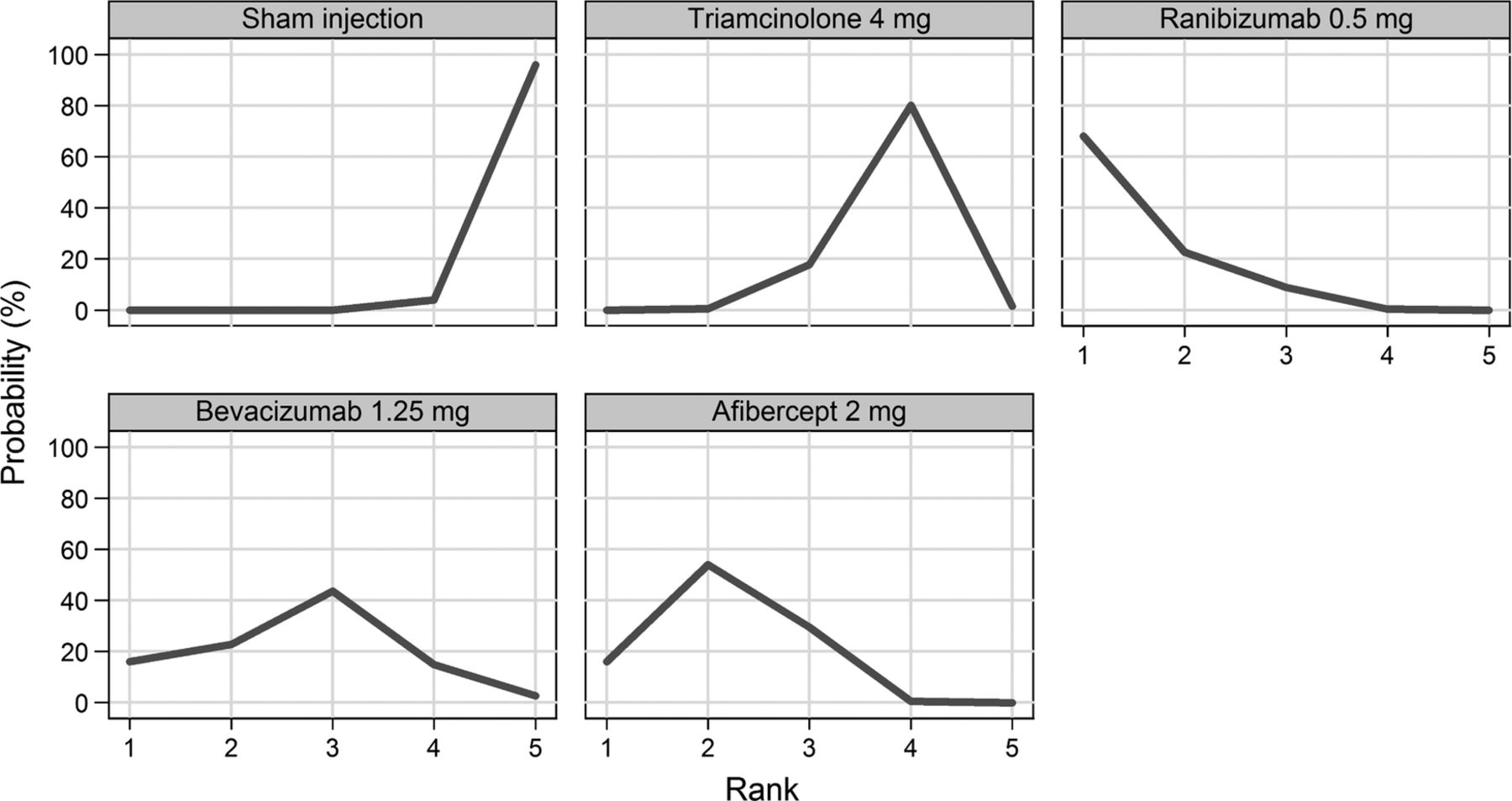
Figure 3 displays a forest plot of the risk ratio and 95% CrI in proportions of patients gaining ≥3 lines for all the possible pairwise comparisons. In terms of proportions of patients gaining ≥3 lines, triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2 mg had a higher probability of being more effective than a sham and dexamethasone (figure 4). There was no difference in the proportions of patients gaining ≥3 lines between triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2mg.

Proportions of patients gaining three lines or more from baseline to 6 months.

Rankogram for gaining ≥3 lines—distribution of the probabilities of every treatment being ranked at each of the possible six positions.
