Article Text

Abstract
Purpose To compare the long-term outcome of Aurolab aqueous drainage device (AADI) and Ahmed glaucoma valve (AGV).
Method Retrospective analysis of patients with refractory glaucoma who underwent AGV (AGV-FP7) and AADI (AADI Model 350) implantation. The outcome measures were intraocular pressure (IOP), requirement of antiglaucoma medications (AGMs) and re-surgery for IOP control. The postoperative complications were classified as early (≤3 months), intermediate (>3 months to ≤1 year) or late (>1 year).
Results 173 patients (189 eyes) underwent AGV implantation (AGV Group) while 201 patients (206 eyes) underwent AADI implantation (AADI group). The IOP in AADI group was significantly lower than AGV group at all time points till 2 years and comparable at 3 years. AADI group had significantly higher number of AGM in preoperative period and significantly lower number in postoperative period till 3 years compared with AGV group. AADI group had more hypotony-related complications but statistically insignificant (p = 0.07). The surgical interventions were significantly higher in AGV (n = 18) compared with AADI group (n = 5) in late postoperative period (p = 0.01). At 3 years, overall success was seen in 58.18% in AGV and 73.08% in AADI group (p = 0.15). Complete success was seen in 7.27% patients in AGV and 25.00% patients in AADI group (p = 0.02).
Conclusion Both AADI and AGV implant had comparable mean IOP at 3 years with lesser requirement of AGM in the AADI group. Both procedures appear to be safe with slight preponderance of hypotony-related complications in AADI group.
- Ahmed glaucoma valve
- Aurolab aqueous drainage implant
- intraocular pressure
- refractory glaucoma
Statistics from Altmetric.com
Manuscript
Glaucoma drainage devices (GDDs) are being increasingly used to manage patients with refractory glaucoma which require surgical intervention. They are employed more commonly as second line of management after failed glaucoma filtration surgery (GFS) that is, trabeculectomy with mitomycin C.1 2 More recently, they are increasingly being employed as a primary procedure in refractory glaucomas such as secondary to pars plana vitrectomy (PPV), penetrating keratoplasty, uveitis, neovascular glaucoma, etc.3 The rate of GDD implantation increased from 18% to 51%, whereas the rates of trabeculectomy decreased from 81% to 46% between 1996 and 2008, due to unpredictable wound healing and complications with trabeculectomy.3
The GDDs consist of a long tube which provides a channel for outflow of aqueous from the anterior chamber directly to equatorial plate which gets encapsulated later on and functions as a bleb.2 The devices are classified as valved and non-valved devices. Ahmed glaucoma valve (AGV; New World Medical, Rancho Cucamonga, CA, USA) is a commonly employed GDD device for intraocular pressure (IOP) control. The reported success rate of AGV implant varies from 60% to 85% depending on the follow-up period. These devices suffer from the limitation of small surface area and hypertensive phase.4 The Baerveldt glaucoma implant (BGI; Advanced Medical Optics, Santa Ana, CA) is a commonly employed non-valved GDD. It has a large surface area which promotes diffuse bleb formation. The pooled results of ABC study showed that the Baerveldt group had lower IOP with requirement of lesser number of medications and a lower failure rate but was associated with increased number of hypotony-related complications.5
Aurolab aqueous drainage device (AADI; Aurolab, Madurai, India) is a newer non-valved GDD modelled on Baerveldt prototype. It became commercially available for use in India in June 2013. The major advantage of the device is its low cost (US$50) compared with AGV implant (approximately US$250). There are only two studies available in literature which have compared the efficacy and safety of this novel implant vis a vis the established AGV implant in adults and have demonstrated comparable outcome in the two devices.6 7 These studies suffer from limitation of small sample size and a short follow-up period.
Due to its low cost, AADI has a great potential to be used in developing nations in management of glaucoma. This study compares the long-term outcome of the AADI with AGV implant.
