Article Text

Abstract
Background/Aims To compare several methods of macular hole measurement using optical coherence tomography (OCT), and to assess their predictive capability against anatomical and visual outcomes in a single cohort of patients.
Methods A retrospective study of 50 eyes undergoing standardised macular hole surgery. All patients underwent preoperative OCT scanning with measurement of macular hole inner opening diameter, minimum linear diameter, base diameter and macular hole height. Values were calculated for the macular hole index and the tractional hole index.
Results Logistic regression analyses indicated that the preoperative base diameter, macular hole inner opening and minimum linear diameter were associated with both anatomical and visual success. Derived parameters as alternatives to these basic ophthalmic parameters add little to the modelling of either anatomical or visual success.
Conclusion Base diameter, macular hole inner opening and minimum linear diameter can each be used to predict anatomical and/or functional success in macular hole surgery. Preoperative base diameter is the most useful variable in this regard, as it holds the strongest association with anatomical and visual outcome and is easily measured on a OCT scan.
- Base diameter
- macula
- macular hole
- OCT
- retina
- sulphur hexafluoride
- trauma
- vitreous
Statistics from Altmetric.com
The first description of macular hole surgery using intraocular gas to tamponade the hole predated the popular use of optical coherence tomography (OCT) scanning by only a few years. Once OCT became available in outpatient clinics, attempts were made to assess hole measurements and predict surgical success. Several authors have described different methods of macular hole measurement using OCT scans, including minimum linear dimension (MLD),1 hole form factor (HFF),2 macular hole index (MHI),3 diameter hole index (DHI)4 and tractional hole index (THI).4
This study aimed to compare some of these methods of macular hole measurement and regress them against anatomical and visual outcomes in a single cohort of patients.
Materials and methods
A retrospective consecutive case series study of 50 eyes from 50 patients (16 men, 34 women) with idiopathic stage II (n=8), stage III (n=38) or stage IV (n=4) macular hole was performed. Cases were operated on by one surgeon (RR) between May 2009 and January 2011, with at least 3 months postoperative follow-up. The sample size resulted from the availability of data from a consistent surgical technique over a 20-month period. Patients with traumatic macular holes, high myopia and previous macular surgery were excluded from the study.
Preoperative data included patient age, gender, best corrected visual acuity (BCVA), stage of macular hole and axial length. Preoperative and postoperative BCVA was measured using a standard Snellen acuity chart and converted to LogMAR scores for the purposes of statistical analysis. Preoperative biometry was performed on all patients using the Zeiss IOLMaster version 5.4 (Carl Zeiss Meditec, Dublin, California, USA). OCT scanning was performed using the Optovue RTVue-100 with version 4.0 software (Optovue, Fremont, California, USA). Twelve radial 6 mm OCT images (MM6/radial slice 0.27 s) through the centre of the macular hole were obtained. Preoperative OCT scans were analysed retrospectively by one researcher (RR) to avoid interobserver variation. Measurements of the hole were made using the following parameters: macular hole inner opening diameter, minimum linear diameter, base diameter and macular hole height. Values for the HFF, MHI and THI were derived from these data as shown in figure 1.
