Article Text

Abstract
Aim To study the outcomes of simple limbal epithelial transplantation (SLET) for unilateral total limbal stem cell deficiency (LSCD) secondary to severe ocular surface burns in children.
Methods Retrospective interventional case series was performed at a private referral tertiary care centre. Children less than 15 years of age who underwent autologous SLET for total LSCD and had a minimum follow-up of 6 months were included in the study. Demographic and clinical data were recorded in a predesigned form. All patients underwent SLET with a standardised technique. The outcome was defined as complete success (completely epithelialised, avascular corneal surface), partial success (focal recurrence of symblepharon not involving the visual axis) and failure (unstable ocular surface with persistent epithelial defects/symblepharon recurrence involving the visual axis).
Results The mean age was 5.75 years (range 2–12). The male to female ratio was 3:1. All eyes (four) presented in the acute phase, had grade 6 chemical injury (Dua classification) and underwent amniotic membrane transplantation at presentation. The mean interval between initial injury and SLET was 6 months (range 4.5–8). The outcome was complete success and partial success in one-fourth and three-fourths of cases, respectively. The overall follow-up was 12–60 months. Pre-SLET visual acuities were hand motions (one eye) and perception of light (three eyes). Post-SLET visual acuities were counting fingers close to face (one eye), 6/36 (two eyes) and 6/18 (one eye) at final follow-up. Cases with partial success underwent repeat SLET with conjunctival autograft, after which the outcome was complete success in all cases at varied follow-up intervals (13–36 months).
Conclusions SLET appears to be a promising technique for treatment of LSCD secondary to ocular surface burns in children.
- Cornea
- Ocular surface
- Stem Cells
- Child health (paediatrics)
- Trauma
Statistics from Altmetric.com
Introduction
The corneal epithelial stem cells located at1 ,2 the basal layer of the limbal epithelium are believed to be responsible for corneal epithelial transparency and health. Severe ocular surface burns cause damage to these cells, leading to limbal stem cell deficiency (LSCD) that in turn results in loss of corneal clarity, often leading to unilateral or bilateral corneal blindness.3 This corneal blindness has extremely poor prognosis for corneal transplantation unless ocular surface is reconstructed.4 With the advent of different techniques of limbal stem cell transplantation (LSCT), it has become possible to treat such eyes.5–7 The technique of LSCT evolved from transplantation of two conjunctival–limbal lenticules, each 3 clock hour width8 (conjunctival–limbal autograft, CLAU), to ex vivo cultivation of less than one clock hour of donor limbus grown over a transplantable epithelial sheet transferred to the bare ocular surface, the concept of cultivated limbal epithelial transplantation (CLET).7 ,9 Simple limbal epithelial transplantation (SLET), an inexpensive technique of in vivo expansion of limbal stem cells that does not require a specialised laboratory, has recently been proposed.10
The published success rate of LSCT in paediatric age group11 is lower than in adult population.9 ,12–17 The largest series published on paediatric autologous LSCT by ex vivo cultivation (CLET) showed up to 50% success rate.11 In the present communication, we describe our experience with SLET for treatment of unilateral total LSCD secondary to severe ocular surface burns in four children.
Methods
Study design and subjects
This was a retrospective interventional case series performed at Cornea and Anterior Segment Services of Sanjivni Eye Care, Ambala, India, from November 2009 to February 2015. A written informed consent was obtained from parents/guardians of all patients for all the investigations and surgical procedures. Children less than 15 years of age with unilateral total LSCD secondary to ocular surface burns who underwent SLET and had a minimum follow-up of 6 months were included in the study. We used the previously specified clinical definition of LSCD (the absence of the limbal palisades of Vogt, dull and irregular corneal epithelium, superficial corneal vascularisation, persistent epithelial defects (PEDs) and conjunctival overgrowth on the corneal surface).10
Data collection
The demographic and clinical data were collected in a predesigned form that included the age and gender of the child, the duration of the chemical injury prior to presentation, the surgical/medical intervention during the acute phase, the clinical condition after epithelialisation (quadrants of symblepharon, the presence of a PED, the cumulative degree of conjunctivalisation), the timing of performing SLET and preoperative and postoperative best corrected visual acuities (BCVAs).