Materials and methods
This was a retrospective analysis of patients with refractory glaucoma, requiring surgical intervention for the management of glaucoma. They presented to the tertiary care institute from June 2013 to January 2018. The study adhered to tenets of Declaration of Helsinki. The study was approved by Institute Ethics Committee and informed consent was obtained from all the participants before surgery. The records of patients were reviewed for various parameters like demography (age, sex and laterality), diagnosis/indication of surgery, history of failed filtration surgery, visual acuity, IOP, the number of antiglaucoma medication (AGM) before surgery, lens status and type of GDD. The patients were divided into two groups: the AGV group—patients undergoing AGV (AGV-FP7) implantation and the AADI group—patients undergoing AADI (AADI Model 350) implantation.
The patients younger than 18 years, patients with no perception of light or with previous cyclodestructive procedure/previous GDDs were excluded. The postoperative visual acuity and IOP were analysed at day 1, 1 week, 1 month, 3 months, 6 months, 12 months, 18 months, 2 years, 3 years and 4 years along with requirement of AGM/ additional surgery.
Surgical technique
Localised conjunctival peritomy was done, most commonly in superotemporal quadrant. The tenon was bluntly dissected till the equator. The implant (AGV/AADI) was inserted into the subtenon space. The two adjacent muscle bellies (most commonly superior and lateral rectus) were hooked and the lateral expansions of AADI plate were fashioned beneath them. The plate was fixed to sclera around 10 mm from limbus using 5–0 Dacron suture (Polyester, Green Braided, Alcon Laboratories, Fort worth, TX, USA). The tube of AADI was occluded tightly near tube plate junction using 6–0 vicryl suture (Braided-coated polyglactin 910 violet, Ethicon, Johnson & Johnson, India). The AGV implant tube was not occluded; it was primed using balanced salt solution to check for the patency of valve. A partial thickness track was created in the sclera by 23 G needle and entry was made into anterior chamber. The tube was trimmed to required length and was fashioned in the track to anterior chamber. The exposed part of tube was covered using sclera patch graft. The conjunctival peritomy was closed with 8–0 vicryl suture (Braided-coated polyglactin 910 violet, Ethicon, Johnson & Johnson).
The patients were prescribed topical antibiotics and steroids in tapering doses for 4–6 weeks. The AGMs were continued in the postoperative period in the AADI group for 3–6 weeks, when they were gradually tapered. In AGV group, all AGMs were stopped on first postoperative day and reintroduced as and when required.
Outcome measures
The success of GDD was defined as complete success if the IOP was >5 or≤21 mm Hg without requirement of AGM or if there was reduction of IOP by ≥20% from baseline without the use of AGM, qualified success if the above-mentioned IOP criteria was met with ≤2 topical AGM. The failure was labelled if the IOP criteria required >3AGM/use of systemic AGM, loss of perception of light or requirement of further surgical intervention for IOP control. The complications in the postoperative period were noted and classified as early (≤3 months), intermediate (>3 months to ≤1 year) or late (>1 year). Any episode of hypotony (≤5 mm Hg on a single visit) was noted. Persistent hypotony was defined as IOP ≤5 mm Hg on two consecutive visits after 3 months. The hypertensive phase was defined as IOP >21 mm Hg during the first 3 months after surgery (with or without AGM) after reduction of IOP to less than 22 mm Hg during the first postoperative week and not caused by tube obstruction, retraction or valve malfunction.8 Prophylactic AGM was introduced in AGV group in first 2 weeks if IOP was >12 mm Hg, to blunt the usual hypertensive phase.
Statistical analysis
The Statistical Package for the Social Sciences programme (IBM SPSS V.21.0 for windows, Chicago, IL, USA) was used for statistical analysis. Descriptive statistics were presented by mean±SD The normality of the data was checked using Shapiro-Wilk test. Wilcoxon signed rank test was used to compare the baseline and final parameters within the group while Mann-Whitney U-test was employed to compute significance between baseline and final follow-up parameters between the two groups. The qualitative variables were analysed using Fisher’s exact test and Pearson’s χ² test. ‘P value’ of <0.05 was considered significant. Kaplan-Meier survival analysis was performed to compare times to failure.
Sample size: Since it was a retrospective analysis, sample size was not calculated. The studies published in literature has shown 50% lesser requirement of medication in AADI group compared with AGV.7 Going by this and assuming 80% power, the sample size was calculated to be 15 eyes in each group.9
Results
In all, 173 patients (189 eyes) underwent AGV implantation (AGV group) while 201 patients (206 eyes) underwent AADI implantation (AADI group). All these patients completed 6-month follow-up. The baseline characteristics are highlighted in table 1.
Demographic profile and baseline characteristics of two groups
The demographic features such as age, sex, laterality were comparable in both the groups. The patients with previous history of failed GFS and cataract surgery were also comparable in both the groups (table 1). The mean follow-up was 27.41±18.81 months and 24.62±18.14 months in AGV and AADI groups, respectively. In all, 157 in AGV group and 151 eyes in AADI group completed 1-year follow-up. In total, 55 eyes in AGV group and 52 eyes in AADI group completed 3 years of follow-up (table 2).
Mean intraocular pressure and antiglaucoma medication (oral+topical) requirement in both groups at baseline and during follow-up
The indication of surgery was comparable in both the groups except that higher number of patients with primary open-angle glaucoma and patients with post-PPV underwent AGV implantation, whereas AADI was put in higher number in patients who developed glaucoma secondary to trauma (table 1).
Visual acuity
The mean best corrected visual acuity (logarithm of the minimum angle of resolution) was better in AGV group versus AADI group at baseline (0.62±0.26 vs 0.68±0.22, p=0.03) and at final follow-up (0.60±0.27 vs 0.66±0.24, p=0.02). There was no significant difference in the visual acuity in the two groups at baseline and final follow-up (p=0.25 in both groups). Two patients in each group lost perception of light at final follow-up.
IOP and AGM
There was significant reduction in IOP and AGM at all follow-up visits compared with baseline (p<0.01) in both the groups (figure 1). In AGV group, there was 50.38% reduction in IOP and 53.69% reduction in AGM at 1-year follow-up and 51.21% reduction in IOP and 47.54% reduction in AGM at 3-year follow-up. In AADI group, there was 59.31% reduction in IOP and 72.57% reduction in AGM at 1 year and 57.44% reduction in IOP and 68.14% reduction in AGM at 3-year follow-up.
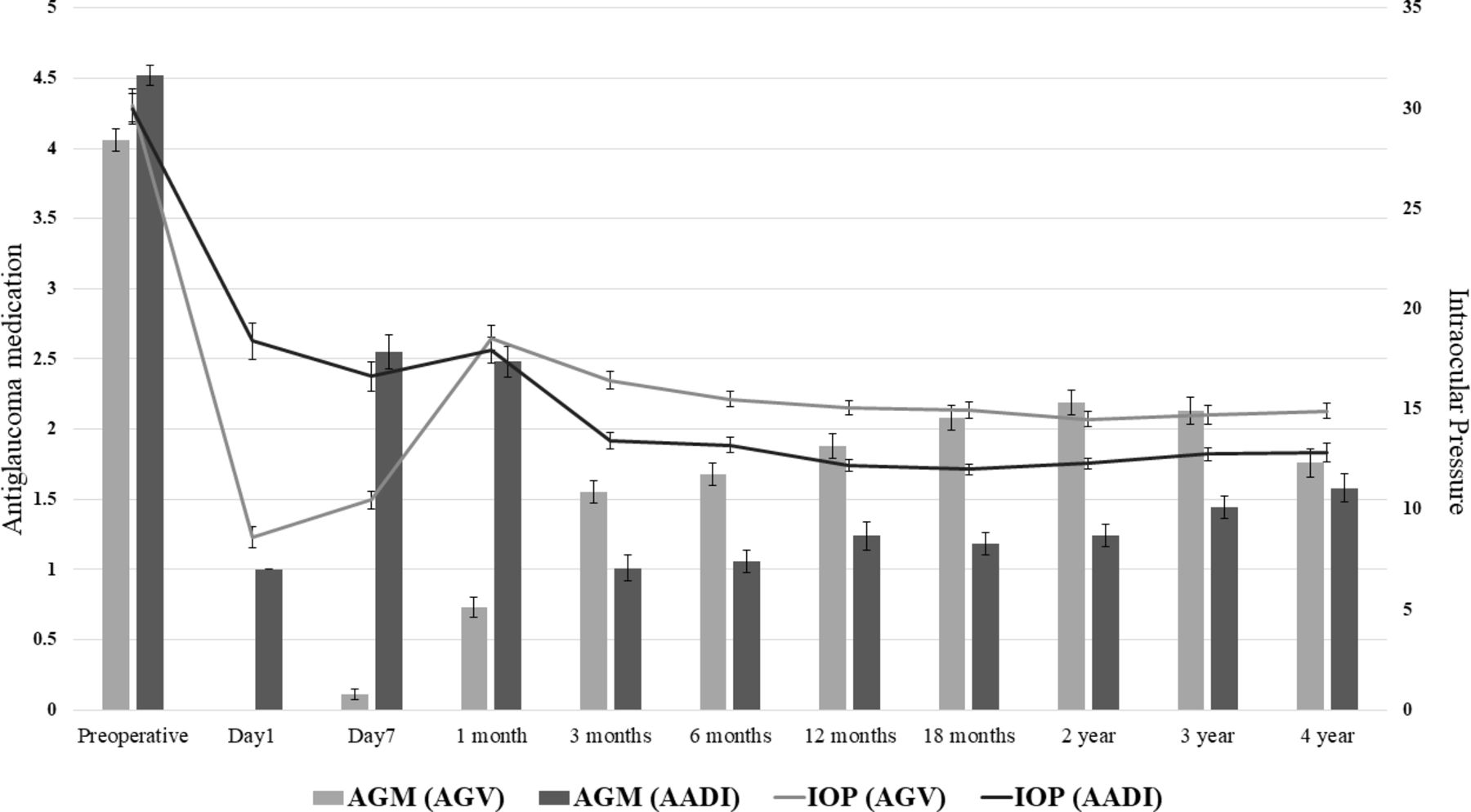
The trend of intraocular pressure and AGM in postoperative period in both the groups (error bars: SE of mean). AGM, antiglaucoma medication.
The IOP in AADI group was significantly lower than AGV group at 3 months, 6 months, 12 months, 18 months, 2 years and 4 years. AADI group had significantly higher number of AGM in preoperative period but it was significantly lower in postoperative period at all time points till 3 years and comparable at 4 years (table 2). Hypertensive phase was seen in 79 eyes (41.79%) in AGV group. Prophylactic AGM was started in 103 eyes (54.45%) in AGV group in first 2 weeks when IOP was >12 mmHg. Out of these 103 eyes, 21 eyes (20.39%) developed hypertensive phase. Hypertensive phase was seen in 58 out of 86 eyes (67.44%) in which no AGM prophylaxis was started. The early, intermediate and late complications in both the groups were comparable and are tabulated in table 3.
Complications and surgical interventions in both the groups in the postoperative period
In all, 38 eyes in AGV group and 40 eyes in AADI group developed hypotony in the early postoperative period. In all, 15 eyes in AGV group and 24 eyes in AADI group developed serous choroidal effusion in early postoperative period. Two eyes in AADI group developed serous choroidal effusion after 3 months. The serous choroidal effusion resolved with conservative management in all the patients except one which required choroidal drainage. Two patients in AADI group developed haemorrhagic choroidals which were drained surgically. Seven patients in AADI group developed persistent hypotony compared with one patient in AGV group (p=0.07). The AGV group required significantly higher number of surgical interventions for IOP control (14 diode laser cyclophotocoagulation (DLCP), 2 GDD capsule excision and two re-AGV) compared with AADI group (5 DLCP) in late postoperative period (p=0.01). The various other surgical interventions in both the groups were comparable and are tabulated in table 3.
At 1-year follow-up, complete success was seen in 11.46% and qualified success in 54.70% patients in AGV group (overall success 66.24%) while complete success was seen in 38.00% and qualified success in 45.33% patients (overall success 83.33%) in AADI group. The rate of overall success and complete success was significantly higher in AADI group (p<0.001). At 3-year follow-up, complete success was seen in 7.27% and qualified success in 50.91% (total success 58.18%) in AGV group while complete success was seen in 25.00% and qualified success in 48.08% (overall success 73.08%) in AADI group. Only the rate of complete success was significantly higher in AADI group at 3 years of follow-up (p=0.02).
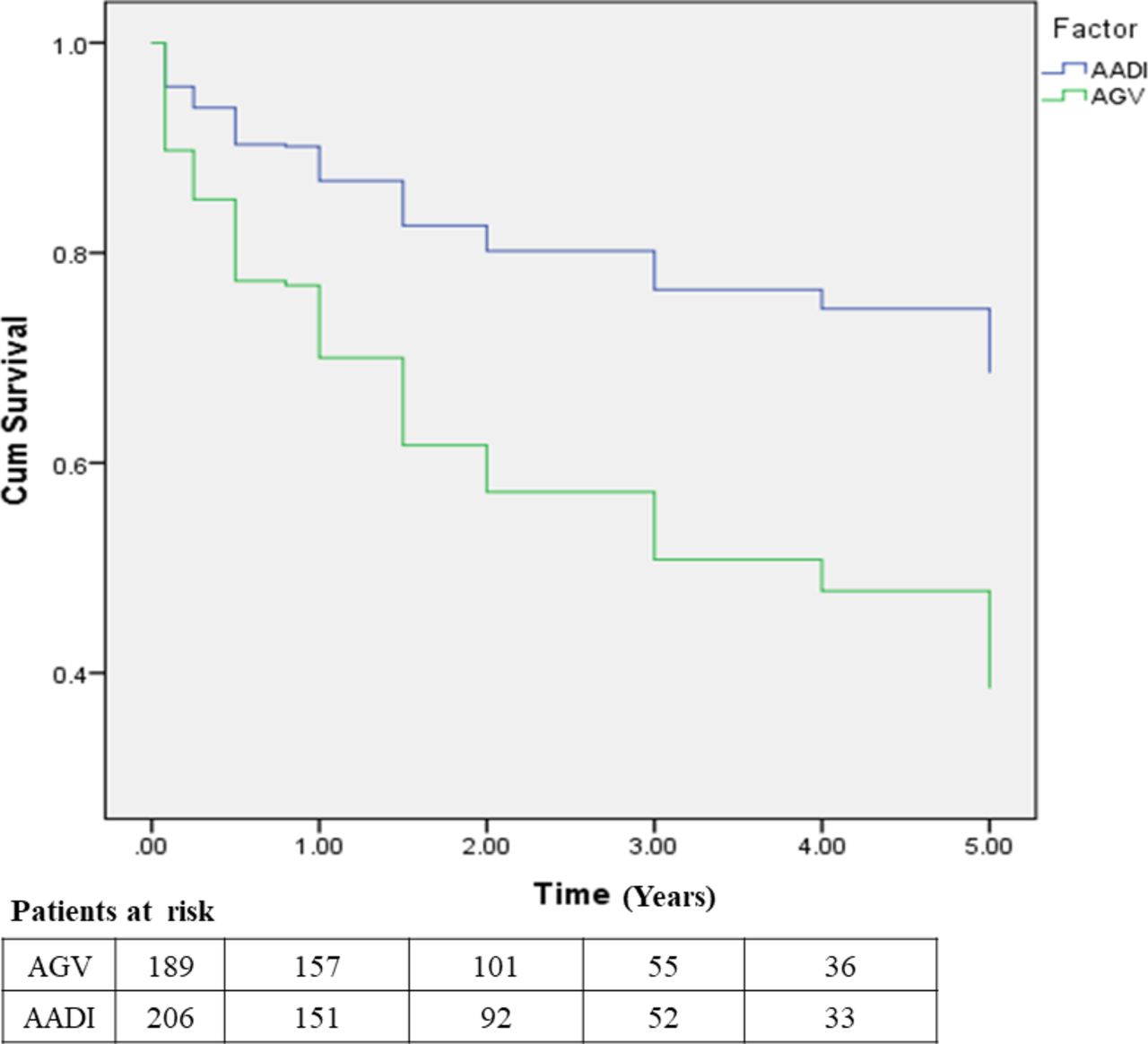
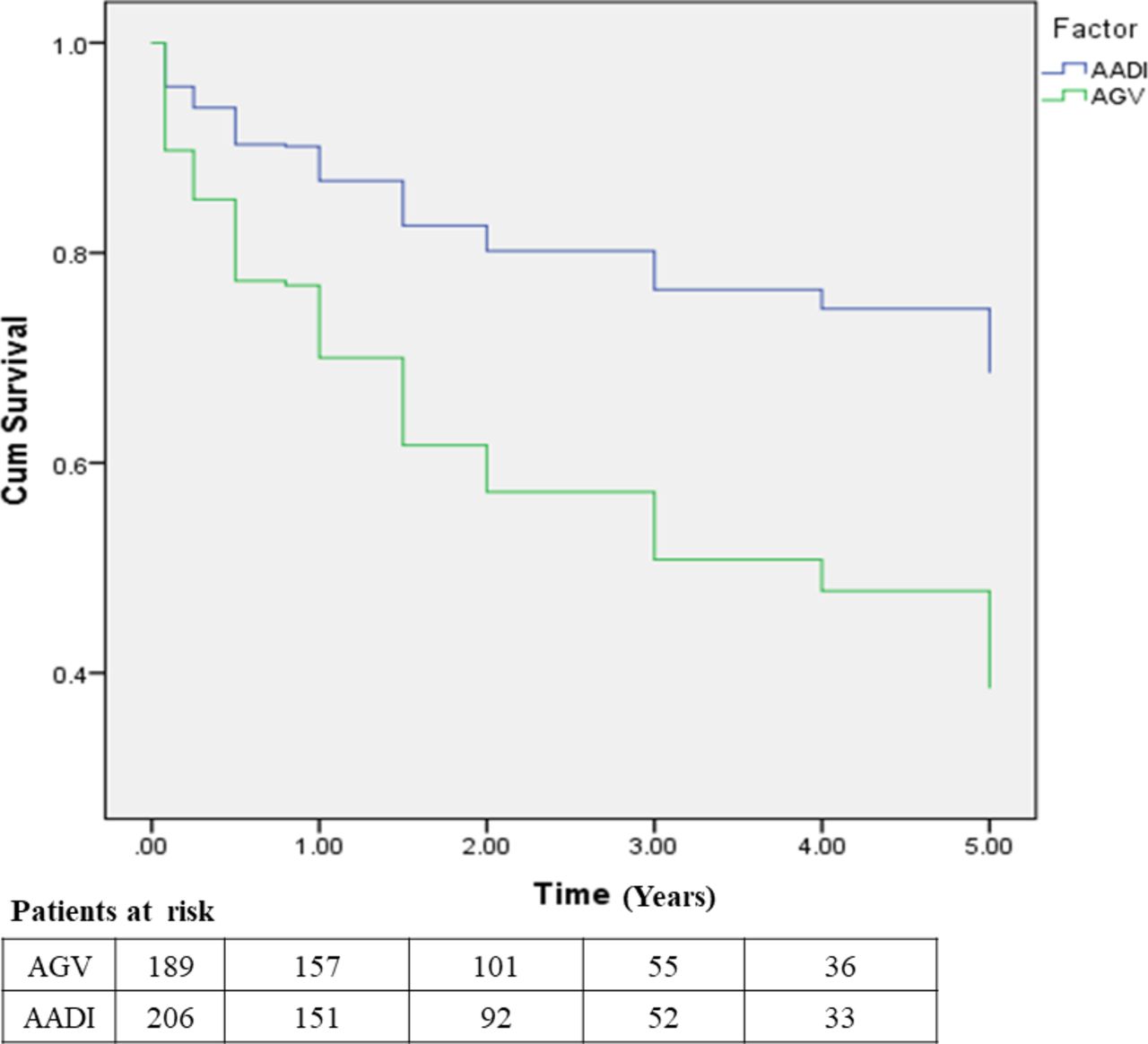
The survival probability of AGV group and AADI group at 1-year follow-up was 68.90% and 88.00%, respectively, and at 3-year follow-up was 50.40% and 77.00% respectively (p=<0.01) (figure 2).
{kind=link}
{kind=link}
The Kaplan-Meier survival plots in AGV group and AADI group, the failure was taken as end point. AADI, Aurolab aqueous drainage device; AGV, Ahmed glaucoma valve.
Discussion
The management of glaucoma in developing nations poses a lot of challenges. The patients often present at advanced stage and are at increased risk of progression to blindness.10 11 Moreover, according to global projections, the number of people with glaucoma will increase by 74% from 2013 to 2040, with highest impact in Asia and Africa.12 There is a need to develop comprehensive and cost-effective strategies to tackle the glaucoma burden, which is accessible and affordable to all sections of society in the developing nations. AADI is a novel, low cost indigenously built non-valved GDD, modelled on Baerveldt prototype (350 mm2 ).13 It is Conformité Européene approved and is available in some countries of Africa and South East Asia. It has shown good results at short-term follow-up comparable to the commonly employed AGV implant, which is a valved device.6 7 Our study demonstrates that AADI has comparable outcomes with higher number of complete success at both 1-year and 3-years follow-up as compared with AGV implant.
The key difference between AGV implant and AADI is their mechanism of functioning. AGV implant, being a valved device, starts functioning immediately because the valve opens up when a certain pressure gradient builds up in anterior chamber. The valved GDDs provide immediate reduction of IOP and maintain the anterior chamber in early postoperative period. Its advantage is immediate control of IOP with lesser chances of hypotony-related complications.14 This immediate hypotensive phase is followed by hypertensive phase which usually starts after 3 weeks.15 The hypertensive phase was seen in 41.79% of our patients. Mahdavi et al have reported an incidence of hypertensive phase in 56% eyes.8 We found decreased incidence of hypertensive phase in the patients who were started on early aqueous suppressant therapy (20.39% vs 67.44%). It was comparable to the study by Pakravan et al in which early aqueous suppressant therapy following AGV implantation showed better IOP control and lesser chances of hypertensive phase at 1-year follow-up (23.4% in treatment group vs 66% in no treatment group).16 It is suspected that since AGV implant allows immediate flow of aqueous from anterior chamber to subconjunctival equatorial plate, it also increases the exposure to inflammatory mediators which have been implicated in bleb encapsulation and long-term failure.17 18 Experimental data suggest that exposure to aqueous in the postoperative period leads to rapid decline in the porosity of bleb of glaucoma drainage implants.19 20 Since AADI is a non-valved implant, the tube is occluded at the time of implantation, with an absorbable suture; therefore, the flow of aqueous through the implant is delayed by 4–6 weeks, by that time implant is already encapsulated. The phenomenon of hypertensive phase is unusual after the non-valved implants owing to large surface area and presence of ligature which limit the flow in early postoperative period.8 21 The ligature degrades over a period of 4–6 weeks, a time when the capsule is formed around AADI. The downside of this is that immediate IOP reduction is not achieved in the postoperative period and the patients need antiglaucoma therapy for 4–6 weeks till the absorption of suture. The large surface area of the implant has been shown to be associated with better IOP control.22 23 AADI has a large surface area of 350 mm2 compared with AGV implant which has a surface area of 184 mm2. The IOP in AADI group was significantly lower with lesser requirement of AGM at all the time points from 3 months to 3 years. The AGV group underwent significantly higher number of surgical interventions for IOP control compared with AADI group (8.47% vs 2.43%, p=0.01). Five-year pooled analysis of Ahmed Baerveldt Comparison (ABC) and Ahmed Versus Baerveldt (AVB) studies also showed significantly higher requirement of number of glaucoma medications (AGV:2.3 vs BGI:1.2) and de novo glaucoma surgery in AGV group compared with Baerveldt group (AGV:19% vs BGI:6%).5
Irrespective of higher preoperative AGM, it was the AADI group which showed higher rate of complete success at 1-year and 3-year follow-up compared with AGV group (38.00% vs 11.46% at 1-year follow-up and 25.00% vs 7.27% at 3-year follow-up). The overall success was also better in AADI group than AGV group at 1-year follow-up (83.33% vs 66.24%) but was comparable to AGV group at 3-year follow-up (73.08 vs 58.18%). The other studies comparing the outcome of AADI and AGV implant in the first year have also shown higher rate of complete and overall success in AADI group.6 7 The overall success in the study by Pathak et al was 92.30% in AADI group versus 80.50% in AGV group at 1-year follow-up.7 AADI has also shown comparable outcomes with AGV implant in managing paediatric glaucoma at 1-year and 3-year follow-up.24 Souza et al have also reported the success rate of AGV implant to be 80.00% and 49.00% at 1-year and 5-year follow-up.25 Bouhenni et al found an overall success rates of 58.00% in Baerveldt implant at 5-year follow-up.26
The visual acuity in both the groups was comparable. Two eyes in each group lost perception of light at final follow-up. Most of the complications in both the groups were transient and managed conservatively. Transient postoperative hypotony was seen in 12.17% eyes in AGV group. Lai et al also found the transient postoperative hypotony in 10.80% cases in AGV group.27 The hypotony-related complications were higher in AADI group. Persistent hypotony was higher in AADI group (3.40%) compared with AGV group (0.53%) though this was statistically not significant. Two eyes (0.90%) in the AADI group developed haemorrhagic choroidals, which required choroidal drainage. Although statistically comparable, but AADI group developed more serous choroidal effusion (13.76%) than AGV group (7.93%). Pathak et al reported serous choroidal effusions in 3.80% in AADI group and 5.60% in AGV group.7 Tube exposure was more common in AADI group (3.40%) while rest of the complications were comparable in the two groups. All the patients with tube exposure had scarred conjunctiva (three had pre-existing buckle, 1 each had scarring secondary to trauma and failed multiple glaucoma surgeries). So this increased incidence could be due to patient factors than implant per se. Two patients in AGV group required capsule excision compared with none in AADI group. In the pooled analysis by Christakis et al, AGV implant had a higher rate of bleb encapsulation (AGV 60%, BGI 27%; p<0.001), whereas the Baerveldt group had higher rate of hypotony-related complications (AGV 4%, BGI 13%; p<0.05).5
The survival probability was significantly higher for AADI group at all the time points. To summarise, AADI implant showed a higher rate of complete success at 1 and 3 years of follow-up with requirement of fewer AGM and less frequent surgical interventions for IOP control than AGV implant. The hypotony-related complications were higher in AADI group (though statistically insignificant). AADI is a low-cost GDD which is equally efficacious alternative to the commonly used AGV implant as a management option to deal with refractory glaucoma.
References
Footnotes
Contributors SSP: Concept and design of work, critical revision of content, final approval of version to be published, accountable for all aspects of work in ensuring questions related to accuracy or integrity of any part of work are appropriately investigated and resolved. NGS: Data acquisition, analysis, preparation of manuscript. FT and MK: Data acquisition, preparation of manuscript. MA and AV: Data acquisition and interpretation. SK and SR: Revision of manuscript for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Linked Articles
- At a glance