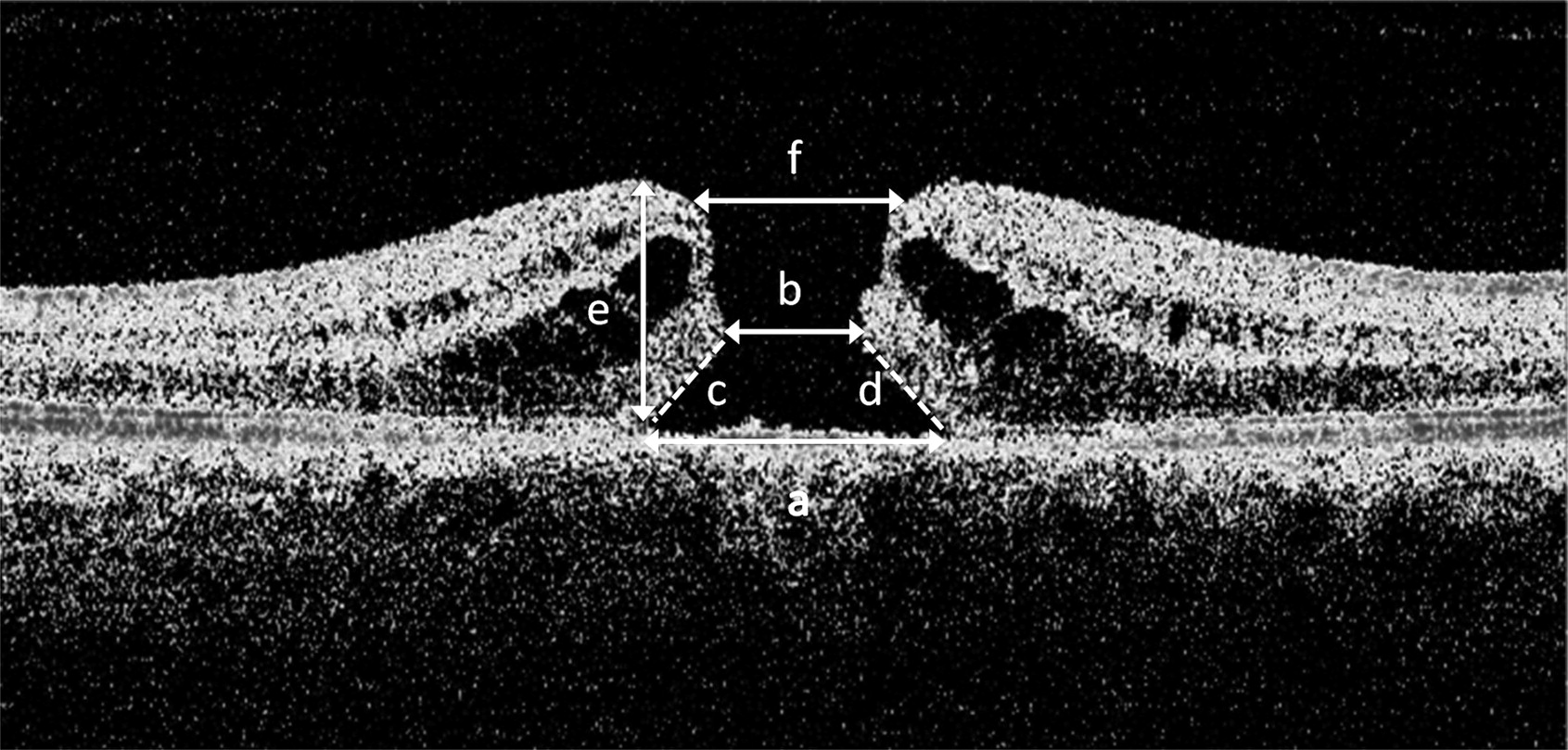
Optical coherence tomography scan measurements: (a) base diameter, (b) minimum linear dimension, (c) and (d) arms for measuring hole form factor, (e) hole height, (f) macular hole inner opening. Hole form factor = (c+d)/a; macular hole index = e/a; tractional hole index = e/b.
Patients underwent transconjunctival, sutureless 23-gauge vitrectomy, phacoemulsification with intraocular lens implantation, internal limiting membrane peel with brilliant blue G staining and endotamponade with 20% sulphur hexafluoride. All patients received a standard postoperative protocol of topical antibiotic and anti-inflammatory agents. Both face-down and supine posturing were actively discouraged.
Patients were examined at 2 weeks, 6 weeks and 3 months, receiving fundus biomicroscopy and OCT to assess closure of the hole. Holes were considered closed, indicating anatomical success, if there was complete circumferential hole rim reattachment without foveal neurosensory retinal defect demonstrated on OCT. This was taken as the primary outcome measure. A secondary outcome measure of ‘visual success’ was defined as a postoperative visual acuity of 0.3 logMAR or less (better than or equal to 6/12, excluding 6/12 ‘part’) at up to a year postoperatively, in order to remain consistent with other UK studies.5 ,6 At the 3-month postoperative visit, patients were discharged if they achieved a BCVA of 6/12 or better. Patients not achieving this level of vision were followed up for longer until 6/12 was achieved, or for a year postoperatively, because best spectacle-corrected visual acuity (BSCVA) has been shown to improve up to and beyond a year postoperatively.7 Patients whose macular holes had failed to close were successfully closed with further surgery.
