Article Text

Abstract
Aims To evaluate the efficacy of lens removal plus intraocular lens (IOL) implantation for spherophakia with secondary glaucoma.
Methods A series of 19 patients (n=24 eyes) were split into two groups according to the degree of zonular abnormality as follows: group 1 (within the range of one quadrant, n=7 eyes) and group 2 (beyond the range of one quadrant, n=17 eyes). The patients in group 1 underwent phacoemulsification+capsular tension ring (CTR)+IOL, whereas patients in group 2 underwent pars plana lensectomy with scleral-fixated posterior chamber (PC) IOL implantation. The best corrected visual acuity (BCVA) (logMAR unit) and intraocular pressure (IOP) were documented at presentation and at 1 day, 7 days, 3 months, 1 year and 3 years postoperatively.
Results The IOP in both groups significantly decreased after surgery (group 1:28.84±5.36 mm Hg at presentation, 15.86±0.79 mm Hg at the 3-year visit, t=6.34, p=0.000; group 2:26.18±12.16 mm Hg at presentation, 14.54±3.40 mm Hg at the 3-year visit, t=3.80, p=0.01). The BCVA increased from 0.79±0.36 at baseline to 0.44±0.38 at the 3-year follow-up but did not reach a significantly different level in group 1 (t=1.72, p=0.11), whereas the BCVA significantly increased from 1.15±0.75 at baseline to 0.43±0.38 at the 3-year visit in group 2 (t=3.45, p=0.02).
Conclusions Both phacoemulsification+CTR+IOL and lensectomy with scleral-fixated PC IOL implantation are effective in lowering the IOP and enhancing the visual acuity in patients with spherophakia and secondary glaucoma.
- Glaucoma
- Lens and zonules
- Treatment Surgery
Statistics from Altmetric.com
Introduction
Spherophakia is an ocular condition in which the crystalline lens assumes a spherical shape with an increased anteroposterior diameter and reduced equatorial diameter.1 ,2 In spherophakia, although the primary abnormality is lens abnormality, the functional sequence is often permanent visual loss because of secondary glaucoma.1 Accordingly, interventions for spherophakia, to some extent, address the secondary glaucoma. However, there are no universal guidelines for the management of the secondary glaucoma with spherophakia. Antiglaucoma medicines do not work as well as they work for primary glaucoma, as they could effectively control intraocular pressure (IOP) in only 18% of glaucomatous eyes with spherophakia.3 Under these circumstances, surgical intervention is necessary for the eyes failing to respond well to medical treatment. Several surgical modalities have been reported to be effective in controlling IOP in spherophakia, such as lensectomy, phacoemulsification (phaco), goniosynechialysis, trabeculectomy and so on. The clinical evidence for the use of these procedures is currently derived from isolated case reports with limited follow-up and, in turn, is not sufficiently strong to guide clinical practice.1 ,4–6
For vision correction, a posterior chamber intraocular lens (PC IOL) is typically implanted; however, this procedure is not always feasible in the absence of stable capsule support for which the use of a capsular tension ring (CTR) has been advocated.7 As an alternative, a scleral-fixated PC IOL has been adopted. The implantation of a PC IOL with CTR after phaco or the insertion of scleral-fixated PC IOL after lensectomy is generally the primary procedure for the management of spherophakia. However, the paucity of the associated data on this procedure, which is likely due to the limited number of spherophakia cases, requires a rigorous study to be conducted to yield considerable evidence that could be helpful for clinical practice. In the present study, we recruited a relatively large sample size of participants in an effort to institute appropriate management for spherophakia with glaucoma.
Materials and methods
Patients
In this prospective, non-randomised, interventional case series between July 2007 and September 2011, 19 patients (24 eyes) who had undergone surgery for ectopia lentis associated with spherophakia and were followed for 3 years, were included. The inclusion criteria were the following: (1) a spherical shape of the lens upon mydriasis; (2) a lens thicker than 4.50 mm;1 (3) findings on ultrasound biomicroscopy (UBM)8 that demonstrated a shallow anterior chamber, a very steep anterior lens curvature, iridolenticular contact, elongated zonules, and an increased distance between the lens equator and the ciliary processes and (4) lenticular myopia. The patients were split into two groups according to the degree of zonular abnormalities as follows: group 1 (within the range of one quadrant, 6 patients/7 eyes) and group 2 (beyond the range of one quadrant, 13 patients/17 eyes). The patients in group 1 underwent phaco+CTR+IOL, whereas patients in group 2 underwent pars plana lensectomy with scleral-fixated PC IOL implantation. Each patient provided informed written consent prior to enrolment. The study was performed adhering to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board.