Surgical technique
The surgical technique was similar to the one described by Sangwan et al,10 In brief, it had the following steps: a 3×2 mm size limbal biopsy was harvested from the contralateral donor eye from the superior limbus. The recipient eye was freed of vascularised pannus, bleeding vessels were cauterised and human amniotic membrane (hAM) graft was secured over the bared ocular surface with fibrin glue. The donor tissue was cut into 6–8 small pieces (limbal transplants) with either Vannas scissors or No. 15 surgical blade (Asian Surgicals, Hyderabad, India). These transplants were placed at limbus in two cases and uniformly distributed on the hAM leaving a clear visual axis in two cases and were held in place with fibrin glue. At the end of the surgery, a soft bandage contact lens (BCL) was placed over the cornea. A symblepharon ring was placed in three cases (Cases 1, 2 and 3). Fornix forming sutures were also placed in two cases (Cases 1 and 2). The eye was patched overnight after instilling topical 5% povidone–iodine.
The cases that had a focal recurrence (defined below) underwent repeat SLET using similar limbal tissue 1–2 clock hours away from previous donor site combined with suitable sized conjunctival autograft (CAG) harvested from superior bulbar conjunctiva of healthy eye.18
Postoperative management and follow-up
Topical prednisolone 1% was prescribed in tapering doses for 4 weeks in donor eye and 2–3 months (depending on surface inflammation) in recipient eye. Topical moxifloxacin 0.5% was used four times a day in both eyes till epithelialisation, along with preservative-free lubricants. The patient was seen on the first postoperative day, weekly in the first month, monthly for 3 months and every 3 months till last follow-up. The symblepharon ring and fornix forming sutures were removed at 1–2 weeks postoperatively depending on the epithelialisation of the ocular surface and the level of discomfort in the child.
Outcome measure
