Article Text

Abstract
Relative scotopic spectral sensitivity depends only on the rhodopsin photopigment and ocular media absorption spectra. Rhodopsin is well characterised so the relative scotopic spectral sensitivity function can be calculated for intraocular lenses (IOLs) of known spectral density. In a recent perspective, Mainster and Sparrow concluded that an IOL with short wave absorbing chromophores would provide more retinal protection than conventional IOLs, but the practical consequences for scotopic vision are unclear. This paper uses published experiments to examine the implications for scotopic vision of the IOLs analysed by Mainster and Sparrow. A 14.6% reduction in scotopic sensitivity is expected for a SN60AT (AcrySof Natural) compared to a SA60AT (Conventional AcrySof) IOL under broadband illumination (equal quantum spectrum). This effect (0.07 log unit) is visually insignificant in relation to the ∼4.0 log unit range of scotopic sensitivity. More importantly, it is expected that scotopic contrast sensitivity would be reduced by only ∼0.01 log unit. It is thus improbable that a difference in scotopic vision between observers with the Natural and Conventional IOLs could be reliably detected using broadband stimuli.
- CSF, contrast sensitivity function
- IOL, intraocular lens
- night vision
- ageing
- contrast sensitivity
- intraocular lens
- scotopic vision
- CSF, contrast sensitivity function
- IOL, intraocular lens
- night vision
- ageing
- contrast sensitivity
- intraocular lens
- scotopic vision
Statistics from Altmetric.com
- CSF, contrast sensitivity function
- IOL, intraocular lens
- night vision
- ageing
- contrast sensitivity
- intraocular lens
- scotopic vision
- CSF, contrast sensitivity function
- IOL, intraocular lens
- night vision
- ageing
- contrast sensitivity
- intraocular lens
- scotopic vision
Scotopic vision refers to vision in darkness, and its importance for human behaviour has often been overlooked by practising ophthalmologists. Expressed in terms of measured light levels, the scotopic range is below a luminance level of about −3.8 log cd m−2. It encompasses the stimulus range from absolute threshold (fewer than 100 quanta delivered to the cornea under ideal conditions) to a retinal illuminance of ∼0.3 photopic trolands, which is about the maximum light level encountered at night under natural conditions.1 Thus, scotopic vision spans approximately 4 log units of ambient illumination. Scotopic vision is mediated by a single class of photoreceptors, the rods. Scotopic vision is not, however, synonymous with rod vision because rods and cones overlap in their range of sensitivity by about 3 log units, the range known as mesopic vision.
The importance of intraocular lens (IOL) absorption spectra on scotopic vision was recently discussed by Mainster and Sparrow.2 They noted that chromophores that may be useful in protecting the retina from the “blue light” hazard also absorb near the scotopic spectral sensitivity maximum. Their analyses considered the percentage change in sensitivity. Here, we shall consider the same issue, but illustrated more traditionally in logarithmic units so that the losses can be seen in the context of the full range of scotopic sensitivity. It will be shown why IOL absorption of light at wavelengths near the sensitivity maximum is no more important for scotopic vision than absorption at any other wavelengths. We shall also consider some aspects of scotopic vision not discussed by Mainster and Sparrow. In particular, the consequences of IOL absorption spectra are evaluated in terms of scotopic spatial contrast sensitivity as a quantitative index of pattern, or form, vision.
SCOTOPIC SPECTRAL SENSITIVITY WITH AN IOL CONTAINING CHROMOPHORES ABSORBING SELECTIVELY AT SHORT WAVELENGTHS
The absorption spectrum of an IOL can be used to calculate the relative spectral sensitivity for scotopic vision because the rods contain only one type of photopigment, rhodopsin, and scotopic sensitivity depends only on the number of quanta absorbed by the photopigment. While some wavelengths are more likely to be absorbed than others because of the chromophores in the photopigment and preretinal filtering (primarily by the lens), once absorbed, all wavelengths produce the same effects. Rushton3 calls this the principle of univariance. This principle has important implications for evaluating the effect of IOL absorption spectra. Both photochemical hazards and scotopic sensitivity depend upon absorbed photons and the probability of absorption is wavelength dependent. Considered in terms of absorbed photons, photochemical hazards are wavelength dependent, but scotopic vision is not. Put another way, IOL absorption at short wavelengths is no more consequential for scotopic vision than absorption at middle or long wavelengths.
