Article Text

Abstract
Aim To compare cycloplegic autorefraction with non-cycloplegic subjective refraction across all age and refractive error groups.
Methods In a cross-sectional study with random stratified cluster sampling, 160 clusters were chosen from various districts proportionate to the population of each district in Tehran. Following retinoscopy and autorefraction with the 0.25 D bracketing (Topcon KR-8000, Topcon, Tokyo, Japan), all participants had a subjective refraction. Then all participants underwent cycloplegic autorefraction.
Results The final analysis was performed on 3482 participants with a mean age of 31.7 years (range 5–92 years). Based on cycloplegic and subjective refraction, mean spherical equivalent (SE) was +0.31±1.80 and −0.32±1.61 D, respectively (p<0.001). The 95% limits of agreement (LoA) between these two types of refraction were from −0.40 to 1.70 D. The largest difference between these two types of refraction was seen in the age group of 5–10 years (1.11±0.60 D), and the smallest difference was in the age group of >70 years (0.34±0.45 D). The 95% LoA was −0.52 to 0.89 D in patients with myopia and −0.12 to 2.04 D in patients with hyperopia. We found that female gender (coefficients=0.048), older age (coefficients=−0.247), higher education (coefficients=−0.043) and cycloplegic SE (coefficients=−0.472) significantly correlated with lower intermethod differences.
Conclusions The cycloplegic refraction is more sensitive than the subjective one to measure refractive error at all age groups especially in children and young adults. The cyclorefraction technique is highly recommended to exactly measure the refractive error in momentous conditions such as refractive surgery, epidemiological researches and amblyopia therapy, especially in hypermetropic eyes and paediatric cases.
- Optics and Refraction
Statistics from Altmetric.com
Introduction
Visual acuity testing during the process of subjective refraction is a psychophysical examination and can be affected by several factors. Subjective responses can vary by visual experiences, mood, attention span, pupil size, accommodation changes, retinal adaptation, and general and ocular health.1–3 Other factors, independent of the individual, include room luminance, size and distance from the target, which can cause intersession differences in a person's responses. Such differences can lead to erroneous and different conclusions about an individual's visual status. Few studies have examined the repeatability of subjective measurement of refractive errors.4 ,5 In some of these studies, objective methods did not differ much from subjective methods; however, one of their most important limitations is comparing non-cycloplegic objective refraction.6 ,7
Cycloplegic refraction is necessary for the diagnosis of refractive errors in children,8 examinations before refractive surgery (keratorefractive surgery, phakic Intraocular lenses, identifying latent hyperopia and pseudomyopia, and cases with strabismus especially accommodative esotropia, high anisometropia, family history of strabismus, history of diplopia, poor cooperation, hysteria and malingering. Cycloplegic autorefraction is usually preferred in epidemiological studies of refractive errors in children. In addition, since children are less cooperative and their responses are unreliable, subjective refraction tests are not so valued and tests should be done objectively under cycloplegia. In some studies, autorefraction provided results different from subjective refraction.9 ,10
In a study by Choong et al,11 results with autorefraction devices compared with subjective testing tended towards minus overcorrection in children, which results in overdiagnosis of myopia. Pesudovs et al12 compared results with Nidek ARK-700A and Topcon KR-8000 against subjective testing, both autorefractors demonstrated perfect agreement with subjective refraction in this age group (mean age of 39 years) with little difference in measuring spherical equivalent (SE). In a study by Jorge et al,7 non-cycloplegic retinoscopy was found more reliable than autorefraction in children. All these studies have serious limitations. Main limitations of previous studies include not performing refraction tests under cycloplegia and having limited age groups.
In this report, comparing the results of our findings among all age groups, we performed cycloplegic autorefraction, which determines refractive errors more sensitively in comparison with subjective refraction.
Methods
This report concerns part of the Tehran Eye Study whose detailed methodology has already been described elsewhere.13 A brief description of the methodology is presented here.