Effects of interventions on proportions of patients losing ≥3 lines
Figure 5 displays forest plot of the risk ratio and 95% CrI of proportions of patients losing ≥3 lines for all the possible pairwise comparisons. A smaller proportion of patients treated with triamcinolone 4 mg, ranibizumab 0.5 mg or aflibercept 2 mg lost ≥3 lines of vision than those treated with sham. There was no difference in the proportions of patients losing ≥3 lines between triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2 mg. Figure 6 shows ranking for efficacy in terms of proportions of patients losing ≥3 lines.
Proportions of patients losing three lines or more from baseline to 6 months.

Rankogram for losing ≥3 lines—distribution of the probabilities of every treatment being ranked at each of the possible six positions.
Effects of interventions on mean change in BCVA
Figure 7 displays a forest plot of the mean changes and 95% CrIs of improvement in BCVA for all the possible pairwise comparisons. Patients treated with triamcinolone 4 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg or aflibercept 2 mg had a higher probability of improvement in BCVA compared to those treated with sham injections. Patients treated with aflibercept 2 mg had a higher probability of improvement in BCVA compared with those treated with triamcinolone 4 mg (figure 8). There was no difference in the mean change in BCVA from baseline between patients treated with ranibizumab 0.5 mg, bevacizumab 1.25 mg and aflibercept 2 mg.

Mean best corrected visual acuity change from baseline to 6 months.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rankogram for mean change in best corrected visual acuity—distribution of the probabilities of every treatment being ranked at each of the possible six positions.
Discussion
Statement of principal findings
Our results show no evidence of a difference in effectiveness between aflibercept, ranibizumab and triamcinolone. Bevacizumab was similar to these drugs in terms of letters gained and the mean change in BCVA. Dexamethasone was less effective compared with these drugs.
Strengths and limitations
This is the first study providing an indirect comparison of drugs to treat macular oedema secondary to CRVO. A robust search strategy, screening process and data extraction were used, and this analysis drew on a systematic review. The studies included had, in general, a low risk of bias. Safety was not considered in this study but is described in detail elsewhere.45 Five different drugs were suitable for NMA. Unpublished data were obtained from one author.42–44 Bayesian methods were used for the NMA. There was good model fit and convergence within the analysis.
However, pre-specified outcomes were not reported in all studies and the sample size varied considerably. For example, Epstein et al, 42–44 assessing bevacizumab, only included 30 participants in each arm. This resulted in wide CrIs from the NMA, which could have led to a type 1 error, especially with regard to the proportions of patients losing ≥3 lines. The SCORE study compared triamcinolone to observation.23–36 The NMA assumes a11 similar effect of sham and observation and this may result in a small degree of bias. Only 6 months of data were included, and the long-term effects are not known. Using a 6-month follow-up period may disadvantage dexamethasone because peak effect in the GENEVA trials was seen at 90 days, and by 6 months, benefits had been largely lost.6–8
As with most network meta-analyses, methodological heterogeneity was present. There were some differences among the trials. For example, CRUISE,9 ,10 assessing ranibizumab, did not include as many patients with ischaemic CRVO as the aflibercept trials.12 ,13 There were also some small differences in the chronicity of macular oedema and the mean BCVA at baseline.
Meaning of the study: possible explanations and implications for clinicians and policymakers
No head-to-head trials comparing aflibercept, bevacizumab, ranibizumab, triamcinolone and dexamethasone have been published in CRVO. Part of the reason for this is that the Food and Drug Administration requires proof of the safety and effectiveness of a drug.46 The easiest and quickest method for pharmaceutical companies to produce this proof is through placebo controlled trials. Trials comparing new medications to current best treatment would be considerably more useful to clinicians and patients.
Head-to-head trials comparing some of these drugs are available in other conditions. For example, a comparison of ranibizumab and bevacizumab was undertaken in age-related macular degeneration in the Comparison of Age-related macular degeneration Treatment Trials (CATT)47 and alternative treatments to Inhibit VEGF in patients with Age-related choroidal Neovascularisation (IVAN)48 trials. Both of these trials found no difference in effectiveness between ranibizumab and bevacizumab. Furthermore, an indirect comparison of ranibizumab and bevacizumab found no evidence of a difference between these drugs.49 Thus, it is highly probable that this may also apply in CRVO. The difference seen in our results regarding bevacizumab may be due to the low number of patients included in Epstein et al.42–44 In the CATT trial, more patients were hospitalised in the bevacizumab arm, but the authors did not believe that this was explained by a direct effect of bevacizumab.47 The 2-year results from the IVAN showed little difference in cardiovascular events, with the number being insignificantly lower with bevacizumab.50 Ranibizumab and aflibercept were directly compared in two similarly designed trials, VEGF Trap-eye: investigation of Efficacy and safety in Wet age-related macular degeneration (VIEW 1 and 2).51 Similar efficacy and safety was found in both drugs.