Statistical analysis
Statistical analysis was undertaken using IBM SPSS for Windows, V.18.0. Demographic variables corresponding to age (in years) and sex, plus several ‘basic’ ophthalmic parameters: axial length (mm), macular hole inner opening (μm), MLD (μm), hole height (μm) and base diameter (μm) were included in the analysis. The dimensionless derived variables MHI (defined as hole height/base diameter) and THI (defined as hole height/MLD) were also included in the analysis. The dimensionless parameter HFF was also considered as a candidate explanatory variable. However, the parameters MHI and HFF, both of which are derived from base diameter and a parameter relating to the height of the hole, exhibit near-extreme collinearity and so little insight would be gleaned from separate analyses of these two variables. Therefore, as evaluation of MHI was considered to be of primary interest in the current analysis, the HFF index was not considered further in subsequent analyses.
Binary logistic regression analyses were derived, using anatomical success and visual success as the outcome measures. Receiver operating characteristic (ROC) curves were derived for variables indicating good model discrimination, assessed by the area under the curve: values close to 1.00 represent good discrimination, whereas values close to 0.500 indicate that the model does not discriminate to any greater extent than that achieved by random allocation.
The ROC curves may also be used for the identification of cut-off values of success probability corresponding to optimum sensitivity and specificity. In the current study, the avoidance of ‘false positives’, that is, the erroneous prediction of the key measure of anatomical success, was considered to be of paramount importance. Therefore, optimum discrimination was considered to be represented by the value of the test variable corresponding to maximum sensitivity, given 100% specificity.
Due to the non-linear relationships between the derived variables and the basic ophthalmic parameters, and high correlations between variables, multiple logistic regression analyses were not derived.
Results
Summary of data
The mean age of patients was 70.5 years (range 50–85 years, SD 7.53 years). Preoperative LogMAR visual acuities ranged from 0.30 to 1.90 (mean 0.778, SD 0.282). One patient was pseudophakic before surgery; the other 49 received phacoemulsification and intraocular lens implantation at the time of macular hole surgery. None had visually significant cataract before surgery. Eight patients had a stage II macular hole, 38 patients had a stage III hole and four patients had a stage IV hole. Axial lengths ranged from 22.05 mm to 26.58 mm (mean 23.51 mm, SD 1.08 mm).
Macular hole closure was achieved in 42 patients (84%). The remainder required a second procedure using heavy silicone oil without prone posturing. Postoperative LogMAR visual acuities ranged from 0.00 to 1.78 (mean 0.425, SD 0.397). Postoperatively, 35 eyes (70%) achieved 6/12 or better Snellen acuity. Four eyes (8%) had a reduction in visual acuity after primary surgery, three of which had holes that failed to close, and one who was lost to follow-up after 3 months. The follow-up period varied between 3 and 12 months (mean 5.36 months, SD 2.27 months).
Considering the available basic ophthalmic variables: the mean axial length was 23.5 mm (SD 1.08 mm); the mean base diameter was 654.8 μm (SD 284.4 μm); the mean macular hole inner opening was 485.8 μm (SD 142.3 μm); the mean MLD was 379.6 μm (SD 148.1 μm); and the mean hole height was 374.0 μm (SD 91.32 μm). Considering the derived ophthalmic variables: the mean (dimensionless) MHI was 0.673 (SD 0.336); and the mean (dimensionless) THI was 1.107 (SD 0.467).
Outcome measure: anatomical success
Logistic regression analyses considering each of the demographic and ophthalmic parameters determined that the basic ophthalmic parameters base diameter, macular hole inner opening and MLD, plus the derived parameter MHI, were significantly associated with anatomical success (table 1). The areas under the ROC curves corresponding to each of these variables indicated that these parameters could be used as effective predictors of anatomical success (figure 2). Basic parameters generally exhibited stronger association and better model discrimination than was exhibited by MHI.