Using a random stratified sampling approach, sampling from 160 clusters was done proportionate to the population of Tehran districts. After the selection of households, interviews were done door-to-door, and all members of the household were invited to have a complete eye examination.
Examinations
All participants of the Tehran Eye Study had complete eye examinations. Examinations included measurement of visual acuity without correction, with correction and with their presenting eyeglasses; dry retinoscopy, subjective refraction, cycloplegic autorefraction and lensometry of their current eyeglasses; colour vision tests, measurement of intraocular pressure and eye examinations with the slit lamp and funduscopy. All participants had an interview concerning demographics, educational level, history of eye disease, ocular trauma, diabetes, hypertension and history of eye examinations. For participants younger than 15 years of age, the interview was done with their parents.
Refraction was measured for all participants >5 years of age using a Topcon automated refractometer with the 0.25 D bracketing (Topcon KR-8000, Topcon) according to the instruction manual. The device was set to measure refraction five times and generate the average, which was recorded for analysis. Results from autorefraction were used as a starting point for full subjective and dry retinoscopy. If the visual acuity of either eye was less than 20/20, their subjective refraction and best corrected visual acuity (BCVA) were tested and recorded.
In order to increase the precision of subjective refraction examinations, a red–green test was used as the end point. For optimum positioning of the retinal image and achieving closest results to subjects’ BCVA, when patients reported that signs on the red background were dominant, a −0.25 D lens was placed, and if they preferred the green background, a +0.25 D lens added to achieve neutrality. For cases who report the two to be equally sharp, we recorded BCVA by considering the patient's preference in subjective refraction. Bichrome test (red–green test) was also used for binocular balancing of patients. For this purpose, we leaved each patient’s eye in similar condition of red–green test. In other words, when a patient reported an equal clarity in red and green, we put their other eyes at the same condition. In addition, in subjects unable to report an equal red and green result, we considered optimal visual acuity based on their preference in subjective refraction for both eyes.
If autorefraction was not possible (especially due to media opacity), dry retinoscopy and subjective refraction was attempted. If, to the ophthalmologist's judgement, there was no contraindication, cycloplegic autorefraction was done with Topcon autorefractor. In this case, two drops of cyclopentolate (1%) were instilled 30 and 25 min before autorefraction.14 Examination procedures and their order were described in a protocol and distributed among optometrists and ophthalmologists so that they all followed the same procedure. Based on cycloplegic autorefraction and subjective refraction, myopia and hyperopia were defined as an SE less than −0.5 dioptre (D), and more than 0.5 D, respectively, and any amount in between (−0.5 to +0.5) was considered as emmetropia. In this study, participants were categorised by age in the following seven groups: 5–10 years of age, 11–20, 21–30, 31–40, 41–50, 51–60, 61–70 and older than 70 years of age.
Statistical analyses
In line with previous studies, since SE in contralateral eyes were strongly correlated (Pearson correlation coefficient=0.845), we only used right eye data in the analysis. Comparisons were between SEs achieved from cycloplegic auto and subjective refraction using the paired t test. We used the Pearson correlation coefficient to demonstrate correlations between the two refractions. Taking cycloplegic autorefraction as the gold standard, we determined the sensitivity and specificity of subjective refraction in determining refractive errors. Using a multiple linear regression, we tested for independent effects of each of age, gender, education and cycloplegic SE while simultaneously adjusting for the effects of the other factors. We also computed the 95% limits of agreement (LoA) and generated a Bland–Altman plot to show the agreement between subjective and cycloplegic autorefraction methods.
Results
In this study, 6497 people were sampled, 4565 of which participated in the study (70.3%) (1–96 years old). In this report, we eliminated data of 1083 individuals from the analyses; 211 were below 5 years of age (because of low accuracy BCVA and subjective refraction), 810 did not have cycloplegic autorefraction (because of poor cooperation and contraindication for cycloplegic refraction) and 62 were missing subjective refraction test results (poor cooperation). Of the remaining 3482 participants, 2077 (59.6%) were female, and the mean age of the final sample was 31.7±18.1 years (range 5–92 years).
