Article Text

Abstract
BACKGROUND/AIMS Amblyopia in people with Down’s syndrome has not been well investigated. This study was designed to determine the prevalence and associated conditions of amblyopia in a group of home reared children with Down’s syndrome.
METHODS All children in the study group underwent an evaluation of visual acuity. In addition, previous ophthalmological records were reviewed, and a subgroup of children was examined. For the purposes of this study, amblyopia was defined quantitatively as a difference of two Snellen acuity lines between eyes or if unilateral central steady maintained (CSM) vision and a clear fixation preference was observed. A high refractive error was defined as a spherical equivalent more than 3 dioptres and astigmatism more than 1.75 dioptres. Anisometropia was defined as a difference of at least 1.5 dioptres of sphere and/or 1.0 dioptre of cylinder between eyes. 68 children with Down’s syndrome between the ages of 5 and 19 years were enrolled in the final study group.
RESULTS Amblyopia was observed in 15 (22%) of 68 patients. An additional 16 (24%) patients had bilateral vision less than 20/50. Strabismus, high refractive errors, and anisometropia were the conditions most commonly associated with decreased vision and amblyopia
CONCLUSION This study suggests that the prevalence of amblyopia is higher than previously reported. Fully 46% of these children with Down’s syndrome had evidence of substantial visual deficits. These patients may be at higher risk for visual impairment and should be carefully examined for ophthalmological problems.
- Down’s syndrome
- amblyopia
- visual acuity
- children
Statistics from Altmetric.com
Increased attention to various ocular abnormalities in people with Down’s syndrome is evident in the literature. Lid abnormalities, iris nodules, cataracts, keratoconus, spoke-like disc vessels, strabismus, nystagmus, and high refractive errors are reported in patients with Down’s syndrome.1-3 However, amblyopia in children with Down’s syndrome has not been well investigated. There are only two reports in the medical literature that make reference to amblyopia in institutionalised people with Down’s syndrome.3 4
This study was designed to determine the prevalence and associated ocular conditions of amblyopia in an unselected group of home reared children with Down’s syndrome.
Materials and methods
Children with Down’s syndrome enrolled in this study were recruited from the child development centre of Rhode Island Hospital. This centre is the only facility that provides comprehensive care for the majority of children with Down’s syndrome in the state and is closely aligned with the two cytogenetic laboratories in Rhode Island. Therefore, almost complete ascertainment of children with Down’s syndrome in Rhode Island is possible, and there is no known selection bias.
From this group of children with trisomy 21, we contacted 106 families who have a child with Down’s syndrome between the ages of 5 and 19 years. All the children are cared for at home. Of the 106 families contacted, 73 responded and agreed to participate in the study. The majority of the other 33 families had moved out of state, and others either failed to respond or refused to participate in the study.
After informed consent was obtained the 73 children (average age 10.6 years) were invited to the child development centre. These children underwent a visual screening examination which included best corrected, full line near and distance acuities tested with Snellen letters, numbers, or Allen pictures. General observations concerning cooperation and fixation preferences were recorded. Subsequently, we obtained information of best corrected, full line visual acuity, cycloplegic refractions, and a complete list of ophthalmological diagnoses from previous ocular examinations for the children in the study group.
A subgroup of 19 children, who had vision less than 20/50 in both eyes or if previous ocular records were incomplete, underwent a full ophthalmological examination at the Rhode Island Hospital Department of Ophthalmology. This ophthalmological examination included best corrected visual acuity testing with full line Snellen optotypes, Allen pictures, or evaluation of central, steady, and maintained (CSM) visual behaviour and fixation preference in those children who were non-verbal or severely mentally retarded. Examinations of ocular adnexa, ocular motility and strabismus, slit lamp examination, cycloplegic refractions, and dilated ophthalmoscopy were also performed. These examinations were carried out by one of the participating ophthalmologists, (CK, WT, RC). Five families declined this examination and were excluded from the study. Thus, the final study sample included 68 patients with Down’s syndrome.