The crystalline lens, or an IOL, will necessarily cause a decrease in sensitivity (increase threshold) by an amount equivalent to its spectral absorption. Thus, when rhodopsin density (a logarithmic scale) is compared with log spectral sensitivity of an aphakic observer, the two curves are essentially identical with a small correction for the spectral density of the cornea.4 This principle has been demonstrated for the scotopic spectral sensitivity functions of phakic5 and pseudophakic6 observers. Figure 1 utilises this principle to compare the expected scotopic spectral sensitivity function for observers with the SN60AT (AcrySof Natural) and SA60AT (Conventional AcrySof) IOLs. The optical densities (−log transmission) of the IOLs were provided by the manufacturer based upon measurements in saline solution. This results in somewhat different values from that in the analysis by Mainster and Sparrow who used the data of Lin et al7 for the conventional IOL (measured in saline) and transmission values from the manufacturer for the natural IOL (measured in air). The two conditions of measurement differ in Fresnel reflection losses, which result in different transmission values. For this reason, our analyses are based on measurements of both IOL types under identical conditions (immersed in balanced salt solution).
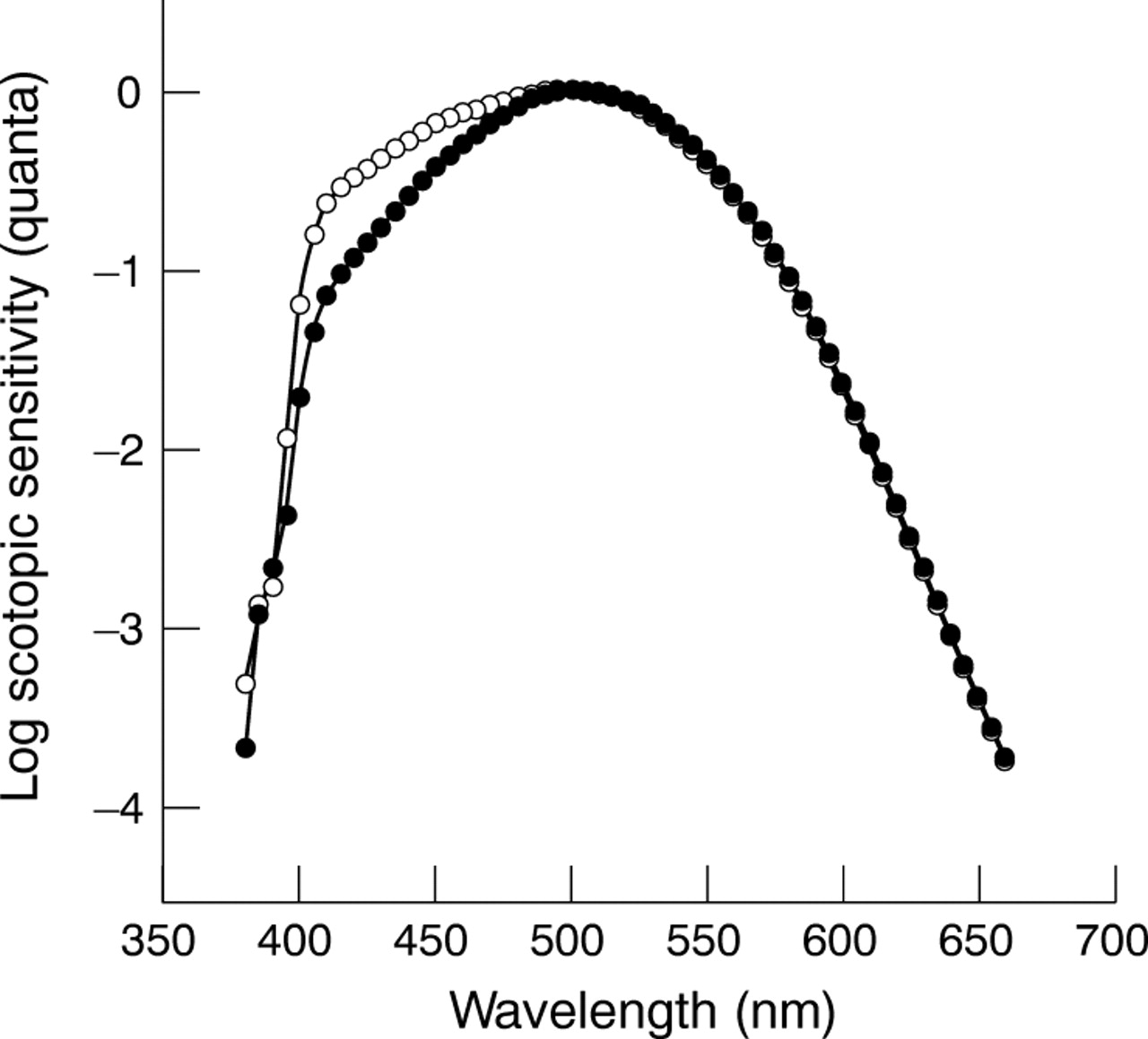
Calculated log scotopic sensitivity plotted in terms of quanta delivered to the cornea as a function of wavelength. Calculations are based on a rhodopsin nomogram and 20 D IOLs. Open symbols, Conventional (Alcon SA60AT) and solid symbols, Natural (Alcon SN60AT).
The curves presented in figure 1 are consistent with analyses by Mainster and Sparrow2; however, the figure uses conventional logarithmic ordinates to place the effect on scotopic sensitivity in perspective. Relative to the range of scotopic sensitivity, the greater density of the AcrySof Natural IOL for wavelengths between 400 nm and 50 nm would seem to be trivial for natural (broadband) illuminants when integrated across the visible spectrum. Such an integration is appropriate because this is what the rods do—count absorbed photons independent of wavelength. Indeed, the effect is small even for most narrow band sources. The consequences of IOL density differences will be further considered in terms of spatial vision in a separate section.
AGEING AND SCOTOPIC SENSITIVITY
