Article Text

Abstract
OBJECTIVES Cerebellar haemangioblastoma occurs sporadically or as a component tumour of autosomal dominant von Hippel-Lindau disease. Biallelic inactivation of the VHL tumour suppressor gene, which is located on chromosome 3p, has been shown to be involved in the pathogenesis of both tumour entities. Mechanisms ofVHL inactivation are intragenic mutations, mitotic recombination events, and hypermethylation of the promoter region. The systematic and complete examination of these genetic and epigenetic phenomena in large series of von Hippel-Lindau disease related and sporadic hemangioblastomas has, thus far, not been performed.
METHODS In the largest series to date, 29 von Hippel-Lindau disease associated and 13 sporadic haemangioblastomas were investigated for all suggested inactivating mechanisms of theVHL gene using single strand conformational polymorphism (SSCP), loss of heterozygosity (LOH), and methylation analyses. Additionally, corresponding blood samples of all patients were screened for VHL germline mutations by SSCP and Southern blotting.
RESULTS Germline mutations were identified in 94% of patients with von Hippel-Lindau disease and their tumours and 62% of these hemangioblastomas showed LOH of chromosome 3p. Of the 13 sporadic tumours, 23% showed a single somatic mutation of theVHL gene that was not present in the germline. 3p LOH was identified in 50% of informative sporadic tumours. No von Hippel-Lindau disease related or sporadic tumour demonstrated VHLpromoter hypermethylation.
CONCLUSIONS For most von Hippel-Lindau disease related haemangioblastomas, the inactivation or loss of both alleles of theVHL gene, as predicted by the Knudson two hit theory, is required. However, in a subset of tumours including most sporadic haemangioblastomas, the genetic pathways involved in tumorigenesis have yet to be defined and may represent alterations of a different pathway or pathways.
- hemangioblastoma
- von Hippel-Lindau disease
- tumour suppressor gene
- DNA methylation
Statistics from Altmetric.com
Haemangioblastomas are benign and usually cystic tumours which are predominantly found in the cerebellum of adults. They occur as a sporadic entity or as part of von Hippel-Lindau disease, an autosomal dominant disorder which is characterised by CNS haemangioblastomas and, in addition, by retinal angiomas, renal cell carcinomas, and pheochromocytomas.1
The VHL susceptibility tumour suppressor gene maps to 3p25–26 and was identified in 1993.2 The three exons contain a coding sequence of 852 nucleotides. Germline mutations within the VHL gene have been identified in up to 100% of affected families.3 Suggested functions of the VHL gene are (1) down regulation of hypoxia inducible mRNAs4; (2) proper assembly of the extracellular fibronectin matrix5; (3) regulation of exit from the cell cycle6 and (4) regulation of expression of carbonic anhydrases 9 and 12.7 TheVHL gene seems to be a classic tumour suppressor gene with biallelic inactivation by two genetic alterations. In von Hippel-Lindau disease, the first hit is an inherited germline mutation which is present in one allele in each cell of the body. It is often a “small” intragenic mutation. The second hit is a somatic DNA alteration which is acquired during the patient's lifetime and is present only in the tumour tissue. Known somatic inactivating mechanisms include recombination events resulting in a loss of heterozygosity (LOH) of the VHL gene, and to a lesser extent intragenic point mutations. Recently, hypermethylation of normally unmethylated sites of the promoter that are rich in 5′-CG-3′ dinucleotides, so called CpG islands, has been suggested as an epigenetic mechanism of tumour suppressor gene inactivation.8 Genomewide changes in methylation pattern are known to occur in all forms of neoplasia. Although non-island CpGs become hypomethylated, certain CpG islands become densely hypermethylated. Furthermore, in normal tissues, extensive methylation of promoter region CpG islands is associated with transcriptional silencing. This is well known for imprinted alleles and genes on the inactive X chromosome.9 The role of tumour suppressor gene hypermethylation, however, is still unclear in many tumours.
Previous genetic studies on CNS haemangioblastomas either did not analyse both von Hippel-Lindau disease related and sporadic tumours or did not investigate all known mechanisms of gene inactivation. These studies have yielded a broad range of different results10-16 which may be a consequence of the investigation of only small series.