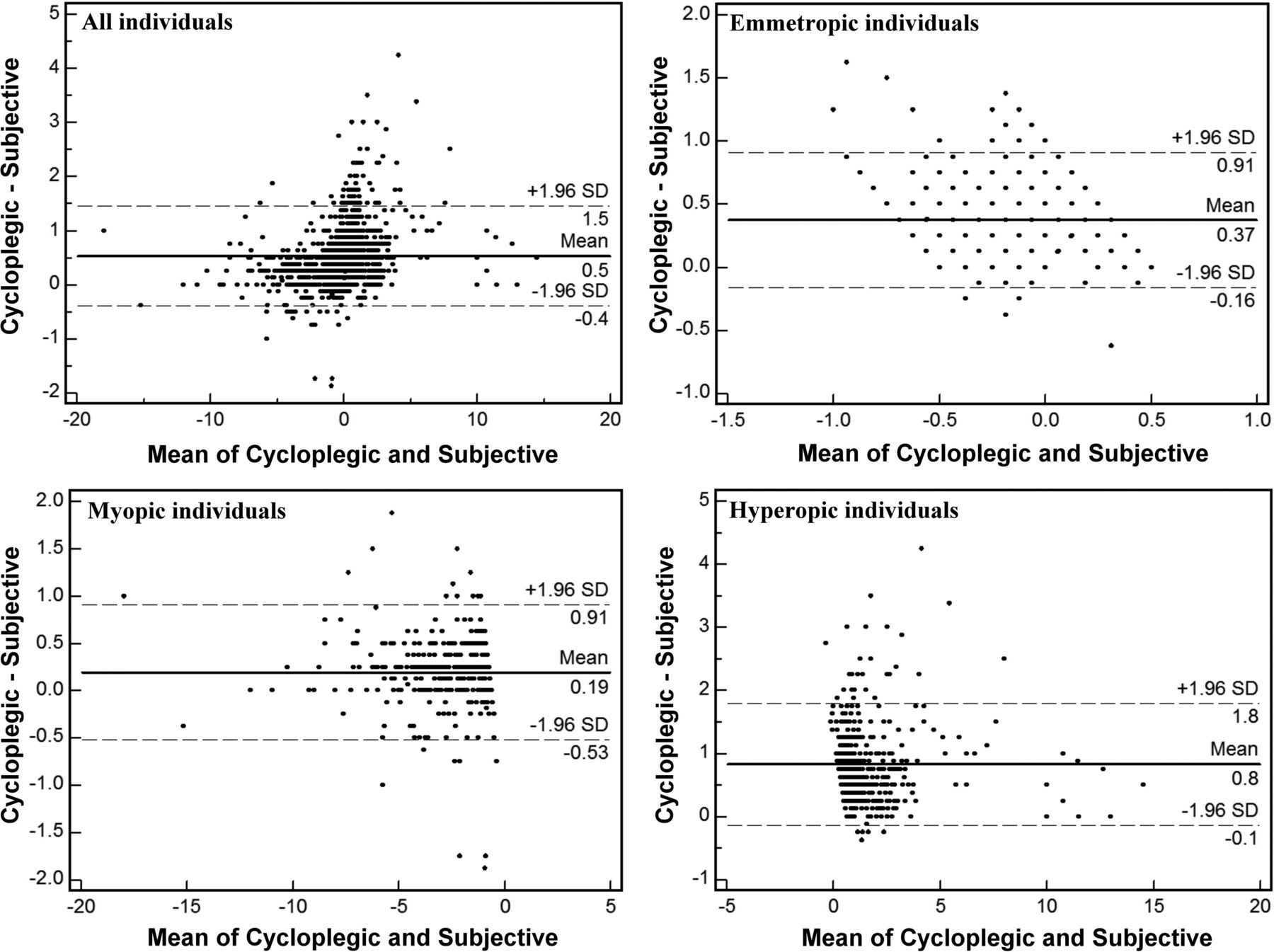
Mean SE was 0.31±1.80 D based on cycloplegic autorefraction and −0.32±1.61 D based on subjective refraction. Mean difference between these two methods was 0.62±0.54 D (p<0.001). The correlation between these two methods was high (r=0.956, p<0.001). The 95% LoA for these two methods were from −0.40 to 1.70 D. After grouping for age, the 95% LoA was −0.4 to 2.0 D for the age group below 20 years and −0.4 to 1.5 D in those older than 20 years. The 95% LoA was −0.52 to 0.89 D in patients with myopia and −0.12 to 2.04 D in patients with hyperopia. Figures 1 and 2 show Bland–Altman plots for the agreement between these two methods of refraction in individuals aged ±20 years.