Results
The visual acuity results for the 68 children with Down’s syndrome are listed in Table 1. It is of note that 10 patients (15%) had CSM vision and only five patients (7%) had 20/25 vision. The largest group of patients had vision in the 20/30 to 20/40 range. Importantly, a significant number of patients (31%) had less than 20/50 vision in the better eye (7%) or in both eyes (24%). The aetiologies associated with this finding were strabismus in three children, nystagmus in one child, anisometropia in two children, and high refractive errors in six children. In five patients, no aetiology was found to explain their decreased visual acuities. A mixed aetiology of poor vision was noted to be a high refractive error associated with nystagmus or strabismus.
Visual acuity in 68 children with Down’s syndrome
Amblyopia was observed in 15 (22%) of 68 patients. Of these 15 amblyopic children, eight had amblyopia associated with strabismus, five with anisometropia, and two with a mixed strabismic and refractive (anisometropic) aetiology. Of these 15 amblyopic patients, five had vision worse than 20/50 in the better eye; two of whom had a refractive (anisometropic) aetiology, one had a strabismic cause, and two had a mixed aetiology. Esotropia was observed in 20 (29%) patients and exotropia in three children (Fig 1).

Conditions associated with amblyopia and/or bilateral vision less than 20/50 in children with Down’s syndrome.
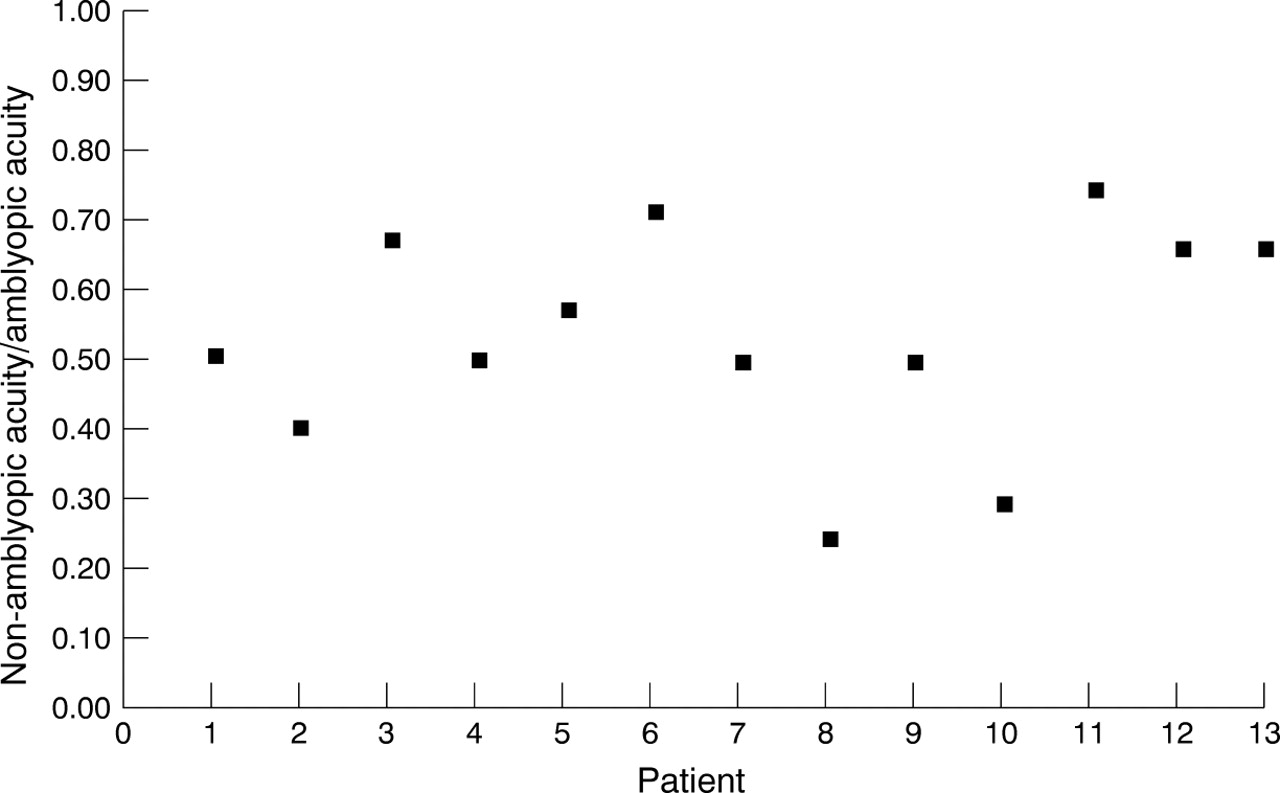
In order to better illustrate the differences in acuity between eyes of the amblyopic children, we plotted the ratio of the acuity of the non-amblyopic eye/amblyopic eye in a manner similar to that suggested by Howell et al.5 This method enables us to quantitate the difference in acuity between eyes. A ratio of 1.0 would indicate that the vision in the two eyes was equal, and a smaller number would indicate increasing differences in acuity between eyes (Fig 2). For the 13 children who could read a Snellen chart, the ratios ranged from 0.25–0.75. Five of the amblyopic children had ratios between 0.50 and 0.59.