Outcome measures
Prior to the surgery and at the scheduled study visits, all patients underwent a complete ophthalmic examination that included assessments of uncorrected visual acuity (UCVA); best corrected visual acuity (BCVA) in manifest refraction; a slit-lamp examination; a gonioscopic examination; Goldmann applanation tonometry; a visual field examination (Octopus 900, Haag-Streit International, Koeniz, Switzerland); and a dilated fundus examination. The thickness of the lenses was determined using a Pentacam system (Pentacam HR; OCULUS Optikgerate, Wetzlar, Germany). A closed angle is defined as the invisibility of the meshwork on gonioscopic examination. Ultrasound biomicroscopy (the angle opening distance at 500 mm anterior to the scleral spur (AOD500) and the anterior depth were simultaneously measured) was performed at the time of presentation and at the 3-year visit. All measurements were performed five times, and the mean values were recorded for analysis. The patients were scheduled for follow-ups 1 day, 7 days, 3 months, 1 year and 3 years postoperatively. No patients were lost to follow-up at any time point.
Surgical procedures
Phaco+CTR+IOL (see online supplementary video 1) (performed by the same doctor, YL) was performed according to the following procedure. Pupils were dilated with 1% tropicamide and 1% phenylephrine drops. Each eye was anesthetised using a retrobulbar block, with 3 mL each of 0.5% bupivacaine and 2% lidocaine hydrochloride. A 2.6 mm corneoscleral tunnel incision at the 11 o'clock position was made, through which Healon was injected into the anterior chamber. A 15° blade was used to make a limbal incision at the 2 o'clock position. A capsulorhexis was then made in a 5.0 to 6.0 mm-diameter circle. Iris hooks (Grieshaber, Alcon, Fort Worth, Texas, USA), if necessary, were used to stabilise the capsular bag. Hydrodissection and hydrodelineation were then performed using a balanced salt solution. Phacoemulsification and/or aspiration were performed at a low-bottle height and a low-vacuum setting. After complete removal of the lens material, the capsular bag and the anterior chamber were expanded with sufficient Healon, and a CTR (PMMA14, Morcher, Germany) was inserted through the main incision into the capsular bag. The foldable IOL (Abbott Medical Optics, TECNIS ZA9003) was then injected into the capsular bag. Anterior vitrectomy was performed to remove the vitreous that had prolapsed into the anterior chamber, if necessary. Postoperatively, 0.5% levofloxacin and 0.1% fluorometholone eye-drops were administered four times per day for 2 weeks.
Pars plana lensectomy plus scleral-fixated PC IOL implantation (performed by the same doctor, YL) was performed according to the following procedure: pupils were dilated preoperatively, and the eyes were anaesthetised by a retrobulbar block as stated above. Patients older than 50 years underwent the previously described phaco procedure that followed lensectomy. Lensectomy and anterior vitrectomy via pars plana were performed using a 23-G outcome. Conjunctival peritomy was performed at the limbus (11 o'clock to 1 o'clock positions and 9:30 o'clock and 3:30 o’ clock positions). A partial thickness scleral incision and grooves were then made 1.5 mm posterior to the limbus at the 12 o'clock position, and two triangular scleral flaps were constructed at the 9:30 o'clock and 3:30 o’ clock positions. Sufficient Helon was injected into the anterior chamber. A needle with 10–0 polyglycan was inserted into the PC at the 9:30 o'clock position and exited at the 3:30 o'clock position beneath the scleral flaps. A special hook was introduced into the PC at the 12 o'clock position, and 10–0 polyglycan was pulled out of the eye through the super scleral tunnel incision. The suture was cut, and the ends were tied to the haptics where it was connected to the optical zone of an IOL (Rayner C-flex Aspheric Monofocal), which was then centrally inserted into the PC. Finally, the sutures were anchored and knotted within the bed of the scleral tunnel, and conjunctival incisions were closed with 8–0 nylon sutures. The postoperative regimen of eye-drops was identical to that used in the Phaco+CTR+IOL procedure.