Agreement between the cycloplegic and subjective measurements of the spherical equivalent in dioptre in individuals aged 20 years or younger in: all individuals (n=1251), patients with emmetropia (n=407), myopia (n=144) and hyperopia (n=700). The middle black line indicates the mean difference, the middle dash line is the lowest fit and the two side lines show the 95% limits of agreement.
Agreement between the cycloplegic and subjective measurements of the spherical equivalent in dioptre in individuals >20 years of age in: all individuals (n=2231), patients with emmetropia (n=868), myopia (n=423) and hyperopia (n=940). The middle black line indicates the mean difference, the middle dash line is the lowest fit and the two side lines show the 95% limits of agreement.
Figure 3 shows the histogram of intermethod differences. As demonstrated, the distribution of differences was skewed to the right with a skewness value of 1.513.
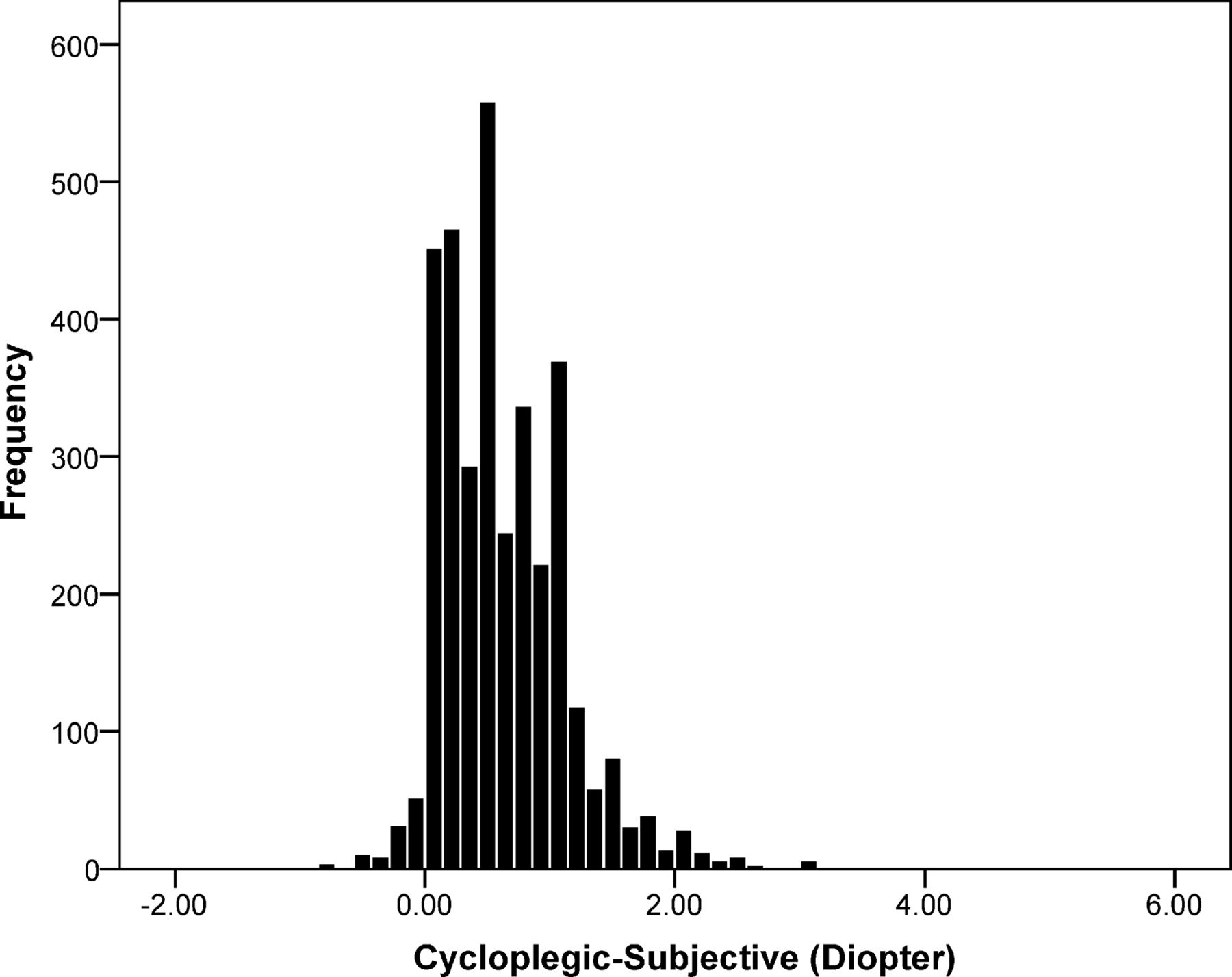
Distribution of differences between cycloplegic and subjective refraction.
Figure 4 displays differences between the two methods in different age groups. As demonstrated, largest differences were in the age group of 5–10 years, and smallest differences were observed in the age group of >70 years. According to our results, the difference between these two methods was 1.11±0.60 D in the age group of 5–10 years and 0.34±0.45 D in the age group of >70 years. The difference observed between cycloplegic and subjective refraction was larger in men (0.67 D) than women (0.59 D) (p<0.001). The median difference between cycloplegic and subjective refraction in men and women was 0.63 and 0.50 D, respectively. Intermethod differences significantly decreased with age (p<0.001). Our results also showed decreased differences with higher education (p<0.001).

Differences between cycloplegic and subjective refraction by age group. The middle line in the box represents the median and the top and bottom lines show quartile 1 (Q1) and quartile 3 (Q3). The height of the box represents the IQR. Whiskers outside the box illustrate the maximum and minimum. Round points show outliers and stars are extreme cases. (Range is between 1.5×IQR below Q1 and 1.5×IQR above Q3 and anything outside of this range is called an outlier).
Results of multiple linear regression indicated that female gender (standardised coefficients=0.048, p<0.001), older age (standardised coefficients=−0.247, p<0.001), higher education (standardised coefficients=−0.043, p=0.003) significantly correlated with lower intermethod differences. In this model, cycloplegic SE also showed a statistically significant correlation (standardised coefficients=−0.472, p<0.001).
According to our results, myopic subjects had the smallest differences between cycloplegic and subjective refraction and hyperopes had the largest; the intermethod difference was 0.19 D in the former group and 0.96 D in the latter (p<0.001).
Figures 1 and 2 illustrate Bland–Altman plots for the agreement between cycloplegic and subjective refraction by type of refractive error in individuals under and over 20 years of age. As demonstrated, in these two age groups, the highest agreement was observed in emmetropes and the least agreement was among hyperopic cases.