From the included trials it is clear that intraocular steroids are associated with complications, including increased intraocular pressure and cataract formation.6–8 23–36 These are substantial drawbacks for using steroids to treat macular oedema in CRVO. However, many affected patients may already be pseudophakic and, on these, the use of intraocular steroids may be reasonable. Steroids may have a place in the treatment pathway of patients who have failed on anti-VEGF therapy, but this is yet to be tested. The anti-VEFG drugs have a good safety profile and do not cause cataract formation.9–13 42–44 For this reason they are more likely to be favoured by clinicians than steroids.
Aflibercept, compared with ranibizumab and bevacizumab, targets a wider range of cytokines and may have a stronger binding affinity.52 Initial results suggested that aflibercept would require fewer injections than ranibizumab.51 Heier and colleagues compared aflibercept and ranibizumab in two similarly designed randomised controlled trials in age-related macular degeneration. They found that 2 mg aflibercept administered every 8 weeks produced similar effects at 96 weeks to 0.5 mg ranibizumab administered every 4 weeks.51 This was reflected in the FDA Dermatologic and Ophthalmic Drugs Advisory Committee recommendation that aflibercept should be given every 2 months following three initial monthly doses in age-related macular oedema.53 This may be because aflibercept also appears to last longer in the eye than ranibizumab.54 Age-related macular degeneration is a more aggressive condition than CRVO and so it is unlikely that more frequent dosing would be needed. Therefore, aflibercept may be preferred because it would reduce pressure on outpatient clinics. Furthermore, there is some evidence from patients with age-related macular degeneration that aflibercept may be effective in patients who have not responded to ranibizumab.55 ,56 This may be due to the higher affinity and wider number of cytokines that are targeted. There is no reason to suspect that these effects are any different for the macular oedema caused by CRVO. However, we have as yet no evidence as to whether ranibizumab would be effective after aflibercept has failed.
The National Institute of Health and Care Excellence has recommended dexamethasone, ranibizumab and aflibercept as options in the treatment of macular oedema secondary to CRVO.18–20 Until these technologies are reviewed together and compared with each other, clinicians are left with three recommended drugs. It should be noted that during the appraisal of ranibizumab the evidence review group found that in the cost-effectiveness analysis dexamethasone was extendedly dominated by ranibizumab (an intervention is judged not be cost-effective because it has an ICER that is greater than that of a more effective intervention). The committee appraising ranibizumab did not re-consider the previous appraisal decision on dexamethasone.
Our results show that dexamethasone was not as effective as ranibizumab or aflibercept, at 6 months follow-up and with the dosing regimens in the trials. However, these results do not assess quality of life or cost effectiveness. Bevacizumab is likely to prove more cost effective than both aflibercept and ranibizumab because it is substantially less expensive.57 However, the National Institute for Health and Care Excellence has not issued guidance on bevacizumab because it does not have a license for use in the eye.
Unanswered questions and future research
Not all patients benefit from the use of anti-VEGF drugs; only about 60% gain 15 or more letters. It is not clear why some patients benefit more than others. Future research should focus on identifying subgroups of patients who are likely to benefit. Only a few of the trials included ischaemic patients, and in those trials only a few patients with ischaemia were included.11–13 More research assessing the effectiveness of these drugs in severely ischaemic patients is needed.
Head-to-head trials comparing ranibizumab, aflibercept, bevacizumab and triamcinolone are needed. These should include assessment of cost effectiveness. To assist this, a better measure of quality of life is needed for patients with eye conditions. The widely used EQ5D may not be sensitive enough to measure changes that are important to patients, such as the ability to drive.
In conclusion, we have found no evidence of differences between ranibizumab, bevacizumab, aflibercept and triamcinolone for improving vision. The anti-VEGFs are likely to be favoured because they are not associated with steroid-induced cataract formation. Clinicians may prefer Aflibercept because it might require fewer injections.
Acknowledgments
The authors thank Christine Clar, Sian Thomas and Rachel Court for assisting with searches, screening and data extraction for the systematic review that precedes this study. They also thank the authors of the Epstein 2012 trial for providing addition data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors NW conceived the idea. All authors contributed to the design of the study. DS and OAU undertook the statistical analysis. JAF, DS and OAU wrote the first draft of the manuscript. All authors redrafted and agreed on the final article. JAF is the guarantor.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.