To get a more complete and reliable picture ofVHL gene function in haemangioblastoma pathogenesis, we sought to examine and compare an extensive series of 29 von Hippel-Lindau disease associated and 13 sporadic hemangioblastomas for all suggested mechanisms ofVHL inactivation.
Methods
PATIENTS AND TUMOUR SAMPLES
A total of 42 CNS haemangioblastoma samples were obtained from 31 patients, who were consecutively treated between 1993 and 1997 at the Department of Neurosurgery of the Freiburg University Medical Centre. The series comprised 29 von Hippel-Lindau disease associated tumours obtained from 18 patients with the disease and 13 sporadic tumours, which were obtained from 13 patients with no clinical signs of a tumour syndrome. Eighty three per cent of disease associated and 62% of sporadic tumours were located in the cerebellum. The diagnosis of von Hippel-Lindau disease was established by the criteria of Neumannet al 17 The tumours were from 11 male and 20 female patients. The age at operation ranged from 16 to 71 years with an average of 38 years. The tumour samples were snap frozen in liquid nitrogen and were stored at −80°C until the molecular genetic investigations were performed. All tumours were classified histopathologically according to the World Health Organisation classification.18
For germ line analysis blood samples were available from all patients. Our study was approved by the ethics committee of the University of Freiburg and our patients gave informed consent.
MOLECULAR GENETIC ANALYSES
Genomic and tumour DNA was isolated by standard methods.19 Southern blotting was performed to detect large deletions in the VHL gene. Genomic DNA (7 μg) was digested with excess Eco RI (Boehringer Mannheim). The fragments were separated in a 0.6% agarose gel with 1×TBE buffer and transferred to a positively charged nylon membrane (Boehringer Mannheim) by capillary blot. Fragments were visualised with the DIG high prime labelling and detection starter kit I (Boehringer Mannheim) according to the supplier. The probes for hybridisation of the Southern blot were made by two sets of primers, one in the very beginning of exon 1 and another set in the 3′ untranslated region of exon 3.
Single strand conformation polymorphism (SSCP) analysis was used to find point mutations, small deletions, or insertions. Four sets of primers were needed to cover all three exons. Mixtures contained 100 ng genomic DNA, 0.2 mM dNTP, 0.5 pmol/μl of each primer, MgCl2 and 0.1 U/μl Taq DNA polymerase (Gibco BRL). Polymerase chain reaction (PCR) conditions and sets of primers have been previously described.20 Polymerase chain reaction amplified fragments (10 μl) were denatured by adding 15μl denaturing solution (containing 95% formamide, 10 mM NaOH, 0.05% xylene cyanol, 0.05% bromophenol blue) and heating to 96°C for 3 minutes before chilling on ice. Denatured fragments were separated on a polyacrylamide gel (MDETM Gel Solution, FMC Bioproducts Europe) with 0.5×MDE and 0.6×TBE buffer according to the manufacturer. After separation at 200 V for 16 hours the fragments were stained with silver according to established protocols.21Aberrant bands were cut out of the gel, dissolved in water, and reamplified for sequencing, which was performed with nested fluorescence labelled primers using the dideoxy method and a semiautomatic sequencer (Alf, Pharmacia). All mutations were confirmed by sequencing. Thus we newly detected or reconfirmed germline mutations as previously described in a larger series of our patients.22
Altogether, three polymorphic markers on chromosome 3p were used for the LOH analysis of the VHL gene including one dinucleotide repeat polymorphism (D3S1038), which is located close to the VHL locus at 3p25–26,23and two restriction fragment length polymorphism (RFLP) markers, which are located directly within the VHL gene: One Hae III RFLP marker is located at the nucleotide 19 of the VHLgene,28 the other one is a PCR generatedAcc I RFLP marker, which is located at nucleotide 1149 in the 3′ untranslated region ofVHL.24