The previous section considered the consequences of IOL absorption for the relative scotopic spectral sensitivity function. The position of the curve along the ordinates, absolute sensitivity, is known to vary with age. This was first demonstrated by examination of the asymptotes of dark adaptation functions which show an elevation of the rod branch as an increasing function of age.8 This latter result has been confirmed by more recent studies.9,10 It was not clear from some of the early studies whether these effects were entirely due to age related changes in retinal illuminance caused by smaller pupils and more dense lenses.
Most recent studies, but not all,11 that have taken age related changes in pupil size and ocular media density into account have demonstrated age related losses in scotopic sensitivity.12,13 For example, Schefrin et al13 measured thresholds in Maxwellian view so that all light entered the eye through a 1.5 mm exit pupil conjugate with the eye pupil. This effectively bypasses any age related variation as a result of pupillary miosis. Following 30 minutes of dark adaptation, sensitivity was measured for 10 ms, 520 nm circular test lights of varying diameters that were superimposed and concentric with a 10°, 640 nm circular background. This background was selected to suppress cone sensitivity with no influence on rod sensitivity. The test lights were imaged along the horizontal meridian, 6° nasal from a foveal fixation point. Figure 2 shows results for one stimulus diameter; essentially the same results were obtained for other diameters. The solid line is based on the linear regression equation fitted to the raw data representing stimuli delivered to the cornea. The broken line is from the regression equation obtained after correcting the data to specify sensitivity at the retina—that is, corrected for age related changes in the ocular media.14 This is what would be expected in a population of aphakes or pseudophakes with a conventional IOL.4,6 Although much of the loss in scotopic sensitivity is the result of the ocular media density, it is clear from these results that age related losses in scotopic sensitivity cannot be explained solely by preretinal change.

Scotopic sensitivity plotted as a function of age. Symbols represent thresholds for test lights of 0.04 degree diameter, 10 ms flashes, 520 nm presented at 6 degrees nasal along the horizontal meridian. The solid line represents the linear regression fitted to these points. The broken line represents the linear regression obtained when the data are corrected for ocular media density and sensitivity is specified at the retina. The dotted line shows the loss in sensitivity expected from an equal quantum spectrum filtered by an AcrySof Natural IOL.