The outcome was defined as a complete success (completely epithelialised, avascular and stable corneal surface); partial success (an epithelialised ocular surface with a focal recurrence of LSCD in the form of pannus not involving the visual axis) and failure (unstable surface with recurrent or PEDs or pannus involving the visual axis).
Results
All surgeries were performed by a single surgeon (VM). During the study period, 11 cases underwent SLET at our centre for LSCD secondary to chemical or thermal injuries and four of them were children. All the four cases presented to us in the acute phase and were managed initially with an aim of saving the globe and later for visual rehabilitation. The mean age was 5.75 years (range 2–12). The male to female ratio was 3:1.
Acute phase management of chemical injury
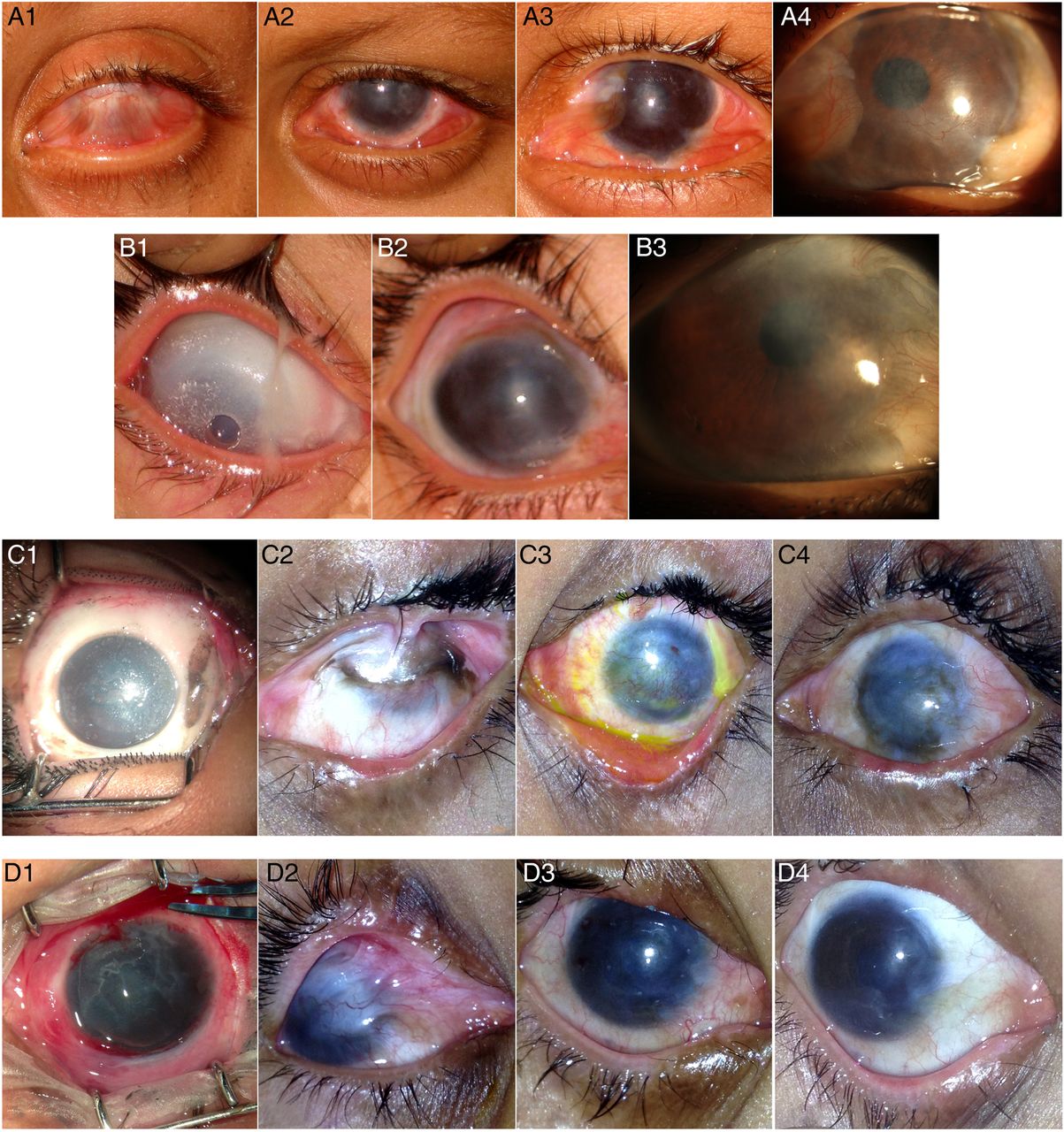
The demographic data, clinical features and management during the acute phase of ocular burn are provided in table 1. All patients had grade 6 chemical injury (Dua classification).19 Three eyes (Cases 1–3) had particles of an offending agent (lime in Cases 1 and 2; dust and gun powder in Case 3, figure 1C1) in fornices and had associated extensive episcleral and scleral ischaemia. All patients underwent copious wash in the operating room, debridement of necrotic tissue and amniotic membrane grafting (AMG). Repeat AMG was needed once in Case 2 and five times in Case 3 for PED. Complete ocular surface epithelialisation was achieved in 1.5–4 months in all eyes. There was extensive symblepharon in all eyes (figure 1A1, C2, D2), obliteration of superior and inferior fornices in two eyes (Case 1, figure 1A1 and Case 2) and obliteration of superior fornix in one eye (Case 3) (figure 1C2).
Demographic and clinical data of paediatric patients with unilateral ocular surface burns during the acute phase
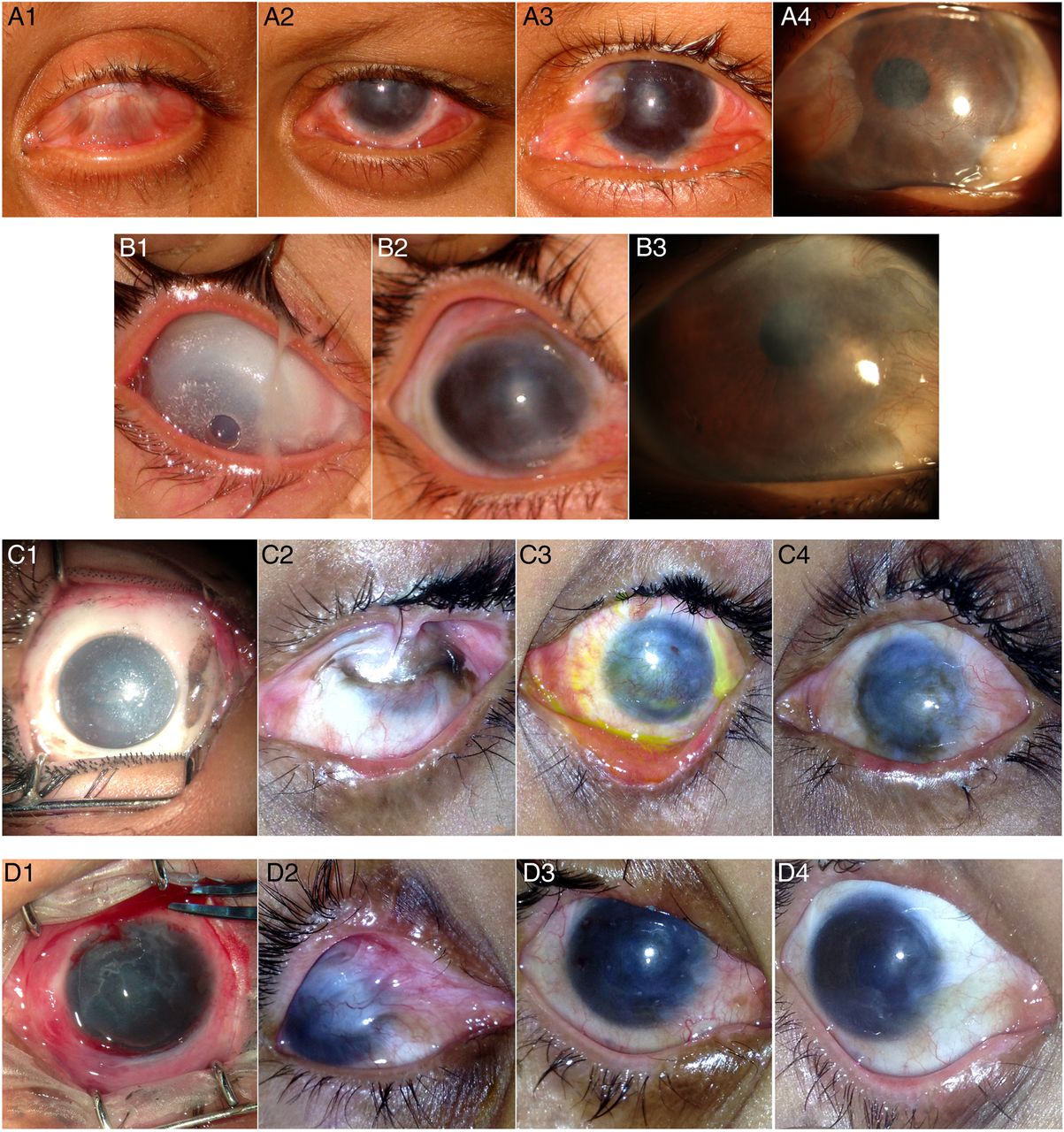
