Article Text

Abstract
Objectives To assess to which extent the COVID-19 pandemic affected corneal transplantation by virtue of donor selection algorithms in different European countries.
Design Survey.
Setting 110 eye banks in 26 European countries.
Participants 64 eye banks covering 95% of European corneal transplantation activity.
Interventions A questionnaire listing the number of corneas procured and distributed from February to May 2018–2020 was circulated to eye banks.
Main outcome measures The primary outcome was the number of corneal procurements. Additional outcomes were national algorithms for donor selection, classified according to their stringency (donors with COVID-19 history, suspected for COVID-19, asymptomatic, PCR testing) and the pandemic severity in each country. We calculated Spearman’s correlation coefficient to determine, two by two, the relationship between the 3-month decline in eye banking activity (procurement), the stringency of donor selection algorithm and the grading of pandemic severity (cases and deaths). A partial correlation was run to determine the relationship between decline and stringency while controlling for pandemic severity.
Results Procurements decreased by 38%, 68% and 41%, respectively, in March, April and May 2020 compared with the mean of the previous 2 years, while grafts decreased, respectively, by 28%, 68% and 56% corresponding to 3866 untreated patients in 3 months. Significant disparities between countries and the decrease in activity correlated with stringency in donor selection independent of pandemic severity.
Conclusions Our data demonstrate significant differences between countries regarding donor screening algorithms based on precautionary principles and, consequently, a decrease in the donor pool, already constrained by a long list of contraindications. Fundamental studies are needed to determine the risk of SARS-CoV-2 transmission by corneal transplantation and guide evidence-based recommendations for donor selection to justify their substantial medical and economic impact.
- epidemiology
- eye (tissue) banking
- infection
- public health
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author gilles.thuret@univ-st-etienne.fr.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Limiting the transmission of COVID-19 is a global priority that poses unparalleled challenges to corneal transplantation, one of the most common tissue transplant procedures performed worldwide. The WHO declared COVID-19 a pandemic on March 11, 2020, and the rapid spread of SARS-CoV-2 severely challenged health systems worldwide, including the delivery of organ and tissue transplant care by matters concerning donor screening and procurement, decisions to postpone or proceed with transplantation pending degree of emergency and entrenched healthcare services.
Despite the current lack of evidence that SARS-CoV-2 can be transmitted through corneal transplantation, and even though viral RNA could not be found in the cornea of patients who died from COVID-19,1 for life-enhancing procedures such as keratoplasty, the risk of transmitting a potentially fatal systemic disease is not acceptable.
Therefore, current recommendations in some countries call for the exclusion of tissues from donors recently infected with or exposed to COVID-19. This approach is appropriately based on precautionary principles. However, it increases the long list of contraindications (list given in the online supplemental appendix), and the already existing global shortage of donor tissue, where one donor is available for 70 patients in need.2 Therefore, it is essential to reach evidence-based and cost-effective screening strategies in which to resume corneal transplant programmes.
Supplemental material
This paper outlines the effect of the acute phase of the pandemic on corneal donation programmes and the different approaches taken across Europe based on precautionary principles. We analyse the impact of the various national strategies for donor procurement and transplantation and the relationship between pandemic severity and donor tissue procurement. Our overall aim is to contribute to a unifying approach, maintain corneal donor tissue availability and re-establish global corneal transplantation activity during and after the COVID-19 pandemic.
Methods
The study had two distinct parts. First, a questionnaire was disseminated to 110 eye banks in 26 countries, via the European Eye Bank Association (EEBA), to report eye banking activity between February and May 2020, compared with two previous years. The questionnaire is available in the online supplemental appendix. We calculated the overall decrease in corneas received by eye banks and the number of corneas assigned to recipients after the completion of the usual tissue selection process. We also asked when the competent/health authorities had established restrictions on procurement and whether the eye bank’s activity had been directly impacted by staff unavailability due to COVID-19 infection, family needs or having exercised their right to workplace withdrawal. The decrease in the number of corneas retrieved and corneas distributed was calculated as a percentage of the average in 2018 and 2019, bank by bank, country by country and collectively.
Second, official national guidelines for donor cornea selection (list of institute and agency are given in online supplemental appendix table S1)) and those of the European Center for Disease Prevention and Control (ECDC) were classified according to their stringency (table 1).
Method for classifying corneal donor selection algorithms
Data describing the severity of the pandemic in each country were also taken into account in the analysis. Data from EU/EEA and UK were collected from ECDC as of 3 June 2020 (https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea). Data for Switzerland up to 3 June 2020, were calculated from the ECDC download file (COVID-19-geographic-distribution-worldwide-2020-06-17.xlsx).
Graphic representations for the decrease in the number of corneas procured, the stringency of selection algorithms and the severity of the pandemic were established in the form of a heat map using Excel (Microsoft Excel workbook, conditional formatting tool). The colour green was assigned to the lowest levels (for decrease, stringency and mortality) and red to the highest.
The number of corneas collected from February to May 2020 was compared with the previous 2 years using a non-parametric Friedman test with repeated data. The non-parametric Kruskall-Wallis test was used to compare the decrease in number of corneas retrieved during the 4 months of 2020 compared with the mean of the previous 2 years. Post hoc analysis was performed using Dunn’s multiple comparison tests.
We calculated Spearman’s correlation coefficient to determine, two by two, the relationship between the 3-month decline in eye banking activity (procurement), the stringency of donor selection algorithm and the grading of pandemic severity (cases and deaths). A partial correlation was run to determine the relationship between decline and stringency while controlling for pandemic severity. Data were weighted by the number of corneas procured during the 3 months. Statistical analysis was performed using IBM SPSS Statistics V.23.0. (IBM Corp, Armonk, NY) with p<0.05 deemed significant with two-tailed tests.
Results
Representativity of this survey
Sixty-four eye banks covering 95% of the European corneal donation activity participated (online supplemental appendix table S2). This estimation was calculated using the number of corneas usually procured in the 110 eye banks of the same EEBA network and published yearly in the EEBA Annual Directory. The survey covered 83% of the eye banks registered with the EEBA and 43% of the eye banks identified by the European Union Tissue Establishment Compendium, which includes numerous small units with low or partial activity.
Decrease in overall eye banking activity
The number of procurements decreased by 38%, 68% and 41%, respectively, in March, April and May 2020 compared with the mean of the two previous years, while corneas assigned to a recipient (presumed to be grafted) decreased, respectively, by 28%, 68% and 56% corresponding to 3866 untreated patients in 3 months. The magnitude of the decrease is illustrated in figure 1. For reference, the same network of eye banks declared that 23 987 patients were transplanted in Europe in 2018 (2020 EEBA Directory, Venice).3
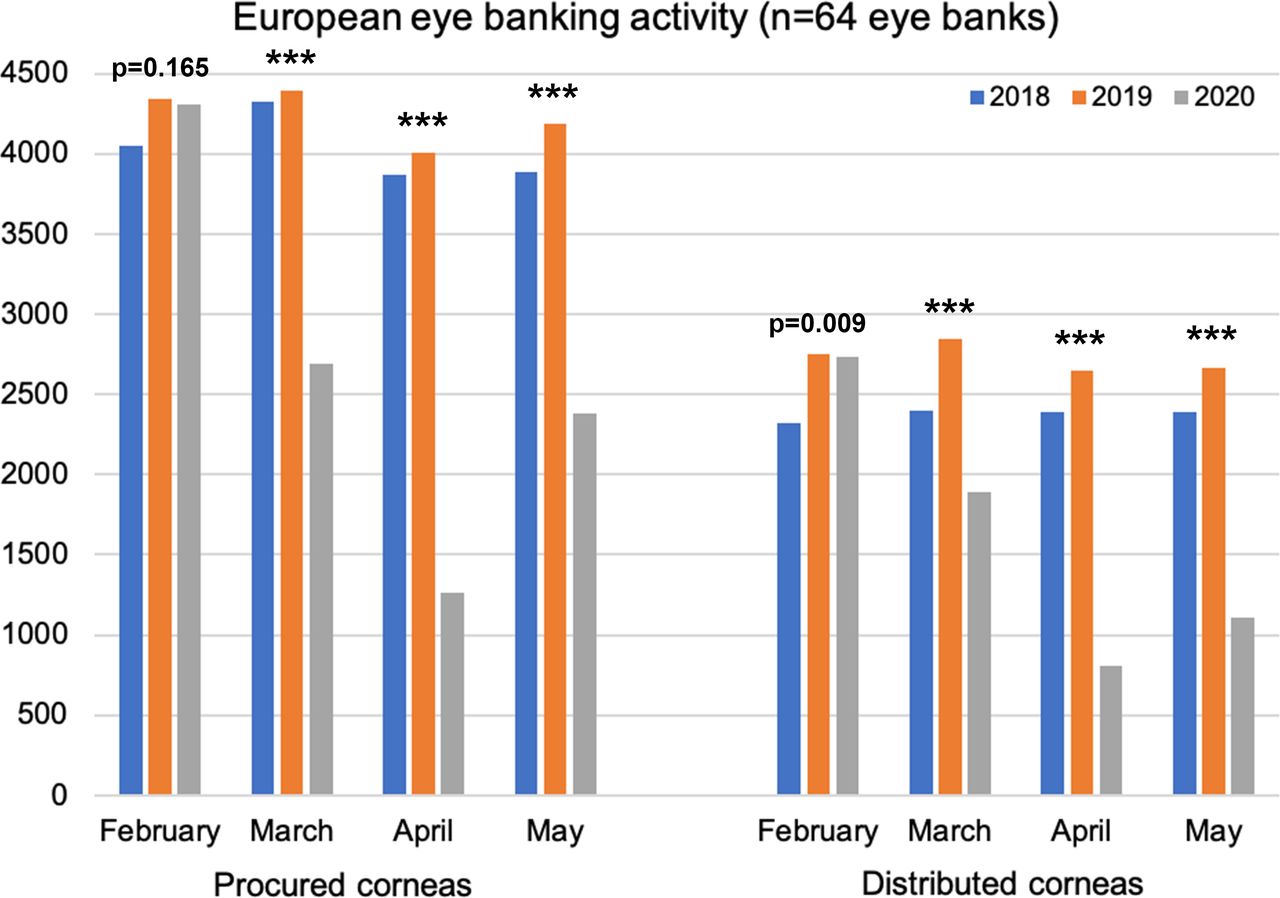
The decrease in the number of corneas procured and distributed per month from February to May 2020 compared with the two previous years. Due to very strict selection criteria regarding cell and tissue quality and microbiological safety, it is usual that a significant proportion of corneas cannot be grafted, which explains the difference between procured and distributed corneas. ***p<0.001.
Interbank variability
There were significant disparities between eye banks with extremes ranging from a total cessation of activity to a 200% increase (figure 2). Such increases were only observed in small eye banks with limited numbers of donors (eg, from three to nine donors).

Percentage change in the number of corneas retrieved by 64 European eye banks in February, March, April and May 2020 compared with the average of the previous 2 years. Box plots of the variation over months. Thick horizontal lines show the distribution median; boxes, the IQR; and individual points, outliers between 1.5 and 3 times the IQR. Whiskers mark the highest and lowest non-outlying values. Cross indicates the mean. The table indicates adjusted p values of paired comparisons.
Intercountry variability
There were significant disparities between countries ranging from an increase in activity (only for one country and a small number of corneas procured) to a considerable decrease of −81.2% compared with the same period in the two previous years, illustrated in figure 3A and detailed in table 2.

{kind=link}
{kind=link}
{kind=link}
(A) Heat map of the decrease in the number of corneas procured in March–May 2020 compared with the mean of the same trimester in 2018 and 2019, expressed in per cent. White figures indicate the number of corneas procured in this period in 2020. (B) Heat maps of the number of deaths from COVID-19 as of 3 June 2020, expressed in deaths per 100 000 inhabitants. It should be noted that there is still uncertainty related to differences between countries in the way deaths caused by/as a result of COVID-19 are reported. (C) Risk interpretation translated into national recommendations for corneal donor selection. Green is the least stringent, and red is the most stringent. Denmark, who changed its selection criteria during the studied period, is shown with the corresponding two colours. The ECDC recommendations of March (grade 9) and April 2020 (grade 5) are shown in the legend. The calculation of the grading is detailed in methods. Table shows correlation analysis (Spearman’s correlation coefficient). All were significant (p<0.01).
The decrease in the number of corneas procured and distributed in March–May 2020 compared with the mean of the same trimester in 2018 and 2019, expressed in per cent
Pandemic severity in different European countries
The decline in eye banking activity by country was put into perspective with the number of cases of inhabitants affected by COVID-19 and the number of deaths (figure 3B and online supplemental appendix table S3).
Variable interpretation of risk
A list of institutes and national agencies that produced donor screening algorithms is provided in the supplemental data (online supplemental appendix table S1). We did not obtain a response from one country, and no specific recommendation for tissue banking existed for another one. All countries contraindicated donations for patients who died of COVID-19. For the other potential donors, there were differences in selection criteria for (1) patients suspected to have COVID-19 but who died from another cause; (2) patients who recovered from COVID-19 and died later on from another cause; (3) asymptomatic patients at risk. For these three categories, the level of precautions ranged from automatic exclusion to retrieval if the PCR on nasopharyngeal swab was negative. The least stringent recommendation imposed a 14-day free interval between recovery and death or between last symptom and death, while the most stringent guidelines imposed a prolonged period of up to 28 days (double the incubation period). Definitions of symptoms compatible with COVID-19 also varied with the strictest recommendations excluding patients presenting with unexplained cough, unexplained asthenia and myalgia, intermittent fever, shortness of breath or unexplained conjunctivitis before death (without specifying whether any one of these isolated symptoms was sufficient to exclude). The definition of the risk for asymptomatic patients was also variable, especially the delay between death and last contact with a contaminating person or between death and return from a country/area with sustained COVID-19 transmission. Even the definition of a contaminating person varied from proven PCR+ cases to highly suspicious ones. The role of PCR testing on nasopharyngeal swab was also not standardised, ranging from mandatory PCR for all donors to the possibility to perform a PCR in case of COVID-19 suspicion (that we could qualify as rescue PCR). The possibility of utilising PCR results on nasopharyngeal swab performed antemortem was also not standardised among countries that recommended PCR. No country recommended PCR on conjunctival swabbing, on a saliva swab or the corneal storage medium. No country made serology testing mandatory. Only Italy recommended performing serology tests for epidemiologic reasons. Results are summarised in online supplemental appendix table S4 and illustrated in figure 3C.
Relationships between eye banking activity decline, stringency in donor selection and pandemic severity
All calculated correlations were significant, but the degree of association varied considerably (figure 3). Apart from the expected strong correlation between COVID-19 cases and COVID-19 deaths, the most significant association was found between the percentage decrease in procurement and stringency of national donor selection algorithms with rs=−0.844 (p<0.01). There was a strong, negative partial correlation between decrease in procurement (−38%±28%) and stringency (8±2) while controlling for COVID-19 death (33.7±21.1 death per 100 000 inhabitants), which was statistically significant, r(6186)=−0.688, n=6189, p<0.01. However, as mentioned above, zero-order correlations showed that there was a statistically significant and strong negative correlation between the decrease in procurement and stringency (r(6187)=−0.844, n=6189, p<0.01), indicating that COVID-19 deaths had very little influence in controlling for the relationship between the decrease in procurement and stringency. Note that most of the recommendations were established at the beginning of the pandemic before the severity was known.
Pandemic impact on eye bank staff
Two banks (in France and Germany) have temporarily halted their activity. Five banks (in Germany (a different bank from the previous one), Denmark, Portugal, Poland and the UK) reported reorganising their teams due to confinements, with limited personnel present on site. Two staff members (in Spain and the Czech Republic) were quarantined at home for COVID-19 confirmed by PCR. No infection of other team members was reported. Three banks (in Germany, Portugal and Poland) informed that part of their staff members had temporarily exercised their right of withdrawal, pending further information on work-related risks. Although the survey was not designed to investigate this limitation, two eye banks (France, Switzerland) spontaneously reported that they reduced their activity mainly because operating theatres for elective surgery were not available.
Discussion
This study shows the severe impact of the COVID-19 pandemic on corneal donation and transplantation activity in Europe between March and May 2020. As the pandemic advanced, healthcare systems issued guidelines for donor screening to balance the need for sight-saving procedures, while minimising the risk to patients and healthcare personnel. We found a wide variation in donor selection algorithms across Europe, ranging from clinical screening to molecular detection, and examined how this heterogeneity affected daily activity and corneal transplant programmes' recovery. We demonstrate the significant impact of complex and hypersecure algorithms on the breakdown of activity, even though no risk of transmission has formally been established to date.
It is well known that corneal transplantation can transmit pathogens that cause local disease, including herpes simplex virus,4 5 bacteria and fungi.6 Therefore, donor exclusion for a history of herpetic keratitis, which is highly prevalent in the general population and known to cause primary graft failure, is easy to justify. However, the cornea is not a suitable vector for transmitting systemic pathogens due to the absence of blood and lymphatic vessels and highly effective surface immunity.7 8 Furthermore, donor tissue is subject to effective pathogen reduction exposure protocol with povidone-iodine. Indeed, no transmission of HIV and hepatitis C viruses from seropositive donors has ever been reported.6 9 There is evidence of only two systemic transmissions, that is, rabies, a neurotropic virus with affinity to the richly innervated cornea,10 and hepatitis B.11 However, it is rather rare, as the number of reported cases can be counted on the fingers of one hand in almost half a century.
Nonetheless, serology and serum viral diagnostics remain mandatory for syphilis, hepatitis C virus (HCV), hepatitis B virus (HBV), HIV-1 and HIV-2 and human T-cell lymphotropic virus (HTLV) (in some countries only). In such cases, donor exclusion is based on the potentially devastating consequences to the recipient, even in the absence of evidence for transmission through corneal transplantation. Conversely, adenovirus in donors without active keratitis is not excluded due to the negligible impact on recipients despite a high prevalence in the population and an established role in keratoconjunctivitis.12 The nucleic acids of other viruses,13 such as CMV, can also be detected in eye bank stored corneal tissues without significant reactivation or infection risk in immunocompetent patients.14
The transmission of airborne respiratory pathogens via the cornea has not been reported to date. Influenza is capable of causing significant morbidity and mortality, can cause conjunctivitis and is detectable by conjunctival swabbing.15 Nonetheless, it is not a current exclusion criterion for corneal donation (except for death from uncontrolled disease). It should also be noted that death by bacterial sepsis is no longer an exclusion to cornea donation when stored in organ culture (the method of choice in Europe),16 which allows for additional microbiological testing before transplantation. Excluding potential donors with reported sepsis and airborne respiratory pathology as a cause of death would result in a significant loss of invaluable corneas for transplantation.
Ophthalmic manifestations were reported early on during the COVID-19 pandemic but are not in the forefront of clinical symptomatology.17 A case series from the Hubei province of China showed that 12 of 38 hospitalised patients (32%) experienced conjunctivitis symptoms, which occurred predominately in patients with severe systemic disease.18 Two of the 12 patients (17%) also had RT-PCR evidence of the virus in the conjunctiva, and both also had RT-PCR evidence of the virus in the nasopharynx (100%), compared with only 28 of the 38 patients (74%) tested. However, these findings should be interpreted with caution because the clinical diagnosis of conjunctivitis is often challenging in patients receiving respiratory support in an intensive care setting. Subsequent studies confirmed that coronavirus infection is rarely associated with conjunctivitis, with occasional cases reported in patients with established COVID-19 infection, along with isolated cases of conjunctivitis as a presenting sign.19 20 On the contrary, Arora et al 21 reported the presence of viral RNA in tears of one-fourth of patients with moderate to severe COVID-19 without conjunctivitis.
The risk of COVID-19 transmission through corneal grafts remains unknown. The entry of SARS-CoV-2 into host cells relies on the interaction between the viral spike (S) protein and the host cell ACE2 receptor.22 The expression of ACE2 on the ocular surface is controversial. It has been reported in a variety of ocular tissues, including the epithelium of the conjunctiva and cornea, and the aqueous humour where it may play a role in the intraocular renin–angiotensin system.23–27 However, the S protein interaction with corneal stromal cells is not described, and there is no evidence to support a clinically significant viral load within the corneal stroma. The theoretical risk of transmission relies primarily on viral persistence in the corneal epithelium with subsequent contamination of the nasopharynx via tears. However, it should be recalled that some of the corneal epithelium is shed during organ culture.28 Furthermore, the corneal surface is sterilised with povidone-iodine during or after procurement and is shown to be effective against SARS-CoV-2,29 and the majority of corneal transplants involve the selective replacement of the corneal endothelium only. Finally, the hypothetical viral transmission to other corneal cell types, especially endothelium, from ocular surface cells that resisted disinfection, seems unlikely. Endocular contamination would then have to be possible, which would be far from the pathophysiology of SARS-CoV-2.
The recommended diagnostic method for potential donor screening for SARS-CoV-2 infection is viral RNA detection in a nasopharyngeal swab specimen with real-time reverse-transcriptase PCR (RT-PCR).30 However, commercial testing systems are not validated for screening postmortem samples, and molecular testing is most likely not cost-effective. Although sensitivity in this setting remains to be determined, we endorse the use of validated RT-PCR testing to avoid systematic donor exclusion. We therefore propose that health authorities evaluate the role of conjunctival swab RT-PCR for this purpose. Our European consortium will collect data from countries that perform testing on some or all donors for 6 months to inform evidence-based screening recommendations.
Our results emphasise the striking impact of national regulations based on risk avoidance on donor procurement and transplantation activity compared with a modest relationship with pandemic severity. As the pandemic unfolded, the systematic exclusion of donors was appropriate, given its possible conjunctival involvement and potential life-threatening consequences. However, as we move forward, it may not be possible to avoid this large donor pool without compromising the sustainability of transplant programmes in Europe and the USA. Moreover, while the USA and most European countries are self-sufficient, stringent exclusion criteria are likely to jeopardise transplant programmes in countries relying on imports.
Transmission of SARS-CoV-2 in working environments is a recognised route that depends on the nature of work and the proximity of contacts.31 Precautionary measures in eye banks include specific training, hand hygiene, personal protective equipment, and disposable materials, draping and sterile preparation of the recovery area, and pathogen reduction with povidone-iodine, and appropriate ventilation system controlling airflow and exchange. Fortunately, tissue establishments have not reported any case of infection to date.
To the best of our knowledge, this is the first reported multinational assessment of the impact of COVID-19 on corneal transplantation and ensuing response by health authorities. Strengths include a very high response rate of 83%, reflecting a strong priority to understand COVID-19 better. Some limitations merit consideration. We cannot determine the relative contribution of elective surgery cessation on donor tissue procurement. However, only 2 of the 64 eye banks participating in this survey raised this possibility. Beyond the direct mortality caused by COVID-19, the numbers of out-of-hospital deaths, not related directly to COVID-19, may also have influenced corneal donation. Repeating this survey as confinement measures are relieved along with PCR data from tissue establishments will help answer this question.
In conclusion, as COVID-19 spreads rapidly across Europe, corneal donation and transplantation activity decreased dramatically. Based on current knowledge, the risk of COVID-19 transmission through corneal transplantation remains theoretical. While the exclusion of potential donors infected with or exposed to COVID-19 based on precautionary principles is appropriate at present, nevertheless, it considerably limits the pool of available donors already restricted by a long list of contraindications. Looking into the future, more evidence is needed to guide donor screening recommendations and justify their considerable societal and economic impact as the burden of COVID-19 becomes higher. As we face an imminent risk of a second global wave of the pandemic, our group proposes the following consensus recommendations for donor cornea screening, taking into consideration the evidence gained during the first wave:
Exclusion of donors with confirmed COVID-19.
PCR on nasopharyngeal swab at the time of corneal procurement for potential donors with a history of respiratory symptoms compatible with COVID-19.
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author gilles.thuret@univ-st-etienne.fr.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank all those European eye banks that kindly agreed to share their data. All contributors are listed in the online supplemental appendix. The authors also thank the European Eye Bank Association for its support in organising the survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GT, PG, MB, IM, CC, PM, JH, JSI, DP, SF, GJ, PR, KB, JA, FF, RN and MD were responsible for the conception and design of the study. GT and MD are the executive coordinators of the project. GT, DP, SF and GJ are responsible for the coordination of data acquisition. GT, EC and SP were in charge of statistical analyses and table and figure design. All remaining authors contributed to data acquisition and interpretation. The first draft was written by GT, EC, SP, CC, PM, JH, JSI, DP, GJ, PR, KB, JA, FF and MD. All authors contributed to data interpretation, critically reviewed the first draft and approved the final version and agreed to be accountable for the work.
Funding Supported by a grant from the Agence Nationale pour la Recherche call for proposal RA-COVID, CorDon Project: Corneal procurement during and after the SARS-Cov-2 pandemic What microbiological tests should be performed? What are the risks?
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- At a glance