A variety of studies suggest that changes at the receptor level may partially account for these age related losses in scotopic sensitivity. In vivo measurements of the photopigment kinetics indicate that a change in the rate of dark adaptation is the result, at least in part, of a slowing of photopigment regeneration.9,15 Other changes at the receptoral level involve the relative ability of “ageing” rods to capture light quanta efficiently. Although there are substantial losses in numbers of rod photoreceptors with age,16 the amount of rhodopsin photopigment in the retina decreases only slightly, if at all, with increasing age.17 This implies that individual surviving rods must contain more photopigment in the older retina. However, some outer segments of these aged photoreceptors undergo morphological changes such that they appear to be more convoluted in shape.18 These relatively deformed outer segments may contribute to reductions in scotopic sensitivity because rhodopsin molecules now possess less than optimal orientations for absorbing light.
It has been proposed that rods are more susceptible to ageing than cones.19 This is consistent with histology showing greater losses in rod numbers than cones in the ageing retina.16 However, the rod system may compensate to some extent for losses in photoreceptor number. For example, surviving rods become larger when neighbouring rods are lost and this may compensate, in part, the quantal catch losses from smaller rod numbers. We13 have shown that the integration area for scotopic vision (that is, the retinal area over which the product of intensity and area is constant, Ricco’s area) enlarges by about 15% per decade throughout the adult years. As a result, the rate of ageing depends not only on stimulus wavelength (when sensitivity is specified at the cornea), but size and duration of test flashes. While it is certain that there are age related losses in scotopic sensitivity, it is uncertain how this compares with age related losses in photopic sensitivity.
In summary, losses in scotopic sensitivity with age are partly the result of age related changes in retinal illuminance caused by decreased pupil diameter and increased ocular media density. When these factors are controlled, however, significant age related losses in scotopic sensitivity remain.12,13 What are the consequences for age related loss in scotopic sensitivity expected from an AcrySof Natural IOL? This is shown by the broken line in figure 2 computed for an equal quantum spectrum. The shift in the curve from that with a conventional IOL is 0.07 log unit for an equal quantum spectrum; it would be greater for lights with more short wave energy such as halogen lights20 and this may be useful for reducing the effects of glare from oncoming car headlights, a significant problem for elderly drivers.21–23 The age related loss would be less for tungsten illumination because the emission spectrum for tungsten is dominated by middle and long wavelengths. Overall, the losses in scotopic sensitivity associated with an AcrySof Natural IOL are inconsequential for conditions of natural illumination.