Serial clinical pictures of Cases 1–4. Case 1 (A1–A4) (A1): pre-op simple limbal epithelial transplantation (SLET) clinical picture showing extensive symblepharon and obliteration of inferior fornix; (A2): 18th postoperative day (POD) after SLET; (A3): 3 months post-op showing epithelialised surface, hazy cornea and early sign of focal recurrence nasally; (A4): 2 years post-op showing clear corneal epithelium; Case 2 (B1–B3) (B1): 1st POD after SLET showing conformer in place to prevent symblepharon formation; (B2): 45 days post-op showing epithelialised surface and hazy cornea; (B3): 1-year post-op showing clear corneal epithelium and visible iris details; Case 3 (C1–C4) (C1): 5 h after firecracker injury showing total epithelial loss and limbal ischaemia; (C2): 8 months post-initial injury showing severe limbal stem cell deficiency (LSCD) and obliteration of superior fornix; (C3): 2 weeks post-SLET showing epithelialised ocular surface; (C4): 13 months post-op showing stable ocular surface; Case 4 (D1–D4) (D1): 26 days after firecracker injury showing near total epithelial loss; (D2): 4 months post-initial injury showing symblepheron; (D3): 4 weeks post-SLET showing epithelialised ocular surface; (D4): 6 months post-op showing stable ocular surface.
Management of stem cell deficiency
SLET was performed in all eyes once the surface was completely epithelialised and inflammation was under control. Table 2 describes the clinical details during SLET surgery and figure 1 shows serial clinical pictures of these patients. The mean time interval between the initial injury and SLET was 6 months (range 4.5–8 months). All four children had accurate projection of rays at the time of intervention. Complete success was achieved in one-fourth of cases. The cases with partial success (three-fourths of cases) had a focal recurrence of LSCD that was managed with repeat SLET and CAG.18 (figure 2; table 3). After repeat SLET, the outcome was complete success and none of these patients had a recurrence of LSCD at varied follow-up intervals (12–60 months after first SLET and 13–36 months after repeat SLET).