Ex-Press implantation (performed by JC) was performed as follows. First, 0.5% bupivacaine and 2% lidocaine hydrochloride were injected into the sub-conjunctiva for anaesthesia. A superior (group 1) or supratemporal (group 2) conjunctival peritomy was performed. A 4 mm isosceles trapezoid-shaped scleral flap was then made. The scleral bed was saturated with mitomycin C (MMC) (0.5 mg/mL) for 3 min along with irrigation using the balanced saline solution. Paracentesis of the anterior chamber was conducted with a 25-G needle through which an Ex-Press shunt (model P50, Alcon, Fort Worth, TX) was inserted into the anterior chamber. The scleral flap was closed with 10–0 nylon sutures, and the conjunctiva was subsequently closed with 8–0 nylon sutures. Postoperatively, tobramycin and dexamethasone eye-drops were administered four times daily for 4 weeks.
Statistical analysis
The Statistical Program for Scientific Studies (SPSS) V.11.1 for Windows (SPSS, Chicago, Illinois, USA) was used for statistical analysis. A paired t test was performed at each visit in both groups. A p value <0.05 was considered statistically significant.
Results
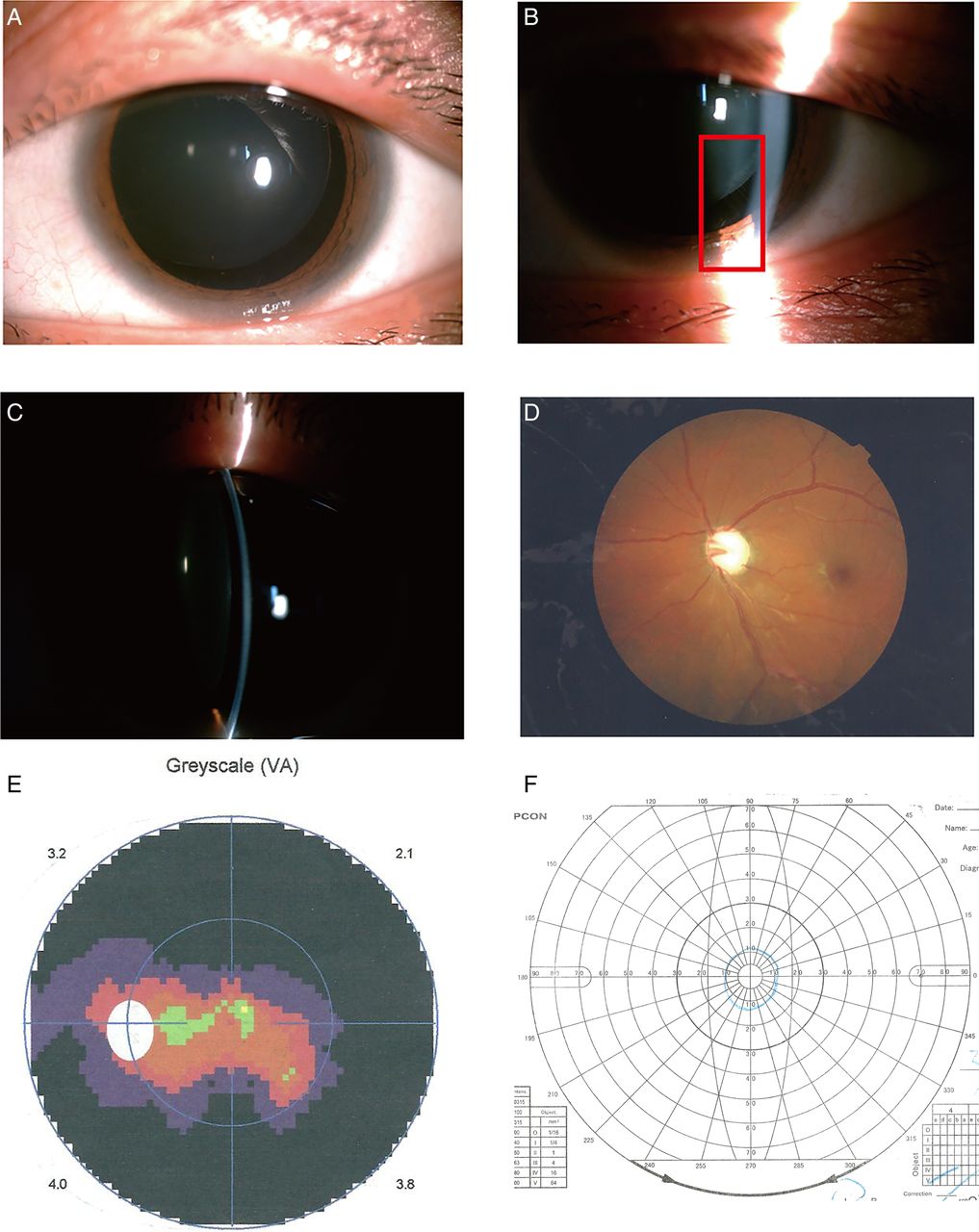
The demographic features at presentation are presented in table 1. The representative images of the slit lamp and visual field examinations are presented in figure 1. Of the 19 patients, 10 patients were younger than 18 years; 12 patients had Weill–Marchesani syndrome, and 7 patients were isolated spherophakia cases. At presentation, 19 eyes underwent laser peripheral iridotomy (6 eyes in group 1, 13 eyes in group 2), and one eye (in group 2) underwent trabeculectomy.