SCOTOPIC SPATIAL VISION WITH AN SN60AT IOL
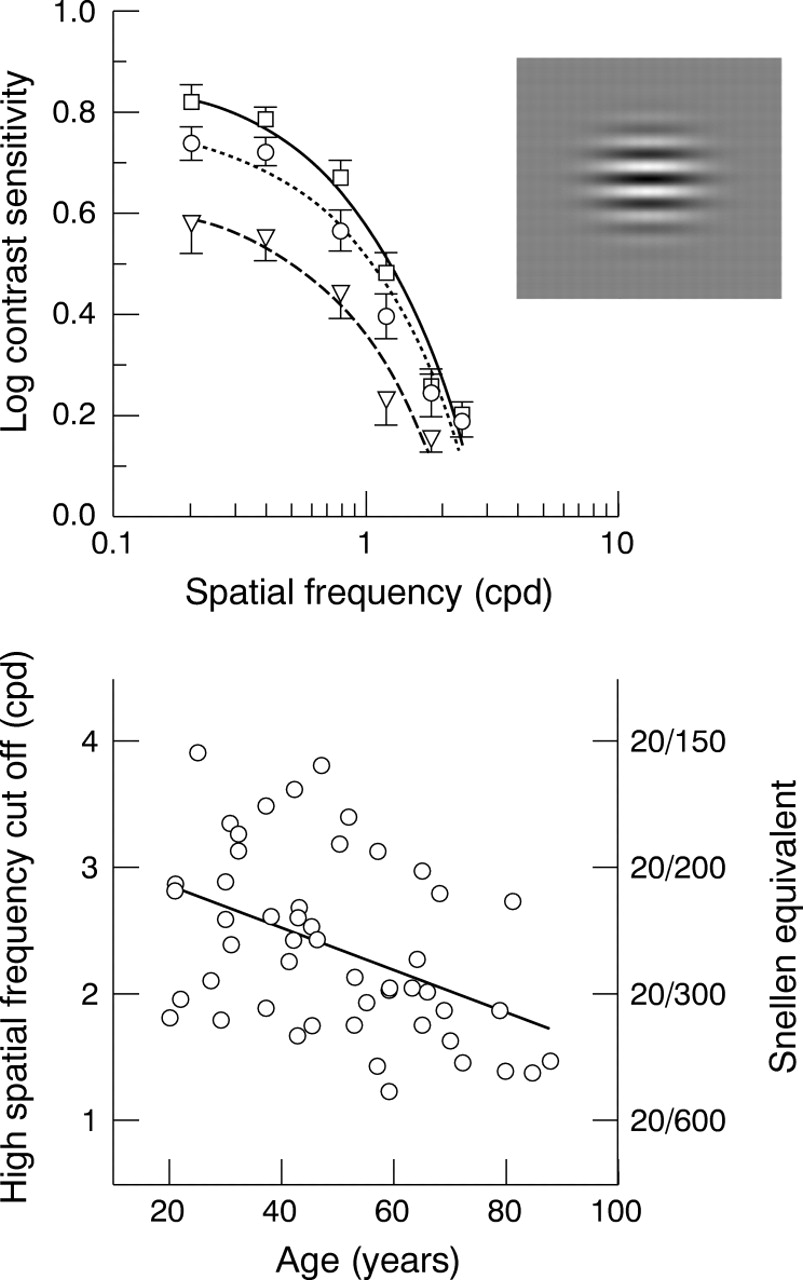
Visual acuity, the minimum angle of resolution, is the most common measure of spatial (form) vision. It is usually measured with eye charts containing letters of various sizes. The resolution limit can also be obtained from a more general measure of spatial vision called the contrast sensitivity function (CSF). Only a few studies have measured contrast sensitivity under scotopic conditions. In our laboratory, scotopic CSFs were measured for 50 observers between the ages of 20 years and 88 years.24 Using a maximum likelihood, two alternative, temporal forced choice threshold estimation algorithm, scotopic CSFs were measured at seven spatial frequencies ranging from 0.2–3.0 cycles per degree (cpd), with mean retinal illuminance equated for observers at −0.85 log scotopic trolands. For each stimulus condition, eight cycles of a horizontal sinusoidal grating25 were presented within plus or minus 1 SD of a two dimensional Gaussian spatial envelope and within a 1 second Gaussian temporal envelope. (This, so called Gabor patch, is illustrated by the inset in the upper panel of fig 3.) Stimuli were centred on the nasal retina along the horizontal meridian 6° from the fovea.

Upper panel shows mean scotopic contrast sensitivity functions for observers of three different age groups. The squares, circles, and triangles represent average sensitivities for subjects aged 20–40, 41–60, and 61–88 years, respectively. Error bars denote 1 SEM. The inset to the right shows a Gabor patch (sine wave with a Gaussian taper). Lower panel shows the high spatial frequency cut off (cpd) or resolution limit (Snellen equivalent) under scotopic conditions plotted as a function of age. (From Schefrin et al24.)
The CSF represents the reciprocal of the minimum contrast required to detect sinusoidal gratings that vary in spatial frequency (the number of cycles per degree of visual angle, cpd). As shown in the top panel of figure 3, scotopic CSFs were found to be low pass for all age groups. Statistically significant age related declines in contrast sensitivities were found for spatial frequencies at or below 1.2 cpd. This greater loss in contrast sensitivity at low spatial frequencies is quite different from photopic contrast sensitivity changes with age in which the decline in sensitivity is only at higher spatial frequencies for luminance varying stimuli.26,27 An analysis of these results in terms of optical factors could be rejected, while the results are consistent with age related changes in scotopic neural pathways.