For investigation of VHL promoter hypermethylation, we performed a PCR based technique using the methylation sensitive enzyme Ehe I, which has two recognition sites within the CpG island of theVHL promoter: Genomic DNA (1 μg) was digested with 10 U Ehe I (MBI Fermentas) and buffer Y+/TangoTM in a total volume of 150 μl at 37°C for 16 hours. Ehe I has the recognition sequence 5′-GGCGCC-3′ within exon 1 and will not cleave if the internal cytosine is methylated. To ensure complete digestion, a further 5 U Ehe I was added after digestion and the sample was incubated for another hour at 37°C. Before the PCR was performed, the sample was purified with GeneClean II DNA purification Kit (Bio 101) according to the supplier's instructions. The digested DNA was redissolved in 20 μl Tris-EDTA-buffer. Two microlitres were used for the following 15 μl multiplex PCR. One set of primers flanked the Ehe I sites within exon 1 (F:5′-GAG GCA GGC GTC GAA GAG TAC GGC-3′, R: 5′-GAC TGC GAT TGC AGA AGA TGA CCT-3′ and will only amplify in cases whereEhe I did not cleave—that is, in the presence of VHL gene methylation. As a control for failure of the PCR, a second pair of primers was used (F: 5′-CTG AGA CCC TAG TCT GCC ACT GAG-3′ R: 5′-CAA AAG CTG AGA TGA AAC AGT GTA-3′) to amplify exon 3, which has no EheI restriction site. The reaction volumes contained 2 μM primers, 0.2 mM dNTPs, and 0.5 U Taq polymerase (GIBCO BRL). Fragments were amplified for 27 cycles of 30 seconds at 95°C, 40 seconds at 62°C, and 30 seconds at 72°C. As a second control, the same procedure was carried out for each DNA sample without enzyme to ensure correct amplification of exon 1.
Results
All CNS haemangioblastomas were investigated for alterations of the VHL gene by SSCP, LOH, and methylation analyses. Additionally, corresponding blood samples of all von Hippel-Lindau disease and sporadic patients were screened forVHL gene mutations by SSCP and Southern blot analysis. The results are listed in table 1.
Mutations of the VHL gene in VHL related and sporadic haemangioblastomas of the CNS. 42 tumours from 31 patients were investigated
Analysis of the blood samples by SSCP disclosed abnormal electrophoretic patterns in the germline of 14 out of 18 patients with von Hippel-Lindau disease. Subsequent sequencing showed that 10 patients had missense mutations, two had in frame insertions, and one had a nonsense mutation. In one patient (9), no mutation could be detected by sequencing, although the SSCP electrophoretic pattern was abnormal. The results of sequencing are summarised in table 1. Southern blot analysis of the germline DNA disclosed deletions of 2 kb within the VHL gene in four patients with von Hippel-Lindau disease, who had no SSCP aberrations. Thus, a germline mutation was identified in 17 of 18 (94%) patients with the disease.
All disease related tumours showed the same mutation as the corresponding blood sample and no disease related tumour showed a somatic mutation in addition to the germline mutation. Three of the 13 sporadic tumours had a single somatic mutation including one nonsense and two frameshift mutations (table 1). The nonsense mutation (R161X) in the sporadic tumour 28 has been described before as a germline mutation.25 The two other mutations have not been described so far.
The results of the LOH analysis are summarised in figure 1. Allelic losses on chromosome 3p were found in 13 of 21 informative von Hippel-Lindau disease tumours (62 %) and in five of 10 informative sporadic tumours (50%). Interestingly, only one of the three sporadic haemangioblastomas with a somatic VHL gene mutation showed LOH on distal chromosome 3p. Eight of the disease associated tumours and three sporadic tumours were homozygous for all of the investigated loci and therefore not informative for LOH analysis. Thus they could not be included in the statistics.
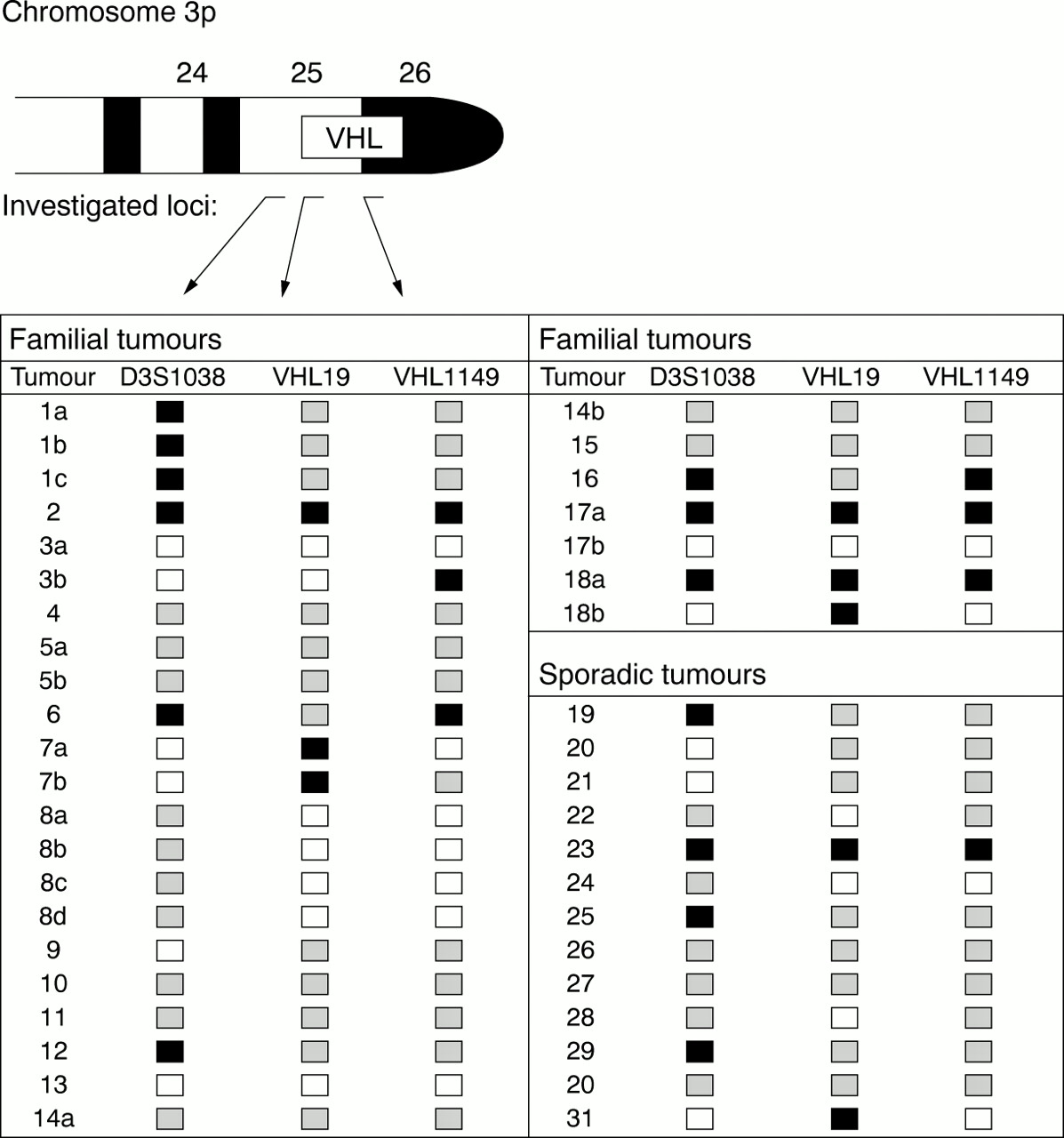
Results of LOH investigations in VHL and sporadic haemangioblastomas. Three different loci on chromosome 3p were investigated. A PCR generated Acc I RFLP at nt 1149 and a Hae III RFLP at nt 1928 were located within the VHL gene, mapped to 3p25-26. The third one was a dinucleotide repeat polymorphism, D3S1038, located at 3p25.23 Black squares=LOH; open squares=retained heterozygosity; grey squares=not informative.
In some patients with von Hippel-Lindau disease, we had the possibility of studying more than one tumour and looked for correlations between these. In four of these patients (1, 7, 8, and 18) the different tumours had the same underlying genetic changes; however, in two patients (3 and 17) the changes differed.
The methylation analysis did not show hypermethylation of theVHL gene promoter region in any of the investigated tumours. This was indicated by failure of amplification of the promoter fragment in all tumour and blood samples that were digested with Ehe I. All undigested samples amplified correctly and the exon 3 control fragment also amplified in each case.
Discussion
Previous reports on mutation analysis of theVHL gene in von Hippel-Lindau disease related and sporadic CNS haemangioblastomas have yielded a broad range of different results.10-16 This phenomenon might be the consequence of only a few cases in the investigated series and the incomplete analysis of VHL gene inactivating mechanisms. Here we have systematically and rigorously investigated theVHL gene for all known inactivating mechanisms in the largest study to date.
Reported frequencies of LOH on chromosome 3p in disease related haemangioblastomas are 14% (1/7),15 27% (3/11),16 66% (2/3),12 and 100% (4/4)13 with an average of 40%. Our investigations showed 3p LOH in 13 of 21 informative von Hippel-Lindau disease tumours (62 %), indicating that a classic two hit inactivation ofthe VHL gene is a common mechanism in disease associated haemangioblastomas (fig 2). In our sporadic tumours we detected LOH of the telomeric 3p region in 50% of cases. These results are in good agreement with two previous studies, which have found allelic loss on 3p in ½12 and 10/1914sporadic CNS haemangioblastomas.

{kind=link}
{kind=link}
Haemangioblastoma associated with von Hippel-Lindau disease and sporadic hemangioblastoma.
Previous investigations on hypermethylation of theVHL gene in CNS haemangioblastomas have yielded different results and were based on small series. Prowseet al found hypermethylation in four of eight investigated von Hippel-Lindau disease related CNS haemangioblastomas.16 By contrast, Tseet al investigated eight (three disease associated and five sporadic) haemangioblastomas and did not detect hypermethylation of the VHL gene in any of the tumours.12 In agreement with the second study we could not find any hypermethylation of the VHLgene promoter region. Both previous groups used methods that were similar to ours, which is digestion with a methylation sensitive restriction enzyme and subsequent PCR with flanking primers. However, the particular enzymes used were different (Sma I and NotI I versus Ehe I in our study). The different results can eventually be explained by different levels of sensitivity. Quantitative analyses of methylation might help to clarify this controversial issue.
With our SSCP method, which has been shown to have a sensitivity of 86% in detecting VHL germline mutations26 we have found only three somaticVHL gene mutations, all of which occurred in sporadic haemangioblastomas. Only one of these tumours showed biallelicVHL gene inactivation due to an additional LOH of the VHL gene region at 3p. The relatively low frequencies of somatic VHLgene mutations in sporadic hemangioblastomas and biallelicVHL gene inactivation agree with three previous studies, in which somatic mutations have been reported with an average of 18% (7/38).10-12 14 In previous studies, no sporadic tumour has been shown to have biallelicVHL gene inactivation, as these studies did not investigate all inactivating mechanisms, or the tumours retained heterozygosity. By contrast, our investigation of all knownVHL gene inactivating mechanisms is now highly suggestive that biallelic VHL gene inactivation is not a common mechanism in the tumorigenesis of sporadic CNS haemangioblastoma. This is very interesting, as until now, the “classic” Knudson two hit mechanism was viewed as dogma for theVHL gene in both von Hippel-Lindau disease associated and sporadic haemangioblastoma.10 11 14Furthermore, the fact that five of 10 sporadic tumours showed 3p LOH, but four of them lacked structural VHL gene alterations implies that the VHL gene plays a minor role in the sporadic tumours and that there are other genes on chromosome 3p with involvement in haemangioblastoma tumorigenesis. This has already been suggested for clear cell renal cancer, where mutations in tumour suppressor genes at 3p14-p21 seem to have a primary role in tumorigenesis in tumours with 3p LOH but withoutVHL gene inactivation.27
In summary, our data suggest that the genetic pathways involved in pathogenesis in von Hippel-Lindau disease haemangioblastoma versus sporadic haemangioblastoma are distinct. Further investigations on chromosome 3p in CNS haemangioblastomas might clarify this hypothesis further.
Acknowledgments
This work was supported by a grant from the Centre of Clinical Research of the University of Freiburg, Germany.