Demographic and clinical features of the patients at presentation
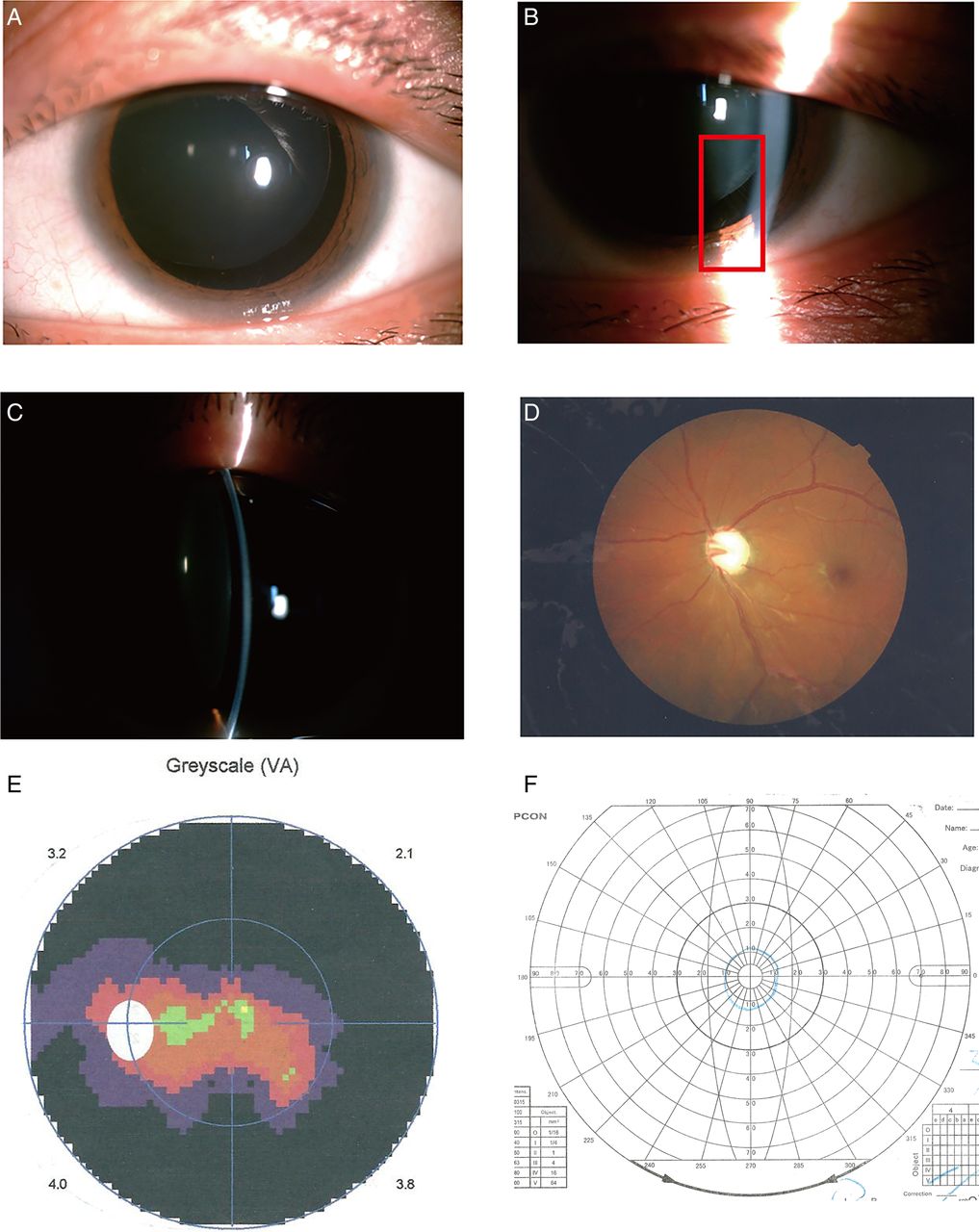
(A) A slit-lamp photograph of a candidate eye revealing a spherophakic lens with ectopia lentis; (B) a sparse and weakened zonule; (C): a shallow anterior chamber; (D) a fundus photograph (C/D=0.9); (E and F) visual fields showing advanced glaucomatous changes. VA, visual acuity.