Clinical data of patients who underwent simple limbal epithelial transplantation (SLET)
Repeat SLET for focal recurrences

{kind=link}
{kind=link}
Repeat simple limbal epithelial transplantation (SLET) for focal recurrence in Cases 1, 2 and 3. Case 1 (A1–A3): (A1): focal recurrence in the form of symblepharon; (A2): 2 months post-repeat SLET and conjunctival autograft (CAG); (A3): 60 months post-primary SLET and 36 months post-repeat SLET showing stable ocular surface; Case 2 (B1–B4) (B1): focal recurrence seen superiorly in one quadrant; (B2): 2 days post-repeat SLET, white arrows show explants of SLET and black arrow points to CAG; (B3): 2 months post-op showing CAG in place; (B4): 1-year post-repeat SLET and 3 years post-primary SLET showing stable ocular surface and no recurrence; Case 3 (C1–C3) (C1): focal recurrence seen superiorly in one quadrant; (C2): 2 months post-op showing CAG in place; (C3): 6 months post-repeat SLET showing recovery of surface.
Discussion
In the present communication, we report the first series on paediatric LSCT using SLET technique. We were successful in achieving a stable, avascular ocular surface after one or two SLET procedures in extensive LSCD secondary to severe chemical burns in children. As these children were managed at our centre both in acute and late phases of chemical injury, the present study provides a complete clinical course in such patients. We also describe in detail the characteristics and management of focal recurrences after SLET.
SLET is a novel technique that combines the advantages of CLAU (low cost, single staged, independent of stem cell laboratory) and CLET (using minimal donor tissue).10 There are two full-length articles on the results of SLET so far (six and four cases, respectively)10 ,20 and rest being isolated reports.18 ,21–25 Unlike our study, both of these articles included adult patients but no paediatric patient and reported 100% success rate after SLET. The success rate in our series after first surgery was 25% (one out of four). The most likely reason for the same could be the extensive LSCD secondary to grade 6 chemical burns (table 1). The success rate improved to 100% after repeat SLET and the ocular surface remained stable even after 12–60 months (median 35.5 months). In contrast with previous SLET studies10 ,20 (9.2 months and 7.5 months), this follow-up (up to 60 months) is the longest published follow-up after SLET so far, pointing towards the long-term efficacy of this procedure.
The success rate of CLET for LSCD secondary to chemical injuries has been reported between 64.5% and 80% with various culture techniques.9 ,12 ,13 At one centre, the reported success of LSCT (CLET technique) in children was much lower (46.7% of 107 subjects)11 than in adults (68% of 200 subjects)9 with similar injuries, with authors suggesting that the results of LSCT in children may not match the same in adults. They also found microbial keratitis as the most common complication due to possible contamination during ex vivo cultivation of cells. In contrast, the present series showed 100% success after one or two LSCT procedures using SLET technique and without any postoperative complications. The successful results of previously published10 ,20 and the present SLET series seem to indicate that the cultivation of limbal stem cells in vivo may be superior to ex vivo culture of these cells.
Another reason for good outcomes even in severe cases of the present series may be the better inherent potential of individual transplants of our young patients. In another study on ocular surface epithelialisation pattern after SLET, we found higher activity in individual transplants of children than adults.25 However, this needs to be substantiated by further studies on large number of patients.
The ocular surface inflammation was intense at presentation (the acute phase of injury), started decreasing only after complete ocular surface epithelialisation (1.5–4 months; table 1) and persisted for 2–5 months (table 2) even after epithelialisation. We performed LSCT after the eye became quiet. As a conducive environment is very important for the stem cells to survive, we feel it is better to wait for a few months for epithelialisation and control of inflammation than risk the stem cells taken from the healthy eye. The appropriate timing of such surgery in children is always a dilemma and needs further studies because early intervention during surface inflammation may increase chances of failure, and late intervention may result in amblyopia despite a stable surface.11
There were four distinct findings in cases with partial success (three out of four): first, these cases had more severe injury to the ocular surface in the acute phase (episcleral and scleral ischaemia, delayed ocular surface epithelialisation) and more extensive LSCD later (four-quadrant symblepharon; obliteration of fornices). This finding has been observed previously26 and indicates that the success or failure of stem cell transplant may depend on severity of initial insult to the ocular surface.
Second, these cases had a focal recurrence of LSCD in the form of pannus and symblepharon but no inflammation or PEDs. Third, the focal recurrences were noticed in the area of maximum severity of preoperative symblepharon (figures 1C2 and 2C1). Hence, one of the causes for such a recurrence could be the extensive damage of the conjunctiva during initial injury and a focal loss of the conjunctival stem cells. To overcome this, we placed CAG during repeat SLET and had satisfactory results18 (table 3). Hence, an appropriate assessment of symblepharon should be done preoperatively and one may consider CAG in extensive symblephera during the primary surgery itself. Although the focal recurrences (symblephera) in our cases were neither progressive, nor encroaching the pupillary area, yet we opted to treat them. The causes for the same were restriction of motility (Case 1), cosmesis (Case 2) and the need for a smooth ocular surface for future optical keratoplasty (Case 3). The success rate of repeat CLET is reported to be 66–81.8% in various studies12 ,27 and much lesser in paediatric age group (30%).11 In contrast, we had excellent results in repeat surgery (100%) indicating the superior efficacy of SLET.