Taking cycloplegic autorefraction as the gold standard, our results showed that subjective refraction had a 98.1% sensitivity rate for detecting myopia of −0.5 D and higher, while the sensitivity rate for detecting hyperopia (0.5 D and more) with this method was 20.5%, and 79.5% of results were false negative. Table 1 summarises sensitivity rates of subjective refraction compared with cycloplegic autorefraction in detecting myopia and hyperopia, and 95% LoA between these two types of refraction in different age groups. As demonstrated, the sensitivity rate of subjective refraction for detecting myopia was >94% in all age groups. For hyperopia, the sensitivity rate was 5.6% with 94.4% false results in the age group of 5–10 years, and as it increased with ageing, the rate reached 76.9% in the age group of >70 years with about 23% false negative results in detecting hyperopia. Table 2 presents the area under the receiver-operating characteristic curve of SE based on subjective refraction for detecting myopia and hyperopia.
Sensitivity rates of subjective refraction compared with cycloplegic refraction in detecting myopia and hyperopia and 95% limits of agreement (LoA) between these two types of refraction
Area under the ROC curve: use of spherical equivalent base on subjective refraction to detect myopia and hyperopia according cycloplegic autorefraction
Figure 5 demonstrates a comparison of these two methods in detecting myopia and hyperopia in different age groups. As demonstrated, the numbers of hyperopia cases in younger age groups are significantly fewer with subjective refraction. Overall, the prevalence of hyperopia is higher with cycloplegic autorefraction in all age groups when compared with subjective refraction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of cycloplegic (C) and subjective (S) refractive errors by age.
Discussion
The present investigation is one of the few studies around the world looking into differences between cycloplegic and subjective refraction in all age groups. Here, we compare subjective refraction versus cycloplegic autorefraction, using the latter as our gold standard.
We discussed the validity of objective non-cycloplegic refraction in a previous report on the Tehran Eye Study.15 However, we prepared this report due to the importance of subjective refraction as the actual refraction accepted by the examinee. As mentioned in the results, results of cycloplegic autorefraction had a hyperopic shift of about 0.6 D compared with subjective refraction; highest amounts of shift were observed in hyperopic and smallest amounts were seen in myopic participants. During subjective refraction, hyperopes tend to accommodate to achieve clear vision, but myopes do not, because the image is focused in front of the retina, and there is no accommodation effort. By eliminating the accommodation function and performing cycloplegic autorefraction, a positive refraction shift can be observed in cases with hyperopia. Another reason for the high difference in hyperopes is related to tonic accommodation. Hyperopic eyes show higher levels of tonic accommodation due to differences in innervation and the autonomic control of accommodation in different forms of refractive error.16 By paralysing accommodation and inhibiting tonic accommodation, a greater positive refraction shift is observed in hyperopes than myopic individuals, and this is a strong justification for the observations in our study.
According to our results, there was a positive or hyperopic shift when cycloplegic autorefraction was compared with non-cycloplegic subjective results of most participants; nonetheless, a few cases demonstrated a negative or myopic shift with cycloplegia. This could be attributed to two factors including an increased positive spherical error as a result of mydriasis and low accuracy of the device or examiner in performing cycloplegic and subjective refraction. It must also be noted that changes in aberrations as a result of cycloplegia can be one reason for this myopic shift. One factor that may have a role in the observed negative shift is increased positive spherical error when the pupil is dilated during cycloplegic autorefraction. With a mydriatic pupil, the periphery of the crystalline lens is involved in retinal image formation and this increases positive spherical error.17 Subsequently, the focus of the image shifts towards the anterior of the eye, and the refractive status experiences a myopic shift.18 With these explanations in mind, the myopic shift observed in some cases can be attributed to increased positive spherical error, low testing accuracy or both.
Differences between subjective and cycloplegic autorefraction results varied by the subjects’ age. Largest and smallest differences were observed in the age groups of 5–10 years and >70 years, respectively. This is due to the active accommodation in the age group of 5–10 years, which is not controlled during subjective refraction. Fogging can partly inactivate accommodation during subjective testing, but it does not inhibit it as much as cycloplegia; this is important in cases with latent hyperopia and pseudomyopia. Tonic accommodation is not affected with fogging, and it can only be inactivated by cycloplegia. Consistent with age-related decline in accommodation, differences between cycloplegic and subjective tests’ results decrease with ageing.19 ,20 In old people aged >60 years, the high prevalence of hyperopia is expected to be associated with large differences between subjective and cycloplegic autorefraction results, but this is overcome by the significant decline in the range of accommodation. Of important note, tonic accommodation decreases with ageing as well,20 and this can be another reason for smaller differences between the two methods of refraction. In light of this fact, Koivula et al21 suggest that hyperopic cases undergo phakic intraocular lenses surgery later than myopic individuals, but there is no suggestion on the best age for myopes and hyperopes to have this surgery.
