Article Text

Abstract
Aims: To measure spectacle dependence following bilateral monofocal intraocular lens (IOL) implantation and assess how it is predicted by postoperative refraction.
Methods: 300 cataract patients had bilateral phacoemulsification surgery with monofocal IOL implantation. A spherical equivalent of 0 to −0.5 D was targeted. Three months after surgery, patients answered a questionnaire and had a spectacle refraction. Refractions were converted into vector notation. Logistic regression was used to evaluate whether spectacle dependence for near and distance was related to overall refractive error, spherical error, signed spherical error and astigmatic error.
Results: 169 patients attended for assessment. 38 wore distance glasses, and 160 wore reading glasses either some or all of the time. The mean right spherical equivalent was −0.03 D, and the mean right cylinder was −0.64 D. Left outcomes were similar. Patients were 34 times more likely to always use distance glasses per dioptre of astigmatic error in the better eye (p<0.003), but there was no significant increase in the likelihood of wearing distance glasses with spherical error (odds ratio = 3.85, p>0.15). Similar effects were seen for both the better and worse eyes. Near-spectacle use was not dependent on astigmatic error (odds ratio = 0.22, p>0.12). It was only related to the signed spherical error in the worse eye with hypermetropic patients 6.74 times more likely to always wear spectacles per dioptre of positive spherical error (p<0.005).
Conclusions: Following bilateral monofocal intraocular lens implantation, small levels of overall refractive error, in either eye, particularly astigmatism, predict distance-spectacle dependence, whereas spherical ammetropia in the range of ±1.0 D does not. Hypermetropia in the worse eye, but not astigmatism, predicts reading-spectacle dependence.
Statistics from Altmetric.com
The standard treatment for patients undergoing routine cataract surgery is to insert a monofocal or fixed focus intraocular lens (IOL). When inserting such an IOL we frequently select an IOL power that will leave the patient with an emmetropic or low myopic prescription. Following bilateral phacoemulsification surgery where emmetropia has been targeted, spectacle dependence for distance is at least 40%.12
What is not clear is what factors in the postoperative refraction predict whether a patient will be spectacle-dependent for near or distance. Knowledge of such factors would allow the surgeon, by changing the IOL power selected, or by managing preoperative astigmatism, to reduce spectacle dependence.
Methods
This study is an analysis of data collected from a study to examine vision-related quality of life after routine bilateral sequential phacoemulsification. Three hundred cataract patients were entered into a prospective study of visual outcomes after bilateral cataract surgery. Patients were randomised to sequential implantation with either the Tecnis Z9000 or the Acrysof MA60AC monofocal intraocular lenses. Computer-generated randomisation using a non-blocked coin-toss protocol was used to allocate patients to sequential bilateral implantation of the Z9000 IOL or MA60AC IOL. A spherical equivalent from 0 to −0.5 D was targeted in each eye. This study has been reported in detail elsewhere.3
Inclusion criteria were: age 30 years and above and presence of bilateral visually significant cataracts. Exclusion criteria were: ocular co-pathology which might influence postoperative vision, congenital cataracts or a history indicative of amblyopia and preoperative astigmatism greater than 1.5 D as measured by the IOLMaster keratometer. Wherever cataract density permitted, biometry was performed using the IOLMaster; otherwise A-scan biometry was performed. Manufacturers’ ultrasound A constants were used throughout. Information on the biometry technique used was retrospectively collected by examining the notes.
Four months after the second eye was operated on, patients were interviewed about whether they wore spectacles for near and distance visual tasks and underwent a subjective refraction. Patients were asked whether they wore distance-spectacles “always,” “for driving/TV only” or “never.” They were also asked if they wore reading glasses “always,” “for fine print only,” or “never.”