The spherical equivalent of and the parameters associated with the glaucoma at presentation and 3 years postoperatively are presented in table 2; the anterior segment images before and after surgery are shown in figure 2; and the representative images from UBM and the Pentacam before and after surgery are presented in figures 3 and 4, respectively.
Spherical equivalent and the parameters associated with the glaucoma before and after surgery at 3 years

Photographs from slit lamp examinations. (A) Before surgery; (B–D) at 3 years postoperatively; (B) phaco+CTR+IOL; (C) pars plana lensectomy plus the scleral-fixated PC IOL; (D) phaco+CTR+IOL+Ex-Press implantation. Phaco, phacoemulsification; CTR, capsular tension ring; IOL, intraocular lens; PC, posterior chamber.
The mean IOP in the 24 eyes with secondary glaucoma decreased from 26.96±10.58 mm Hg at presentation to 14.93±2.93 mm Hg at the 3-year visit, and the number of antiglaucoma medications used by the patients decreased from 3.67±1.05 to 0.71±0.46 (table 3). In group 1, the mean IOP decreased from 28.84±5.36 mm Hg to 15.86±0.79 mm Hg (t=6.34, p=0.000), while it dropped from 26.18±12.16 mm Hg to 14.54±3.40 mm Hg (t=3.80, p=0.01) in group 2. Five eyes (2 eyes in group 1 and 3 eyes in group 2) underwent Ex-Press implantation due to the late-onset IOP elevation that could not be effectively controlled with antiglaucoma eye-drops.
Mean IOP and the eyes needing additional treatments and the numbers of the additional medicines
The mean BCVA in 24 eyes increased from 1.04±0.69 at baseline to 0.43±0.37 at 3 years postoperatively (table 4). The BCVA increased from 0.79±0.36 at baseline to 0.44±0.38 at the 3-year follow-up in group 1, although this difference was not significant (t=1.72, p=0.11), while it significantly increased from 1.15±0.75 at baseline to 0.43±0.38 at the 3-year visit in group 2 (t=3.45, p=0.02) (figure 3).
The best corrected visual acuity before and after surgery

Ultrasonographic biomicroscopy images. (A) a spherical lens with a shallow anterior chamber; (B) the elongated zonules and closed angle; (C) the well-centred lens and the normal depth of the anterior chamber at the 3-year visit; (D) the re-opened angle at the 3-year visit.
Two eyes underwent anterior vitrectomy 5 days in group 1 due to the prolapse of vitreous into the anterior chamber. The CTRs and IOLs were all in the capsular bag, with two of them exhibiting a slight decentration in group 1, whereas the IOLs were stably located in the ciliary sulcus in group 2 (figure 4). Six eyes developed different degrees of posterior capsular opacity and five eyes were successfully treated by Nd:YAG capsulotomy in group 1.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pentacam images. (A) Before surgery: the displaced lens and elongated zonules; (B–D) at 3 years postoperatively; (B) phaco+CTR+IOL; (C) pars plana lensectomy plus the scleral-fixated PC IOL; (D) phaco+CTR+IOL+Ex-Press implantation. Arrow a: elongated zonules; arrow b: CTR. Phaco, phacoemulsification; CTR, capsular tension ring; IOL, intraocular lens; PC, posterior chamber.
Discussion
The aim of both controlling IOP and correcting lenticular myopia seemingly justifies the development of a procedure aimed at treating the spherophakia itself. Lens removal plus IOL implantation have been introduced and have gained broad acceptance in managing this condition. However, no unanimously accepted guidelines are available for clinical practice in treating spherophakia with secondary glaucoma.