The bottom panel of figure 3 shows the highest spatial frequency (the CSF “cut-off” frequency) that can be detected under scotopic conditions as a function of age. The axis on the right shows the equivalent visual acuity using the more familiar Snellen notation. It is apparent that our ability to see fine detail is substantially less under scotopic compared to photopic vision, and it declines as a function of observer age.
While age related losses in scotopic contrast sensitivity are largely of neural origin for the phakic observer, the question remains whether IOLs with different chromophores might influence the scotopic CSF. These effects can be calculated using data from the literature in which scotopic contrast sensitivity is measured as a function of retinal illuminance.
It has been shown that contrast sensitivity to a wide range of spatial frequencies under photopic conditions28 and to low spatial frequencies under mesopic29 and scotopic conditions30 increases monotonically with mean luminance level and then remains essentially constant. The range of luminance levels over which contrast sensitivity is constant is an example of Weber-like behaviour and is the result of contrast gain control mechanisms in the visual pathways.31 When photon flux reaches a critical level, scotopic vision depends only on contrast, not ambient light level.
Figure 4 illustrates mean illuminance dependent changes in scotopic sensitivity for nine observers having a mean age of 75 years.32 These data are from a larger study of 50 observers tested at 0.3 and 1.2 cpd after 30 minutes of dark adaptation. The stimuli were essentially the same as those used to obtain the data shown in figure 3, but the illuminance level was varied from absolute threshold to the Weber line where contrast sensitivity does not change with increases in retinal illuminance. Relevant to the analysis of IOLs was an analysis of the respective slopes of the ascending limbs of the contrast sensitivity versus retinal illuminance functions as shown in figure 4. For all but one observer, the slope associated with the 1.2 cpd grating data was steeper than the slope calculated for 0.3 cpd data. Therefore, 1.2 cpd is a “worst case” for determining contrast sensitivity losses with reductions in light level. Based upon a 14.6% transmission difference between SN60AT (AcrySof Natural) and SA60AT (Conventional AcrySof) IOLs, the loss in contrast sensitivity is calculated to be only 0.01 log units (1.2 cpd), an amount smaller than the data points in figure 4. This difference in IOL density is insignificant for scotopic contrast sensitivity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean log contrast sensitivity (1.2 cpd) for older observers (mean age, 75 years) plotted as a function of log retinal illuminance. Error bars represent 1 SEM. (Data from Schefrin et al32.)
CONCLUDING COMMENT
This report compares the consequences for scotopic vision for two different IOLs, SN60AT (AcrySof Natural) and SA60AT (Conventional AcrySof) IOLs chosen because the effect on scotopic vision was questioned by Mainster and Sparrow.2 The consequences for IOLs with other short wave absorbing filters may be different for photopic and scotopic vision, but sufficient data to estimate consequences of these IOLs on age related changes in scotopic vision are available in the literature. I have not considered the benefits of an IOL with short wave absorbing chromophores in terms of elevating the threshold for photochemical damage, a topic of long interest in our laboratory33,34 and thoroughly summarised by Mainster and Sparrow. This benefit is important whereas the loss in scotopic sensitivity is not, even considering that any losses would be added to normal age related changes caused by neural factors. The consequences for scotopic spectral sensitivity involve a reduction of only 0.07 log unit at absolute threshold. This is inconsequential compared with the range of scotopic sensitivity. More relevant to everyday visual performance is a loss of only 0.01 log unit in contrast sensitivity under the worst case. This is visually insignificant and given the measurement error in psychophysical experiments with naive observers under scotopic conditions, it is unlikely that a difference between the Natural and Conventional IOLs could be reliably detected with normal sampling using broadband illuminants.
REFERENCES
Footnotes
-
Experimental studies described in this paper were supported by National Institutes of Health (NIA grant AG04058) and a Jules and Doris Stein Research to Prevent Blindness Professorship. The author gratefully acknowledges Mutlu Karakelle for providing Alcon IOL absorption spectra.
-
The author has no financial interests in the products described in this paper.