Fourth, these focal recurrences presented within first 4 months after first surgery. The previous reports on CLET suggest that most of stem cell transplant failures occur within first few months (8 months in the largest series (444 cases) on CLET).28 In our study, the fourth case was followed for 12 months and had no recurrence. Similarly, the three cases that underwent a repeat procedure did not have any recurrence even after 13–36 months of repeat surgery. This indicates the burden of struggle faced by transplanted stem cells is maximum during early postoperative period, after which the cells may regain the near-normal function for long term. This hypothesis also needs validation through further studies.
As noted in earlier studies,10 ,20 there was no loss of BCVA in healthy eye in any case (table 4). One case (Case 1) showed subtle non-progressive pannus at donor site. In this case, although it was left eye that was mainly involved, the parents gave a history of chemical injury in right eye (donor) as well. At presentation to us (2 weeks after injury), the right eye did not have any epithelial defect and had only mild conjunctival congestion (table 4). It is possible that this eye had a low stem cell count at the time of surgery that otherwise appeared healthy. The pannus was noted 6 months after surgery and did not progress till 5 years of follow-up and hence no intervention was required. In rest of the cases, there was no evidence of donor site LSCD (see Supplementary Figures 1 and 2). In fact, it was difficult to locate the donor site 5–6 months after SLET in these cases. Subtle loss of pigmentation was the landmark used to assess the site of primary limbal biopsy (donor site) while performing the second procedure. Another key feature about the present study is that since all cases were managed in the acute phase of chemical injury (presented within 5 hours to 20 days) at our centre with AMG (for epithelialisation and control of inflammation), topical steroids (control of inflammation) and lid surgeries (to avoid mechanical trauma to the ocular surface), the best environment before SLET was possible, thus contributing to its success. We believe AMG during the acute phase helps in easier localisation of dissection plane between pannus and cornea during SLET.
Donor eye findings
As there was obliteration of fornices in three cases, a conformer was planned to be in place for 3–4 weeks, but had to be removed earlier (within 2 weeks) due to discomfort in children (table 2). We feel the conformer might have helped in preventing early adhesions in our cases. A BCL was placed in all cases for 4–6 weeks to protect the regenerating epithelium from the mechanical trauma by the lids. After removal of pannus and securing hAM, the limbal explants were secured with fibrin glue either circumferentially on limbus (Cases 1 and 2) or all over cornea (Cases 3 and 4). However, there was no difference in results between the two placements.
Although an improvement in BCVA was seen in all cases, it was limited due to amblyopia or corneal scarring. Visual acuity improved from PLPR to 6/36 in Cases 1 and 2. The causes of low vision in these cases were subtle corneal scar and amblyopia owing to visual deprivation at a very young age. Case 3 is awaiting penetrating keratoplasty (PKP) for a dense corneal scar. It was not performed along with SLET due to reports of poorer clinical outcomes of single-stage surgery (CLET with PKP) than a two-stage approach.29 Although Case 4 had maximum improvement in visual acuity (6/18), it was limited due to anterior corneal scar and may be considered for anterior lamellar keratoplasty in future.
To summarise, our study describes the use of SLET technique of stem cell transplantation in extensive uniocular LSCD in children, management of focal recurrences after SLET and long-term results of this surgery. Weaknesses of our study include the sample size and the retrospective nature of this study. However, LSCD itself is rare and in children it is difficult to conduct a prospective study with a large sample size for such a disease.
In conclusion, SLET technique of stem cell transplantation seems to be a very promising treatment for LSCD in children. Future studies and refinements in SLET may help in improving the outcomes and reaching out to help these patients of stem cell deficiency.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Contributors Design of the study—VM. Conduct of the study—VM and RM. Collection, management of data and analysis and interpretation of the data—VM, RJ and RM. Preparation, review or approval of the manuscript—VM, RJ, RM, UV and PN.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board (IRB) approval was not obtained for this retrospective study as it was based on clinical audit of cases of a single surgeon.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author has full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Linked Articles
- At a glance