Ratio of acuity in amblyopic children with Down’s syndrome.
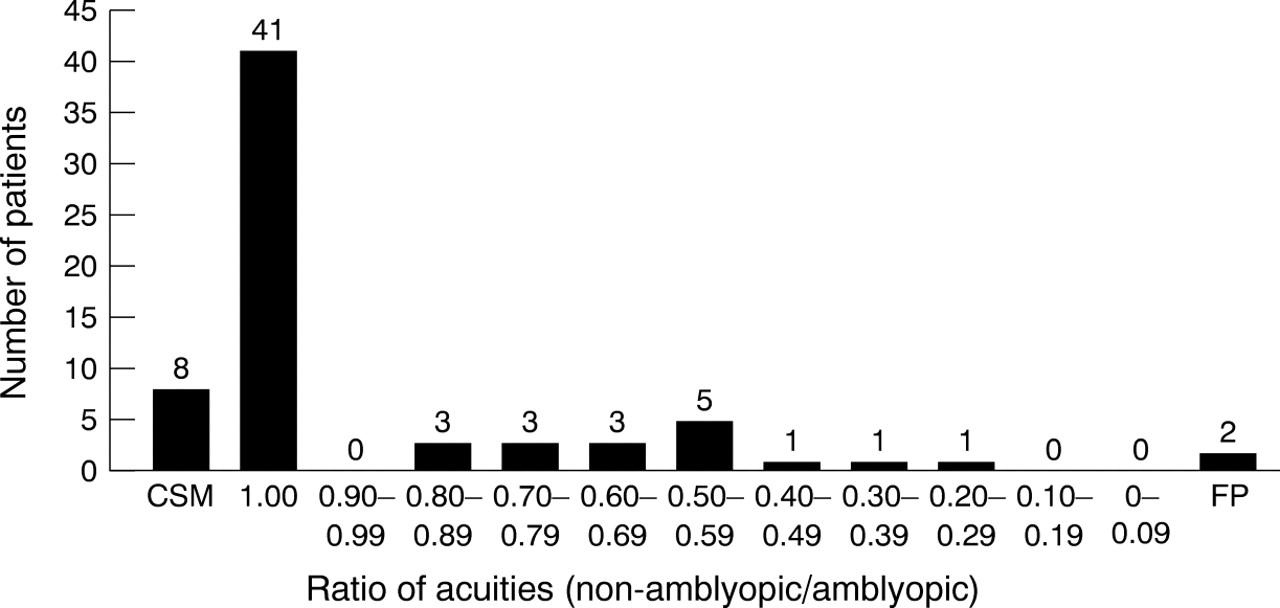
This method of analysis was then applied to the entire sample of 68 children. The distribution of the range of acuity ratios is plotted in Figure 3. Forty nine of the 68 children (72%) had either CSM vision or an acuity ratio of 1.0. The remainder of the study group had ratios distributed from 0.25 to 0.8. Five patients had ratios less than 0.5 or a clear fixation preference, which would indicate a substantial unilateral visual deficit. Within the group of patients with an acuity ratio of 1.0 however, there were the 16 children with bilateral 20/50 vision or worse.

{kind=link}
{kind=link}
{kind=link}
Distribution of acuity ratios in 68 children with Down’s syndrome.
Other ophthalmological conditions included esotropia in 20 (29%) and exotropia in three (4%) children. High myopia (more than 5 dioptres) was found in five (7%) children, lesser degrees of myopia were observed in an additional 11 (34%) children, and three children had more than 4 dioptres of hyperopia. Only six (9%) children had more than 1.75 dioptres of astigmatism. Various types of nystagmus were recognised in 12 (18%) children, yet in only three children was there an association with decreased vision. In addition, keratoconus and significant anisometropia were identified in one child, and congenital cataracts in another.
Discussion
Amblyopia in children with Down’s syndrome has been noted in only two previous studies. Hiles and coworkers found that 11 (8.5%) of 123 patients with Down’s had amblyopia,4 and Jaeger observed amblyopia in only three (13%) of 23 patients in whom reliable distance acuity was testable.3 Both of these studies involved institutionalised patients. Our study, however, is entirely composed of children brought up at home. Because we attempted to access all home reared children with Down’s syndrome between 5 and 19 years of age in Rhode Island, and since there is no apparent selection bias, the results of our study may more accurately reflect the prevalence of ophthalmological problems in children with Down’s syndrome in this age range.
We observed amblyopia in 15 (22%) of the 68 patients in our study group. This is a markedly higher prevalence than previously reported in patients with Down’s syndrome,3 4 and also significantly increased over the 2–2.5% prevalence figure for amblyopia in the general population.5 The high prevalence of amblyopia seems to parallel the increased frequency of other ophthalmological problems in children with Down’s syndrome.8 9 Strabismus and high refractive errors, both treatable conditions, were the most commonly encountered diagnoses associated with amblyopia in our study group.
The number of children with bilaterally poor vision bears further note. Though visual acuity was equal in the two eyes, 16 children (24%) had vision less than 20/50 in both eyes. Six of the 16 children had bilateral high refractive errors and several had strabismus, nystagmus, or a mixed cause for their visual acuities. Five of these children, however, had no apparent aetiology for their poor vision. Bilateral poor vision of unknown aetiology has also been noted by other investigators.3 6 Jaeger was able to obtain a Snellen acuity in 60% of his institutionalised patients and could only “rarely” obtain a distance acuity. “The majority” of his patients who could read a distance chart had 20/50, 20/70 vision.3 Wagner et al recorded visual acuity in only 15 of 188 patients with Down’s syndrome. The mean visual acuity in their group was 20/120, though 15 of the 30 eyes had a visual acuity of better than 20/60.7 Of note is the fact that the mean age of their study group was 4.1 years, and the mean age of those who could give a Snellen acuity was 8.9 years, whereas the average age in our study group was 10.6 years.
The use of visual acuity ratios (non-amblyopic acuity, amblyopic acuity) may be helpful in analysing the depth of amblyopia between eyes in this group of children in whom a large number manifest poor but equal acuity responses for both eyes. Generally, ratios less than 0.7 indicated amblyopia with a difference of at least two lines of Snellen acuity between eyes, with smaller fractions indicating an increasing disparity between eyes. The data in this study did not point to a threshold ratio for amblyopia, and the values of the ratios for the group of amblyopic children fell mostly into the 0.50–0.59 range.
Nystagmus was studied by Wagner et al who found this condition to be present in 30% of 188 individuals with Down’s syndrome.7 In our study only 12 (18%) patients were observed with nystagmus, and this condition accounted for decreased vision in only three children.
Strabismus is a common finding in people with Down’s syndrome and has been reported in 21–44% of patients.1-4 7 The prevalence of esotropia of 29% in our study population is similar to the prevalence rates previously noted.1-4 Strabismus frequently appeared to contribute to visual loss and amblyopia.
Conclusion
The results of this study indicate that 46% of our patients had a marked visual deficit including amblyopia and/or visual acuity less than 20/50 in both eyes. This represents a significant visual problem and raises concern about the overall visual function of children with Down’s syndrome. These findings are relevant to both ophthalmologists and paediatricians who provide care for children with Down’s syndrome and careful attention to ophthalmological problems in children with Down’s syndrome is warranted.