In cases of myopia, subjective refraction had acceptable sensitivity in all age groups compared with cycloplegic autorefraction, and it was not <94% in any age group. The situation was different with hyperopia. In cases of hyperopia, the sensitivity of subjective testing showed an overall increase with age. The lowest sensitivity was observed in the age group of 5–20 years, and the highest was in the age group of >70 years.
We could say that subjective testing has acceptable sensitivity (>70%) for those >60 years of age, but in younger age groups, especially those below 40 years, it is not sensitive enough (<8%) for identifying hyperopia and sensitivity rates are very low (table 1). An obvious reason for this observation relates to the age-related decline in accommodation amplitude and tonic accommodation, which dampens the effect of uncontrolled accommodation during subjective refraction of older examinees and helps achieve more accurate results, although they are never as accurate as cycloplegic results at any age. This highlights the necessity of cycloplegia for achieving accurate refraction results especially in patients younger than 40 years. In fact, if we rely only on subjective refraction, it is possible to miss some hyperopic children who have significant hyperopia and are at risk of refractive amblyopia, accommodative esotropia and resultant strabismic amblyopia. To avoid such issues, cycloplegic refraction seems to be essential to detect all patients with hyperopia at risk of amblyopia.
One of the important applications of comparing cycloplegic and subjective refraction results is in refractive surgical procedures. Most people seeking such procedures are aged between 20 and 40 years. Our study demonstrated a sensitivity rate of about 100% for detecting myopia by subjective refraction, and thus, the test appears reliable, while the sensitivity rates was <10% in hyperopic individual aged 20–40 years.
Therefore, the importance of cycloplegic autorefraction in hyperopic candidates of refractive surgery is pointed out, and it can affect the surgeon's decision in terms of amount of correction.
As demonstrated, the amount of hyperopic shift with the cycloplegic method compared with subjective refraction was significantly higher in men than in women. We could not find any particular explanation for this difference. This could be due to intergender neurophysiologic differences in the autonomic control of the accommodation system. Other possible reasons include women being more sensitive to blurry optotypes during subjective testing, as well as differences in tonic accommodation. Further studies are needed to understand the actual reason for the observed difference between men and women.
Conclusion
Despite a strong correlation, results of cycloplegic and subjective refraction were different in all age groups. This difference decreases with age, and is greater in men than women. When deciding about the actual refraction, subjective refraction appears to be reliable in myopes of all ages, because it provides results that are comparable with those by cycloplegic refraction as the gold standard method. However, for hyperopes, especially cases younger than 40 years, subjective refraction testing is much less sensitive than cycloplegic refraction, even though it has acceptable sensitivity in hyperopes older than 60 years. Therefore, accurate refraction is needed for hyperopic individuals and performing cycloplegic refraction seems to be necessary when determining eligibility and correction amount in refractive surgery and making employment and judicial decisions, as well as for the diagnosis and treatment of amblyopia, strabismus, high anisometropia and in younger adults and children.
References
Footnotes
Contributors Design and conduct of the study: HH and AF. Collection and management of the data: HH and AF. Analysis and interpretation of the data: MK, SS, AA, ND and AY. Preparation, review and approval of the manuscript: HH, MK, SS, AA, ND, AY and AF.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Ethics approval The Ethics Committee of Iranian National Research Center for Medical Sciences approved the study protocol, which was conducted in accord with the tenets of the Helsinki Declaration.
Linked Articles
- At a glance