Implantation of a conventional PC IOL is a challenge for clinicians due to the combined effects of a smaller capsular bag and a weakened zonule for which assistance is provided by a CTR.9 ,10 Early studies have shown that CTR can improve capsular stability and maintain postoperative IOL centration in the setting of mild zonular weakness,11 ,12 as demonstrated in the present study in which IOLs were well centred in five of seven eyes (71.4%). However, CTR does not work well in the setting of seriously impaired zonules in spherophakia, whereas scleral-fixated IOL is an optimal alternative. With this understanding, the patients included in the present study were grouped according to the severity of the laxity of zonular fibres.
For IOP control, the eyes in both groups showed a significant decrease in the mean value, but in different manners. The IOP decreased slowly and plateaued 1 week postoperatively in group 1, whereas the IOP dropped sharply first and was subsequently slightly elevated in group 2. Prolapse of the vitreous into the anterior chamber may have contributed to the slow decrease in the IOP in group 1, whereas no entrance of the vitreous into the anterior chamber arguably occurred following anterior vitrectomy in group 2. Of note, the two procedures did not create a sufficiently direct impact on the IOP in approximately half of the patients, such that a reduction in the adjunctive antiglaucoma medicine was necessary. Furthermore, of the 21 eyes in which the anterior chamber angle was closed beyond the range of 180° at presentation, the angle was not ameliorated after surgery in only nine eyes (five eyes undergoing additional Ex-Press implantation), which indicates that most of the cases had actually benefited from the two procedures. The finding that 17 eyes still required additional antiglaucoma medicine implies that the removal of the spherophakia alone may fail to effectively lower IOP in cases with a synechial angle or an angle anomaly possibly existing in the re-opened anterior angle.3 This result has called into question the plausibility that lens surgery for spherophakia is superior in its efficacy in the management of secondary glaucoma over trabeculectomy, which has been reported to be effective in controlling IOP.13 Nevertheless, aside from its potentially serious complications, such as the development of a flat anterior chamber or malignant glaucoma,14 trabeculectomy cannot assume an important role in correcting lenticular myopia. In contrast, the two procedures reported in this study appear to be helpful for IOP control and yielded an improvement in BCVA.
The increase in the BCVA in group 1 was not statistically significant, which may be because the patients in group 1 had better BCVA at presentation due to the lower lens decentration. Also noteworthy is that posterior capsule opacification and/or IOL decentration decrease the improvement in BCVA, as was found in some cases. Fortunately, posterior capsule opacification is amenable to the treatment of Nd:YAG capsulotomy that is believed to have the potential to yield a favourable prognosis for vision. Generally, Phaco+CTR+IOL and pars plana lensectomy plus the scleral-fixated PC IOL are both effective in correcting spherophakia because the two main concerns associated with spherophakia, that is, the control of IOP and vision correction, can, to a certain extent, be addressed.
Determining an appropriate procedure for the management of spherophakia is difficult. A thorough understanding of the challenges inherent in ectopia lentis cases and the management of intraoperative complications will ensure that surgeons achieve the best possible surgical results.15 In conclusion, removing the spherical lens can relieve the anterior chamber of crowding, which is essential for the treatment of secondary glaucoma. However, the magnitude of the treatment effect in controlling IOP and improving BCVA relies on many factors, such as the disease duration and anterior chamber angle at presentation, and primarily depends on the treatment strategy.
The limitation of this study is that a comparative study was not performed between the groups due to the disparity in sample size. In addition, bias may exist because we preferred shunt surgery to trabeculectomy for the five patients in whom late-onset IOP elevation was not well controlled. Furthermore, the bag-CTR-posterior chamber intraocular lens complex is likely to dislocate to the vitreous cavity due to the potential progression of zonular abnormalities in patients with Weill–Marchesani syndrome.16 Further studies are warranted to validate the findings and corroborate the conclusions drawn from this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online video
Footnotes
JY and QF contributed equally.
Contributors Substantial contributions to conception and design, acquisition of data or analysis and interpretation of data: JY, QF, AJW, LC, HS, WYL and YXJ. Statistical analysis: QF; JY and JYC. Drafting the article or revising it critically for important intellectual content: JY, QF and YL. Final approval of the version to be published: JY, QF, LC, HS, JYC, YXJ and YL.
Funding This work was supported by the National Natural Science Foundation of China (NSFC, Grant No. 81270989) and the Cutting-Edge Technology Combined PR Project of Shanghai Shen Kang Hospital Development Centre (Grant No. SHDC12012104).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance