Article Text

Abstract
Purpose To compare the efficacy of topical 1% voriconazole vs 5% natamycin for the treatment of fungal keratitis.
Methods In a prospective, double-masked, randomised, controlled, registered clinical trial, 118 patients with fungal keratitis were treated using identical dosage schedule with either voriconazole (58) or natamycin (60) as inpatients for 7 days and followed up weekly. The outcome measures were percentage of patients with healed or resolving ulcer and final visual acuity at last follow-up (primary) and on day 7 (secondary) in each group.
Results More patients (p=0.005) on natamycin (50/56, 89.2%) had healed or resolving ulcer compared with voriconazole (34/51, 66.6%) at last follow-up. The improvement in vision was marginally greater in patients in the natamycin group compared with the voriconazole group at day 7 (p=0.04) and significantly greater at final visit (p=0.01). In univariate analysis, drug, age and mean size of corneal infiltrate and epithelial defect had a significant effect on the final visual outcome. In multivariate analysis, the effect of drug (voriconazole vs natamycin, adjusted coefficient 0.27 (−0.04 to 0.57), p=0.09) was marginal while the effect of age and epithelial defect was significant (p<0.001 for both). In the group treated with natamycin, the final visual acuity was significantly better (p=0.005, Wilcoxon signed-rank test) in patients with Fusarium keratitis but not with Aspergillus keratitis (p=0.714, paired t test).
Conclusions When compared with voriconazole, natamycin was more effective in the treatment of fungal keratitis, especially Fusarium keratitis.
Trial registration number: Clinical Trial Registry India (2010/091/003041).
- Cornea
- Drugs
- Infection
- Microbiology
Statistics from Altmetric.com
Introduction
Fungi are responsible for 20–44% of keratitis in India.1 The prevalence of fungal pathogens in microbial keratitis has been reported to be 38% in Ghana, 36% in Bangladesh, 35% in southern Florida and 17% in Nepal.1 Currently, fungal infections of the cornea are difficult to eradicate as fungi often resist treatment. Amphotericin B and the azoles, ketoconazole and fluconazole, are generally not very effective against Fusarium and Aspergillus. Although natamycin is a good drug to treat fungal keratitis, treatment failures have been reported by several authors and the search for a better broad spectrum antifungal drug to treat fungal keratitis continues.2 In recent times, topical 1% voriconazole with or without oral administration has been shown to be effective in the treatment of refractory fungal keratitis caused by yeast as well as filamentous fungi.2 One of the advantages of topical voriconazole is its diffusion into the aqueous humour (0.61–3.30 mg/L after 1 h of topical administration).3 This level was above the minimum inhibitory concentration for Aspergillus fumigatus and Candida albicans.3 In most parts, the current literature suggests a promising role of voriconazole in the treatment of fungal keratitis, and given its better penetration, this drug is purported to be a superior alternative to natamycin. However, recently published clinical trials have reported equal or inferior efficacy of 1% voriconazole (reconstituted from injection vial) compared with 5% natamycin eye drops in fungal keratitis.4 ,5 These results are contradictory to experimental and in vitro data.6 ,7 Moreover, commercial 1% voriconazole eye drop has come into the Indian market recently and the availability of another potent topical antifungal drug in the market has its own benefits. The purpose of this study was to revisit the comparison of the efficacy of 1% voriconazole eye drops to 5% natamycin eye drops, in a randomised, masked, controlled trial, for the treatment of small-to-medium-sized fungal corneal ulcers with the hypothesis that subjects treated with voriconazole eye drops will have a non-inferior outcome compared with subjects treated with natamycin.
Materials and methods
The study was conducted at three tertiary centres of L V Prasad Eye Institute located in three different cities of India—Hyderabad, Bhubaneswar and Visakhapatnam—between November 2010 and December 2012. The study coordinator (SS) provided common protocol, case record forms and randomisation list to all study centres. Each centre had an ophthalmologist, microbiologist, pharmacist and study nurse to execute the study. All patients with suspected microbial keratitis seen in the cornea clinic of these hospitals were considered for inclusion in the study. The trial was stopped when the required number of patients was recruited.
Inclusion and exclusion criteria
Patients with age ≥18 years, able to understand and sign the informed consent form, and either men or women with duration of complaints not more than the past 14 days before presentation to the study centre were included in the study. All included patients were required to have the presence of a corneal epithelial defect with stromal infiltrate or exudate, clinically suggestive of fungal ulcer with or without hypopyon. The widest diameter of the ulcer needed to be between 2 and 6 mm as long as there was no scleral involvement. It was mandatory that only patients with corneal scraping positive for fungal filaments in direct smear examination by any one or more of the methods used be recruited. At the time of recruitment, either none or inadequate prior treatment with antifungal eye drop (less than six times per day) and absence of foreign body on the cornea was required. If present, the subject was enrolled after the foreign body was totally removed and the other enrolment criteria were met.
Patients having history of allergy to voriconazole or natamycin were excluded from the study. Other exclusion criteria included patients with impending or actual corneal perforation, presence of scleral involvement or involvement of posterior one-third stroma, legally blind unaffected eye, presence of dacryocystitis, presence of other comorbidities such as corneal anaesthesia, exposure or dry eye and patients who received/required topical or systemic steroids or other immunosuppressants (unless discontinued before randomisation). Patients who were known to be HIV-positive or diabetic, whose corneal infiltrate extended into the posterior one-third of the stroma, whose initial corneal culture showed significant growth of bacteria (>10 colonies) or who were on any topical antifungal agent that had been used in adequate dosage (four hourly) within the past one week or those who had bilateral infection, were excluded.
Laboratory investigations
Corneal scrapings were collected using blade no. 15 on Bard Parker handle, under topical anaesthesia on the slit lamp and smeared on glass slides and inoculated on culture media in the clinic and brought to microbiology laboratory. The smears were stained with Gram stain and 10% potassium hydroxide with 0.1% calcofluor white for direct microscopy. Table 1 shows the culture media inoculated and the incubation conditions. Any bacterial growth was identified using API system (bioMérieux, France) and fungal identification was based on colony characteristics and microscopic features. All media were held for 2 weeks in case of no growth before declaring the sample as sterile. Only unequivocal or significant culture results were considered as described earlier.8
Culture media inoculated and the incubation conditions for the processing of corneal scrapings
Masking, randomisation and treatment
The treating ophthalmologist, microbiologist and patients were masked to the drug by using similar vials. The study pharmacist provided the drugs. The patients were randomised (by SS) using computer-generated randomisation blocks (http://www.randomization.com) into one group receiving 1% voriconazole eye drop (Aurolab, Madurai, India) and the other group receiving 5% natamycin ophthalmic suspension eye drop (USP 5% Natamet, M.J. Pharmaceuticals, Mumbai, India). No systemic antifungals were given, and the subjects were hospitalised for 7 days and discharged on the same randomised medication that they were assigned while hospitalised. They were asked to follow-up weekly.
The dosing schedule of both medications was identical—day 1–3: one drop topical medication every hour round the clock; day 4: one drop hourly while awake, every three hours when asleep; and day 5 and after: one drop every two hours while awake until cured.
Sample size
Sixty subjects in each of the two treatment arms were required with 80% probability that the study would detect a one-sided 0.05 significance level if the true difference between the treatments was 5.0 units.
Outcome measures
Assessed at the end of 1 week and at last follow-up visit, the outcome measures were response to medical treatment in the form of healed keratitis, resolving keratitis or worsening keratitis and visual acuity (logarithm of the minimum angle of resolution (logMAR)). An ulcer was defined healed if epithelial defect diameter reduced to ≤1 mm associated with the complete absence of stromal infiltrate, plaque and satellite lesions. A corneal ulcer characterised by reduction of size of stromal infiltrate size by at least 1 mm and/or density of infiltrate and/or decrease in endothelial plaque or satellite lesions was classified as resolving keratitis. An ulcer was deemed to demonstrate no response or worsening if there was lack of improvement or worsening in inflammatory sign scores or stromal infiltrate dimensions or corneal melt and deterioration in any clinical examination factor. Best-corrected visual acuity was recorded at the follow-up visits.
Patients requiring surgical interventions such as tissue adhesive for impending perforation, superficial keratectomy, penetrating keratoplasty and evisceration were considered as treatment failure.
Statistical analyses
All statistical analyses were performed using the R software (V.2.12). Means with SDs were reported for normally distributed continuous variables and median with IQR were reported for non-parametric data. The χ2 tests were used to compare categorical data and t test and Wilcoxon rank-sum and Wilcoxon signed-rank tests were used to compare continuous data. Visual acuity at three time points for patients in both groups were compared by multiple comparisons of means from a mixed effect model with Dunnett contrasts. Adjusted p value was obtained by Bonferroni method.
A univariate linear regression was carried out to evaluate the relationship between the final visual acuity (primary outcome measure) with regard to fungal species, drug, follow-up, age, gender, mean corneal infiltrate size and mean size of corneal epithelial defect. A multivariate linear regression model with stepwise elimination using Akaike information criteria (AIC) was used to assess the association between the final visual acuity and the independent variables.
Results
The total number of patients in the voriconazole group was 58 while 60 patients received natamycin.
Comparison of baseline clinical and microbiological parameters between the patients recruited in the voriconazole and natamycin groups
A comparison of baseline clinical and microbiological findings of the two groups is given in table 2. The type of fungi isolated from patients in both groups is shown in table 3.
Fungal species grown from corneal scrapings of 44 fungus culture-positive patients in the voriconazole group and 46 culture-positive patients in the natamycin group
There was no significant difference between the groups in terms of mean age, gender, mean presenting infiltrate size, presenting visual acuity and type of fungal species grown. Mean follow-up was 26 (15 to 38.5) and 21 (10.33) days in the natamycin and voriconazole groups, respectively. Despite the frequency of healed or resolving ulcers being similar on day 7 (natamycin 35/54, 65%; voriconazole 34/50, 68%), at the final visit the percentage of patients who had healed corneal ulcer were significantly higher in the group treated with natamycin (50/56, 89.2% vs 34/51, 66.6%; p=0.005).
Out of the 18 patients who worsened in the voriconazole group, 11 were switched over to natamycin (figure 1). The ulcers healed in 10 of 11 patients, with 1 patient proceeding to penetrating keratoplasty. All remaining patients required surgical intervention (penetrating keratoplasty in three, superficial keratectomy in one and evisceration in one) and two patients were lost to follow-up. There was no difference between the groups in the number of patients who either did not improve or marginally worsened on day 7 (natamycin 19/54, 35%; voriconazole 18/50, 36%). Patients on natamycin were continued on natamycin. While the ulcer healed or was resolving in 15 patients, 2 patients required keratoplasty and 2 were lost to follow-up.

Flow chart depicting the outcome of all patients included in the study. LTFU, lost to follow-up.
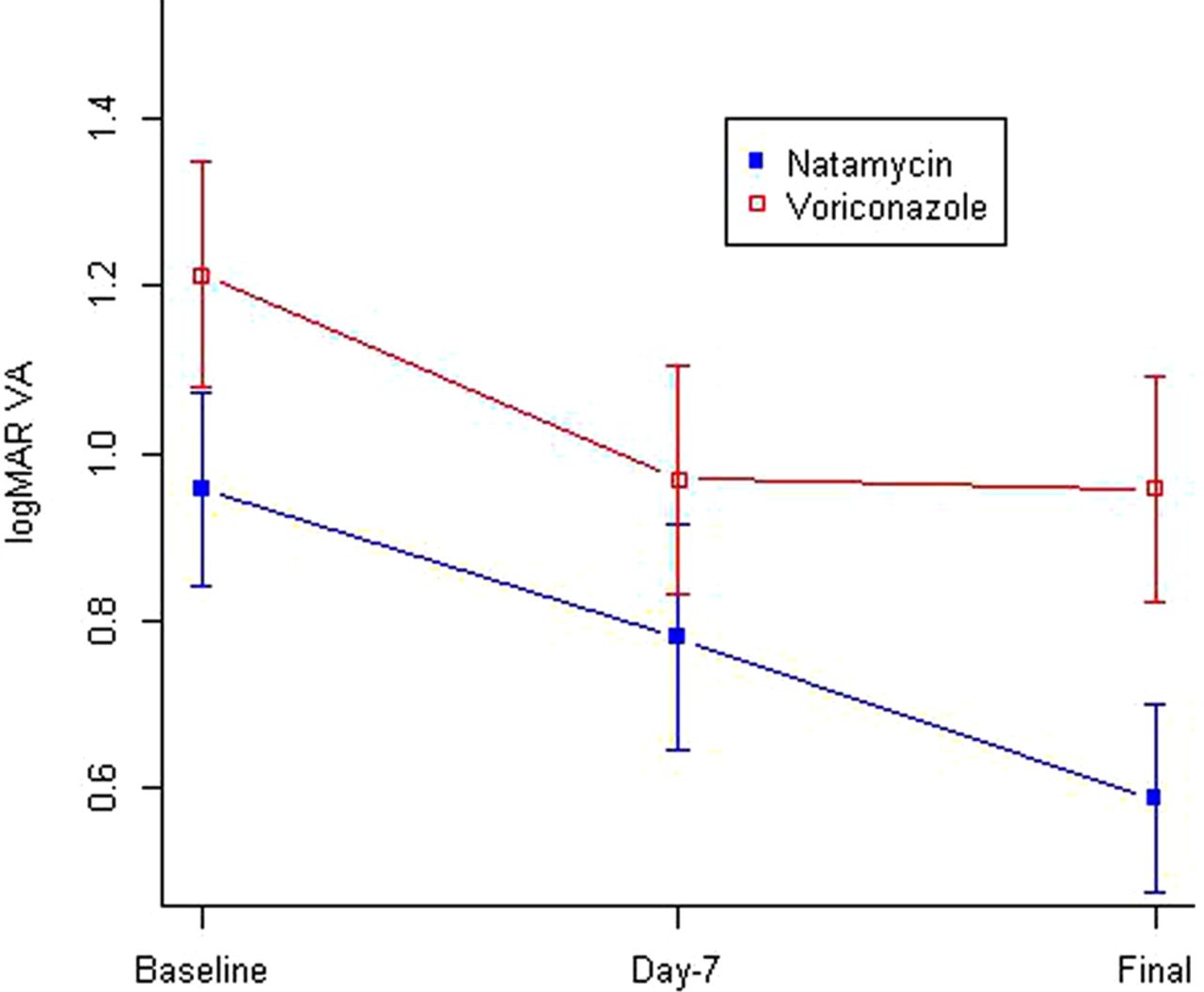
Figure 2 compares the visual acuity of the patients in the two study groups at baseline, day 7 and final follow-up visit. Using Wilcoxon signed-rank and Wilcoxon rank-sum tests for non-parametric data, the visual acuity was compared between the two drugs at the three time points. There was no difference in the baseline visual acuity (p=0.19) of the patients in the two groups; however, the improvement in vision was marginally greater in patients in the natamycin group compared with the voriconazole group at day 7 (p=0.04) and significantly greater at the final visit (p value 0.01). Within the voriconazole group, the visual improvement compared with baseline was significant at day 7 (p value 0.01) as well as at the final visit (p value 0.02). On the other hand, initial insignificant improvement at day 7 (p value 0.16) became highly significant at the final visit (p=0.001) in the natamycin group (figure 2).

{kind=link}
{kind=link}
Comparison of best-corrected visual acuity of baseline, day 7 and final follow-up visit of patients in the voriconazole and natamycin study groups. logMAR, logarithm of the minimum angle of resolution; VA, visual acuity.
On univariate analysis (table 4), the following factors were associated with significantly better visual acuity: drug, age, mean corneal infiltrate size and mean size of corneal epithelial defect. The lesser the age, the better the visual outcome (p<0.001). Similarly, the lesser the mean corneal infiltrate and epithelial defect size, the better the vision (p<0.001 and <0.001, respectively).
Regression table showing association of various factors with final visual acuity in multivariate and univariate analyses (n=118)
In multivariate regression analysis (table 4), we built a model with the independent factors (fungal species, drug, follow-up, age, sex, mean corneal infiltrate size and mean size of corneal epithelial defect) followed by stepwise elimination using the AIC. The final model retained drug, age and epithelial defect size as significant factors affecting visual outcome in fungal keratitis. After adjusting with other cofactors, the natamycin group showed a marginally better outcome (p=0.09) compared with voriconazole. Similarly, with final visual acuity as a dependent variable and drug, age and epithelial defect as the independent variables, the latter two remained significant (p<0.001 for both).
In a subanalysis of the group treated with natamycin, the final visual acuity was significantly better than pretreatment visual acuity (p=0.005, Wilcoxon signed-rank test) in patients with Fusarium keratitis. Although the numbers were small, such a difference was not seen in patients with Aspergillus keratitis (p=0.714, paired t test).
Discussion
This study reiterates the findings of two previous studies published in 2010 and 2013 from India.4 ,5 The former study found no difference in visual acuity, scar size and perforations between the two fungal keratitis groups treated with voriconazole and natamycin. The latter study reported significant better clinical and microbiological outcomes in the natamycin-treated group compared with voriconazole, with difference specifically seen in patients with Fusarium keratitis. Both studies used reconstituted parenteral preparation of 1% voriconazole and commercially available 5% natamycin eye drop. We evaluated a commercial eye drop of 1% voriconazole against a commercial eye drop of 5% natamycin with results similar to the former study in multivariate analysis and similar to the latter study in univariate analysis. Our study reaffirms the results obtained in the previous studies that go in favour of natamycin. In addition to analysing visual outcome at day 7 and final visit, we also analysed the change in corneal infiltrate size at day 7 and final visit. It was interesting to note that after 7 days of therapy there was no difference (voriconazole 18/50, 36%; natamycin 19/54, 35%) in the number of patients whose corneal ulcer either did not respond or worsened on medical treatment. However, as per the protocol, on worsening, 11 patients in the voriconazole group were switched over to natamycin. Although the visual acuity at day 7 had initially improved in marginally greater number of patients on voriconazole, it plateaued thereafter and the visual improvement was significantly higher in the natamycin group (figure 2). On the same lines, surgical intervention was more often required (voriconazole in six and natamycin in two) in patients treated with voriconazole.
Response to natamycin topical therapy was significantly better in patients with Fusarium keratitis, a finding similar to Prajna et al.5 We could not show such a response in patients with Aspergillus keratitis but are unable to accept this as true effect due to the smaller number of isolates in each group (natamycin in eight and voriconazole in seven). Contradictory reports exist in the literature regarding the response of Fusarium and Aspergillus keratitis to monotherapy with 5% natamycin.9 ,10 While Prajna et al found Aspergillus infection to be a predictor of poorer outcome,9 Jones10 reported Fusarium to be more destructive. However, compared with Aspergillus spp., in vitro susceptibility of Fusarium spp. to natamycin is indeed reported to be better and this may reflect in the in vivo response. In the face of the argument that factors other than susceptibility of the fungus contribute to the outcome in fungal keratitis,11 ,12 we would like to submit that this study had reasonably good control of the confounding factors such as duration of symptoms, age, gender, baseline visual acuity, size of corneal infiltrate and size of corneal epithelial defect, and we believe that the superior effect of natamycin is acceptable, especially in Fusarium keratitis. Apart from final visual acuity, using the measure of efficacy of a drug as reduction in size of corneal infiltrate and healed ulcer at last follow-up, this study found significantly better results with natamycin.
Despite strict implementation of inclusion criteria and intensive medical therapy under supervision for at least one week, two patients in the natamycin group required keratoplasty. This outcome reiterates the fact that medical treatment of fungal keratitis needs further research to find effective antifungal drugs. Until then it seems that natamycin is the drug of choice for the treatment of filamentous fungal keratitis, leaving the choice of voriconazole as the second best.
There is increasing trend of using topical, stromal, as well as oral voriconazole in the treatment of fungal keratitis, and given its excellent penetration in the cornea, it is considered superior to natamycin by many.13–19 With the current availability of commercial voriconazole eye drops, it is likely to be used more often, especially because it is only marginally more expensive than natamycin (250.00 rupees vs 118.00 rupees). A survey published in 2009 indicated that physicians would prefer to use voriconazole over natamycin if it were to be commercially available.20 Unpublished reports of high efficacy of intrastromal injection in deep-seated corneal infiltrates in fungal keratitis are often presented in meetings, although a recent study did not find it particularly useful.19 The study, however, recommends topical voriconazole to be used as an adjunct therapy along with natamycin in the face of no response to monotherapy with natamycin.19 Synergistic action of natamycin and voriconazole is an interesting aspect to explore in future studies.
References
Footnotes
Contributors SS: concept, design, data analysis, microbiology investigation, manuscript preparation and final approval of manuscript. SD, MF, SKS and PG: patient treatment, data collection, surgery and final approval of manuscript. AV: data collection, data analysis and final approval of manuscript. NKK and SRM: microbiology investigation, data collection and final approval of manuscript. MHA: statistical analysis.
Funding Hyderabad Eye Research Foundation (HERF), Hyderabad and Aurolab, Madurai. While HERF provided the infrastructure and financial support, Aurolab provided the voriconazole eye drops.
Competing interests None.
Patient consent Obtained.
Ethics approval Institutional Review Board of L V Prasad Eye Institute, Hyderabad Eye Research Foundation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All clinical and microbiology raw data pertaining to all subjects included in the study are available with the corresponding author (SS). Final format of all data used for statistical analysis and all comparisons are available with the biostatistician (MHA).