Binocular uncorrected visual acuity (UCVA) and binocular best spectacle corrected visual acuity (BSCVA) were tested using Early Treatment of Diabetic Retinopathy Study (ETDRS) log minimum angle of resolution (logMAR) letter charts projected on a high-resolution liquid crystal display 4 m from the subject. Refractions were performed by two trained ophthalmic technicians, using a precise protocol. The duochrome technique was not used. All refractions were recorded in minus cylinder format. Near acuities were not recorded, as the original primary aim of the study was to assess the effect of two IOL designs on distance vision-related quality of life.
Spherocylindrical powers were converted to a three-dimensional vector notation that included astigmatism and sphere powers (M, J0 and J45).4 The spherical error (M) refers to the spherical equivalent; J0 and J45 refer to Jackson crossed cylinders with orientations of 0 and 45° respectively. The values for M, J0 and J45 specify a point in space, and the distance of this point from the origin represents overall refractive error (D). The astigmatic error (J) is half the cylindrical power. Visual acuity has been shown to decline systematically as D increases, regardless of the proportions of sphere and cylinder contributing to the blur.5
Logistic regression was used to evaluate whether the questionnaire responses to spectacle dependence for near and distance were related to D, M and J. Normally, M, J and D are unsigned. For the logistic regression, we also used a signed version of M hypothesising that a sign would be important for reading-spectacle dependence. For each pair of eyes, one was labelled as “better” and the other as “worse.” For analysis of distance-spectacle use, the “better” eye was the one with the lower value of M. Where the M values were the same, the eye with the lower cylinder magnitude was labelled as better. For analysis of reading-spectacle use, the “better” eye was the one with the more myopic MRSE. A p value <0.01 was taken to be significant.
Results
Between May 2003 and October 2006, 300 patients underwent bilateral sequential cataract surgery; 179 patients attended for a refraction and assessment 4 months after their second eye was operated on. The low return rate was due to the trial population being recruited from a mobile, multiethnic population, and a large number of cases were unavailable or could not be contacted.
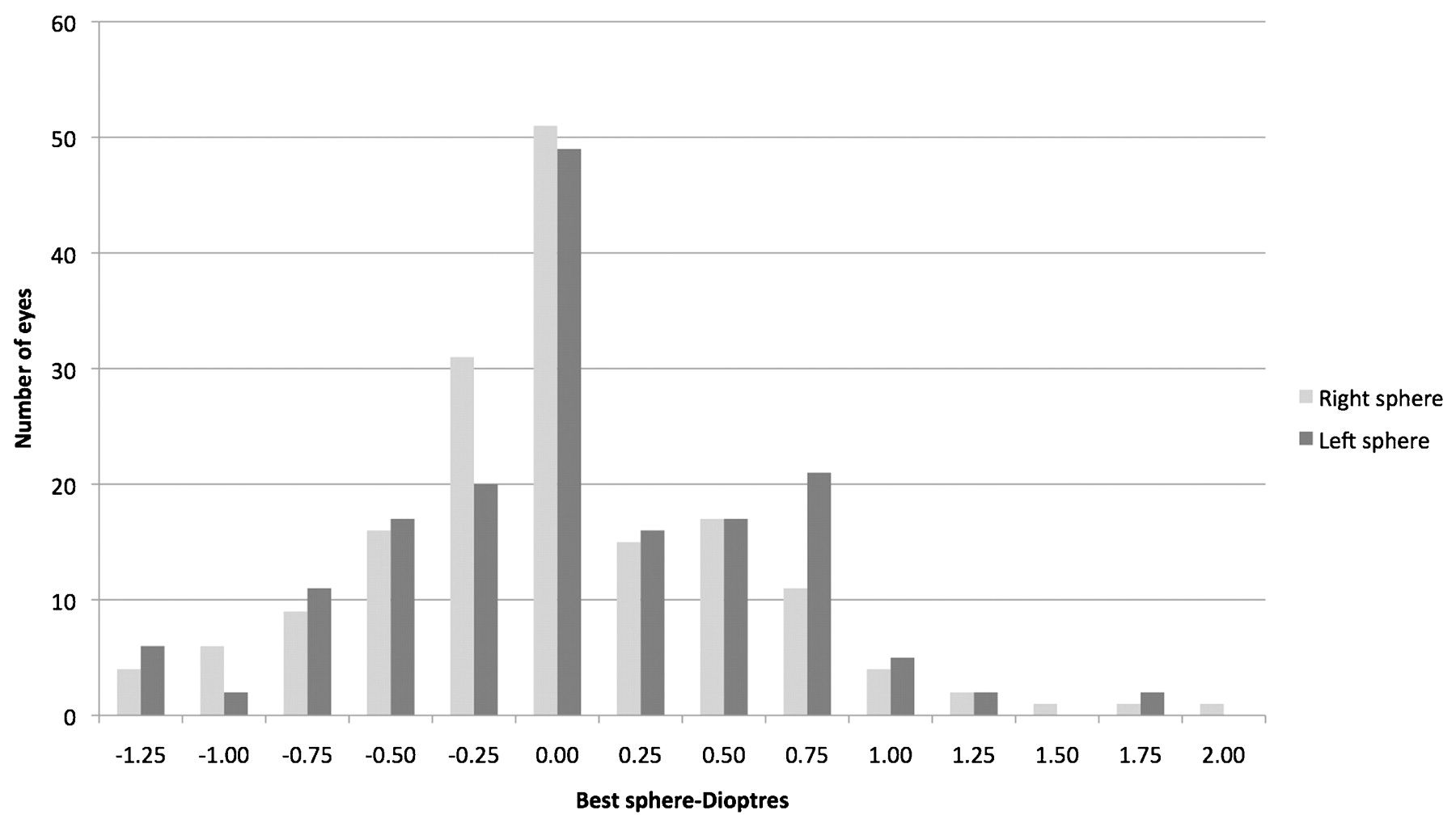
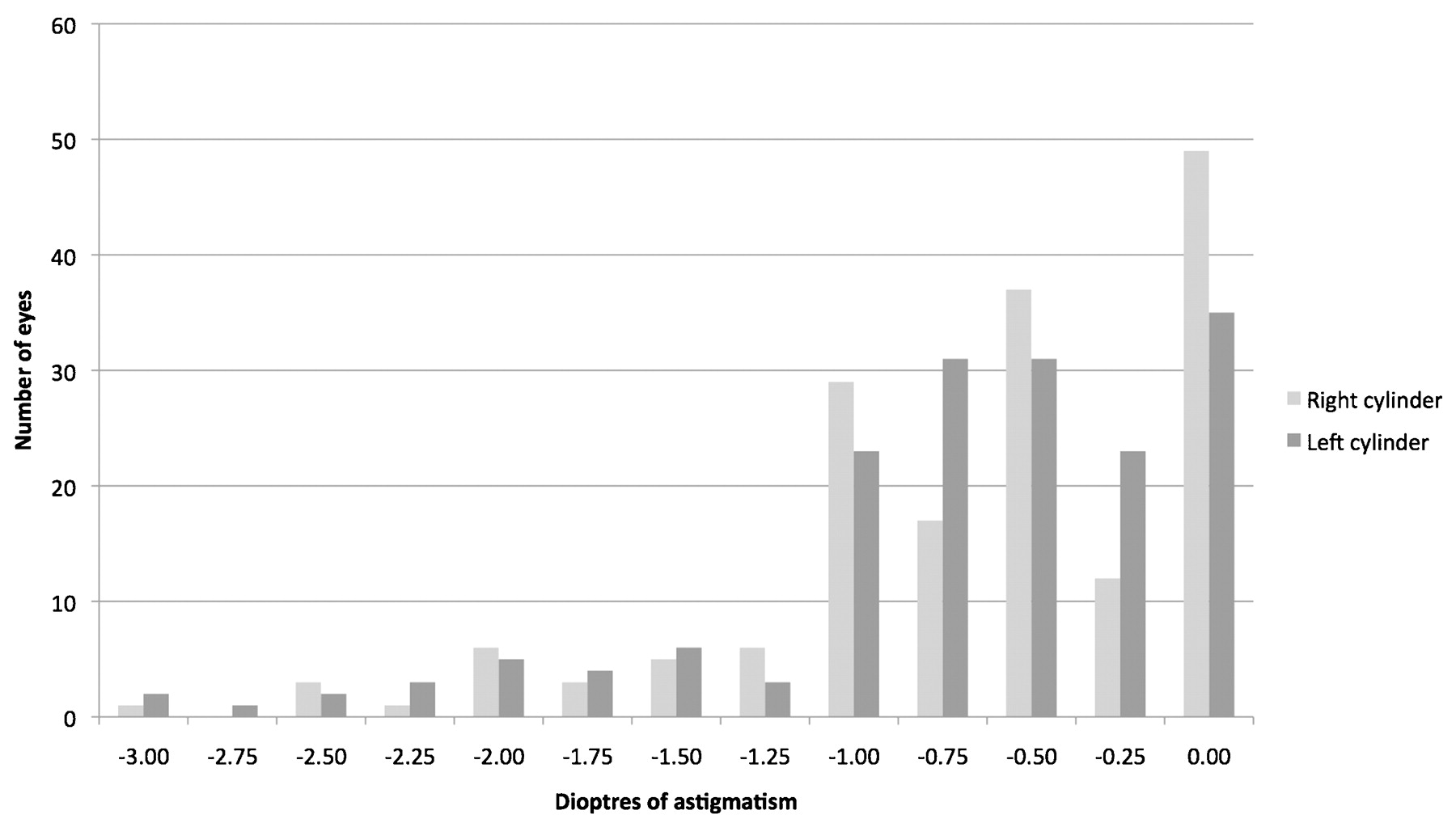
Refractive and questionnaire outcomes were available on 169 patients. The mean age of the patients was 70.7 years, 63 were male and 106 female. The mean postoperative refractive spherical equivalent in the right eye was −0.03 D (range +2.0 to −1.5 D, SD 0.55 D) and the mean right cylinder was −0.64 D (range 0 to −3.25 D, SD 0.63 D). In the left eye similar results were achieved; mean refractive spherical equivalent = 0.00 D (range +1.75 to −1.85 D, SD 0.57 D) and mean left cylinder = −0.70 D (range 0 to −3.0 D, SD 0.65 D). The best spheres were normally distributed (Shapiro Wilk test NS). Figures 1, 2 show the distribution of best sphere and manifest cylinder respectively for right and left eyes. Ninety-six patients received Acrysof, and 73 received TECNIS. Biometry in the right eye had been performed using the IOLMaster in 145, and A-scan in 17. Information on the biometry technique used was not retrospectively available for seven patients. The figures for the left eye were similar. The mean absolute difference in spherical equivalent between eyes was 0.34 D (SD 0.34 D).
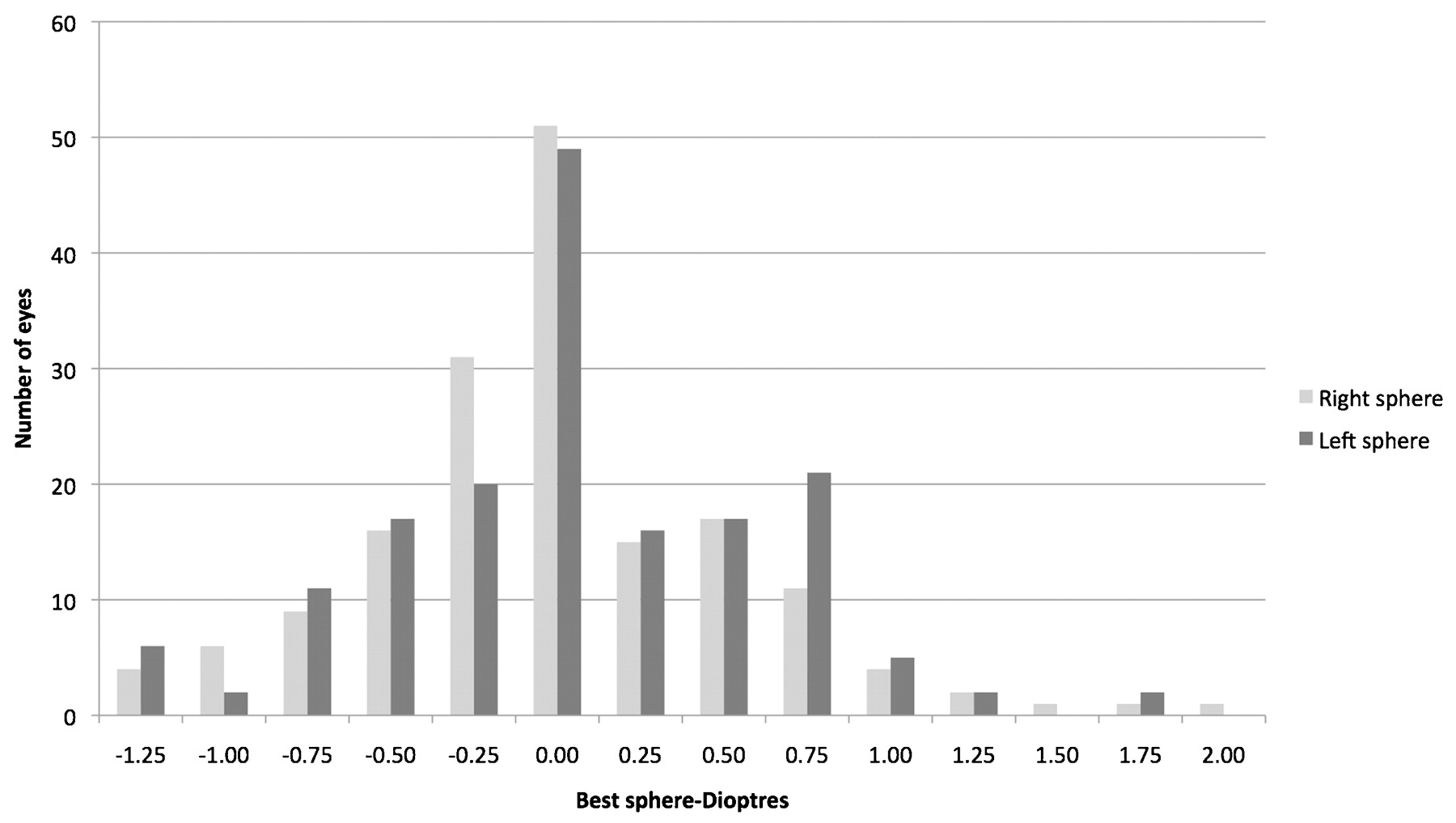
Distribution of best sphere (D) for right and left eyes.

Distribution of manifest cylinder (D) for right and left eyes.
Since the surgery, 103 patients had obtained new spectacles. Ten (5.9%) wore glasses with a distance prescription all the time, and 28 (16.6%) wore them some of the time. A total of 38 (22.5%) wore glasses either some or all of the time; 131 (73.1%) never used distance glasses; 113 (66.7%) patients always wore glasses for reading; 47 (27.8%) wore glasses for fine print only; and nine (5.3%) never wore glasses for reading. Table 1 shows the mean cylinder and spherical equivalents, and unaided and aided logMAR binocular acuities for the three categories of distance-spectacle use. Table 2 shows the mean cylinder and spherical equivalents, for the three categories of near-spectacle use. There was no significant difference in the percentage of patients reporting near or distance-spectacle use between Acrysof an TECNIS IOL recipients (χ2 test p>0.05).
Numbers of patient reporting that they wore glasses for distance tasks against mean spherical equivalent and cylinder, binocular logMAR uncorrected and best spectacle visual acuities
Numbers of patient reporting that they wore glasses for near tasks against mean spherical equivalent and cylinder
The odds ratios for wearing spectacles “all of the time versus never” and “some of the time versus never” per dioptre of overall refractive error, spherical error and astigmatic error are shown in table 3 (distance-spectacles) and table 4 (near-spectacles).
Odds ratios (for individual eyes) for likelihood of wearing distance-spectacles per dioptre of overall refractive error, spherical error and astigmatic error
Odds ratios (for individual eyes) for likelihood of wearing reading-spectacles per dioptre of overall refractive error, spherical error and astigmatic error
Patients with a greater overall refractive error (D) and greater astigmatic error (J) were much more likely to use glasses for distance. Within the range of refractions studied, astigmatic error had a much greater effect on the likelihood of spectacle use than overall error. In the better eye, a patient was 33.96 times more likely to always use glasses per dioptre of astigmatic error compared with only 9.53 times more likely per dioptre of overall refractive error. Spherical error (M) was not predictive of distance-spectacle use, and the sign of M (myopic vs hypermetropic) was not relevant. These effects were seen for both the better and worse eyes, although the effect was less for the worse eye. Although refractive error in the “better” and “worse” eyes predicted distance-spectacle use when separate models were fitted for the two eyes, the “worse” eye no longer predicted distance-spectacle use when both eyes were put into a single model.
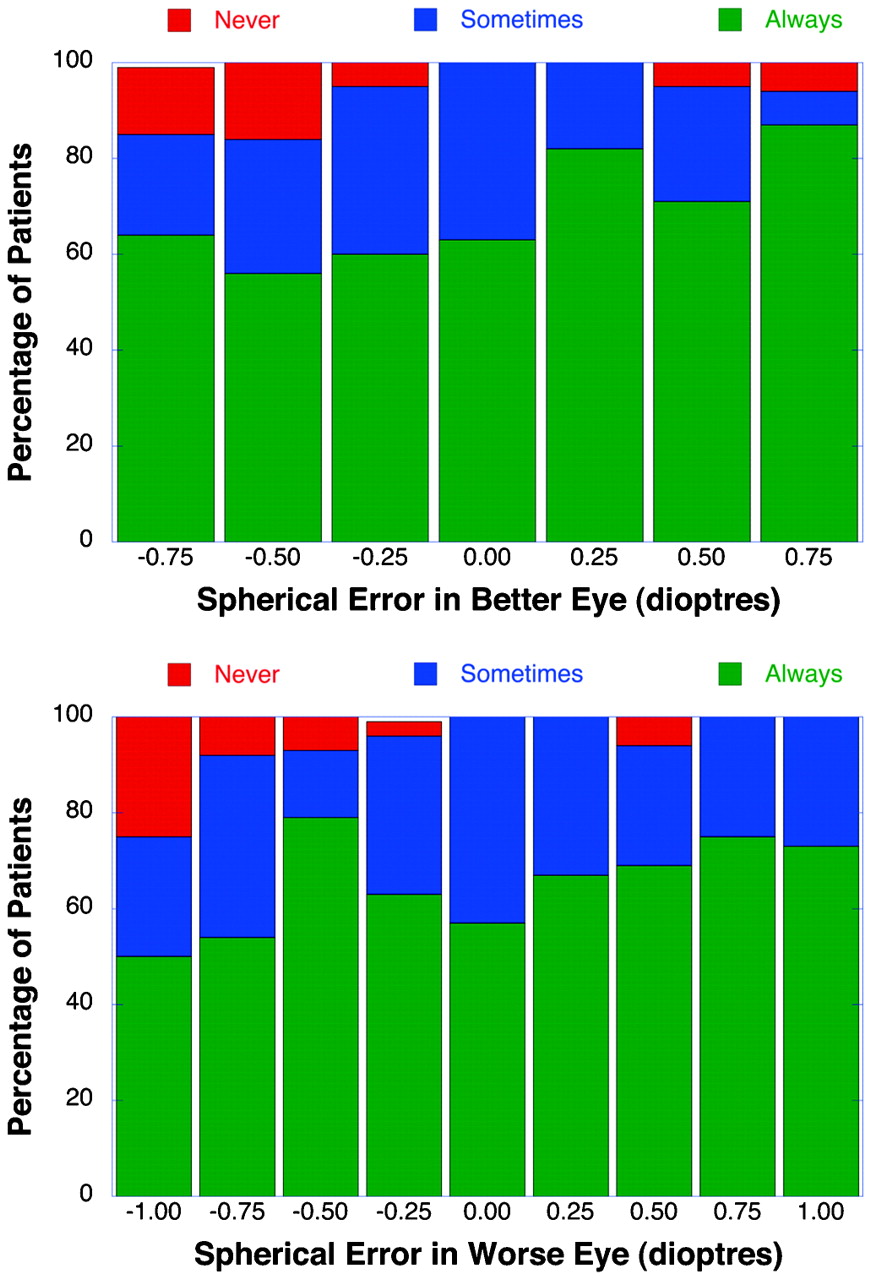
For near-spectacle use, unlike for distance, spectacle use was not dependent on overall refractive error (D) or on astigmatic error (J). It was only related to the sign of the spherical error (M) in the “worse” eye. A patient was 6.74 times more likely to use near-spectacles all of the time per dioptre of positive residual sphere. This effect is shown in mosaic plots of the regression analysis (figs 3, 4). The plots show the percentage of patients who use spectacles for either distance or near vision as a function of astigmatic error (J) or spherical error (M).

Percentage of patients who use spectacles for distance vision as a function of astigmatic error (J) in better eyes (top panel) and worse eyes (bottom panel).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of patients who use spectacles for near vision as a function of spherical error (M) in better eyes (top panel) and worse eyes (bottom panel).
The mean difference in spherical error between eyes was low at 0.34 D. The difference in spherical error (M) between eyes was not a significant predictor of near or distance-spectacle use (p>0.5). Unplanned monovision thus had no significant effect on near-spectacle use.
Discussion
Reducing spectacle dependence is a common aim for cataract surgeons. Very little evidence exists about how spectacle independent patients are for distance tasks when emmetropia is targeted. There are two studies where spectacle dependence after bilateral monofocal IOLs has been described.16 Javitt et al reported that 40% of patients targeted to receive emmetropia/very low myopia were dependent on spectacles for distant use.1 In a second study comparing bilateral multifocal with monofocal IOL implantation, Nijkamp showed that between 42 and 60% of monofocal patients reported always using distance glasses; the figure varied depending on the time point after the surgery.2 If emmetropia is targeted, most surgeons would assume that their patient would be dependent on reading glasses for near tasks. The same two studies found that 4–11% of patients were not dependent on reading glasses when emmetropia was targeted with monofocal IOLs.12 Nijkamps’s figure varied between 4 and 6.2% depending on the time postop.2 A third study reported that no patients receiving monofocal lenses were independent of glasses for all reading tasks.6
In this study, we have shown that distance-spectacle dependence after bilateral cataract surgery with a mean achieved spherical equivalent of 0 D is 22.5%, while near-spectacle dependence is 95.7%. Furthermore, the components of the refraction did not equally predict spectacle use. The odds of using distance glasses were 9.53 times greater for every dioptre of overall refractive error in the “better” eye, and 33.96 greater for each dioptre of astigmatic error in the “better” eye. Postoperative spherical error (M) had no predictive effect on the use of distance-spectacles. Overall refractive error in the “worse” eye did not predict distance-spectacle use when “better” and “worse” eyes were put into a single model.
For near-spectacles overall refractive error, spherical error, and astigmatic error did not predict near-spectacle use, while only signed spherical error in the worse eye did. The more hypermetropic the spherical error in the “worse” eye, the more likely the patient was to report wearing reading glasses. We were unable to demonstrate a monovision effect. Signed spherical error in the “better” (more myopic) eye did not predict near-spectacle use, nor did the difference in spherical equivalent between eyes predict their use. However, the mean absolute difference in spherical equivalent was small, 0.34 D; it may well be that the amount of monovision achieved was too small for an effect to be seen.
Some work has suggested that patients who end up with low myopia combined with some astigmatism after cataract surgery achieve “good” unaided near and distance acuity.78 Both studies looked at eyes rather than patients, and neither assessed the spectacle dependence of patients.78
Although targeting low myopia with some myopic astigmatism does confer some unaided distance and unaided near acuity, it may well be that static reading tasks such as the near test type do not really reflect real-world situations.9 Phakic presbyopes fitted with contact lenses to give them either low spherical myopia (−0.5 D) or myopic astigmatism (plano/−1.0 D) have better intermediate distance acuity and refractive quality of life with spherical myopia rather than with myopic astigmatism, and there is no difference in distance and near acuities.10 Studies analysing the effect of postcataract surgery low myopia and astigmatism have used an acuity ⩾6/12 to select patients with relatively good unaided acuity.78 Patients close to 6/12 unaided in each eye might have trouble meeting the minimal legal requirement to drive in the UK, which approximates to 6/10.11 Equally for near tasks, variables such as maximum reading speed and critical print size may be more relevant. We have no information from the same studies about such variables.
Our use of the manufacturer’s A constants rather than those optimised for the IOLmaster meant that our mean spherical equivalent was 0 D rather than between 0 and −0.5 D as targeted. The trial was started before this issue was widely known. The standard deviation was 0.55 D in the right eye and 0.57 D in the left. Thus, 95% of eyes had a spherical equivalent ±1.0 D of emmetropia. This has allowed us to assess the effect of spherical equivalent for low hypermetropic and myopic outcomes. Previous studies have found a near-spectacle independence rate of 0–11%.126 Our figure of 5.3% falls in the middle of this range. We found that near-spectacle use was significantly associated with signed spherical error. The association between spherical equivalent and near-spectacle independence in this and the other three studies is shown in table 5.
Near-spectacle independence and spherical equivalent in four studies where monofocal implants were implanted bilaterally
The current interest in multifocal IOLs has heightened interest in achieving spectacle independence for near and distance tasks. Studies have highlighted the impact of astigmatism on the visual acuity in patients receiving multifocals.1213 Distance and intermediate acuities suffer greater impairment from astigmatism than monofocal IOLs.12 It is thus likely that distance-spectacle dependence would be more sensitive to astigmatism in patients implanted with multifocals.
This study suggests that astigmatism needs to be corrected if distance-spectacle dependence with monofocal IOLs is to be as low as possible. Even where multifocals are not being inserted accurately, counselling and consenting patients prior to surgery is essential. Where a patient has astigmatism preoperatively, they should be made aware of the chances of wearing glasses for distance tasks postoperatively or advised on available measures to reduce the astigmatism. Making one eye slightly myopic could also reduce near-spectacle dependence.
The Blue Mountains study shows that 13% of patients have astigmatism over 1.5 D.14 Furthermore, the prevalence of astigmatism increases with age.14 The mean cylinder was −0.6 D in persons aged 49–59 years and rose to −1.2 D in those aged 80–97 years. Knowledge of the impact of astigmatism on distance-spectacle dependence is therefore crucial for ophthalmologists performing cataract surgery, since the prevalence of cataracts and astigmatism both increase with age.15
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
The Moorfields IOL Study Group: Study design: B Allan, C Bunce, F Fitzke, G Rubin. Recruiting surgeons: W Abdullah, B Allan, D Gartry, A Ionides, V Maurino, S Tuft, M Wilkins, R Wormald. Trial coordinator: N Dudley. Visual assessment technicians: K Bibi, E White. Data entry: W Xing, N Harris, S Mann. Data analysis: C Bunce, G Rubin, S Mann, W Xing, M Wilkins.