Assessment of variables associated with anatomical success
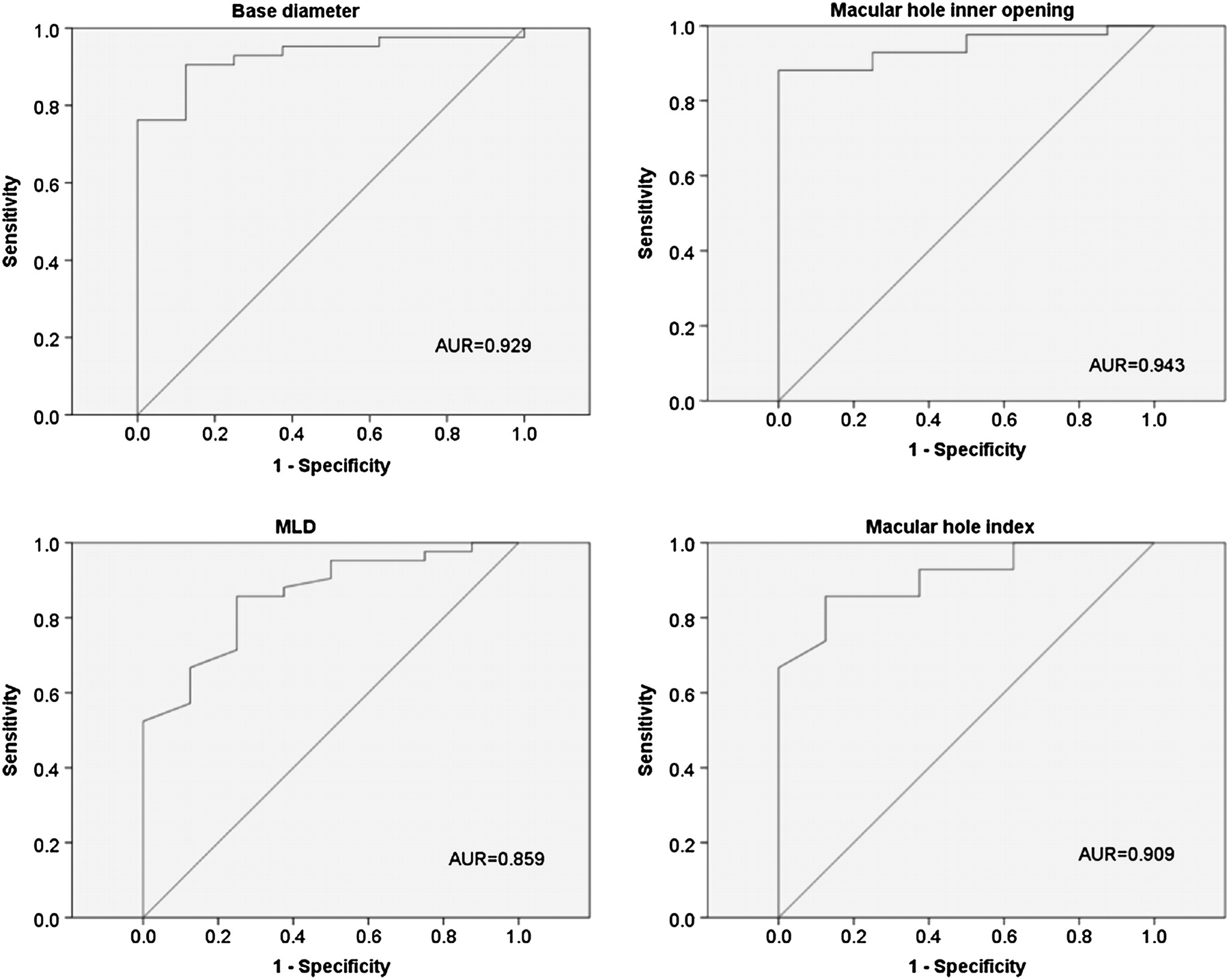
Receiver operating characteristic (ROC) curves for base diameter, macular hole inner opening, minimum linear dimension (MLD) and macular hole index (outcome measure anatomical success). AUR, area under ROC curve. Diagonal segments are produced by ties.
Other ophthalmic and demographic variables were not found to be significantly associated with anatomical success, and were found to exhibit inferior levels of model discrimination.
Outcome measure: visual success
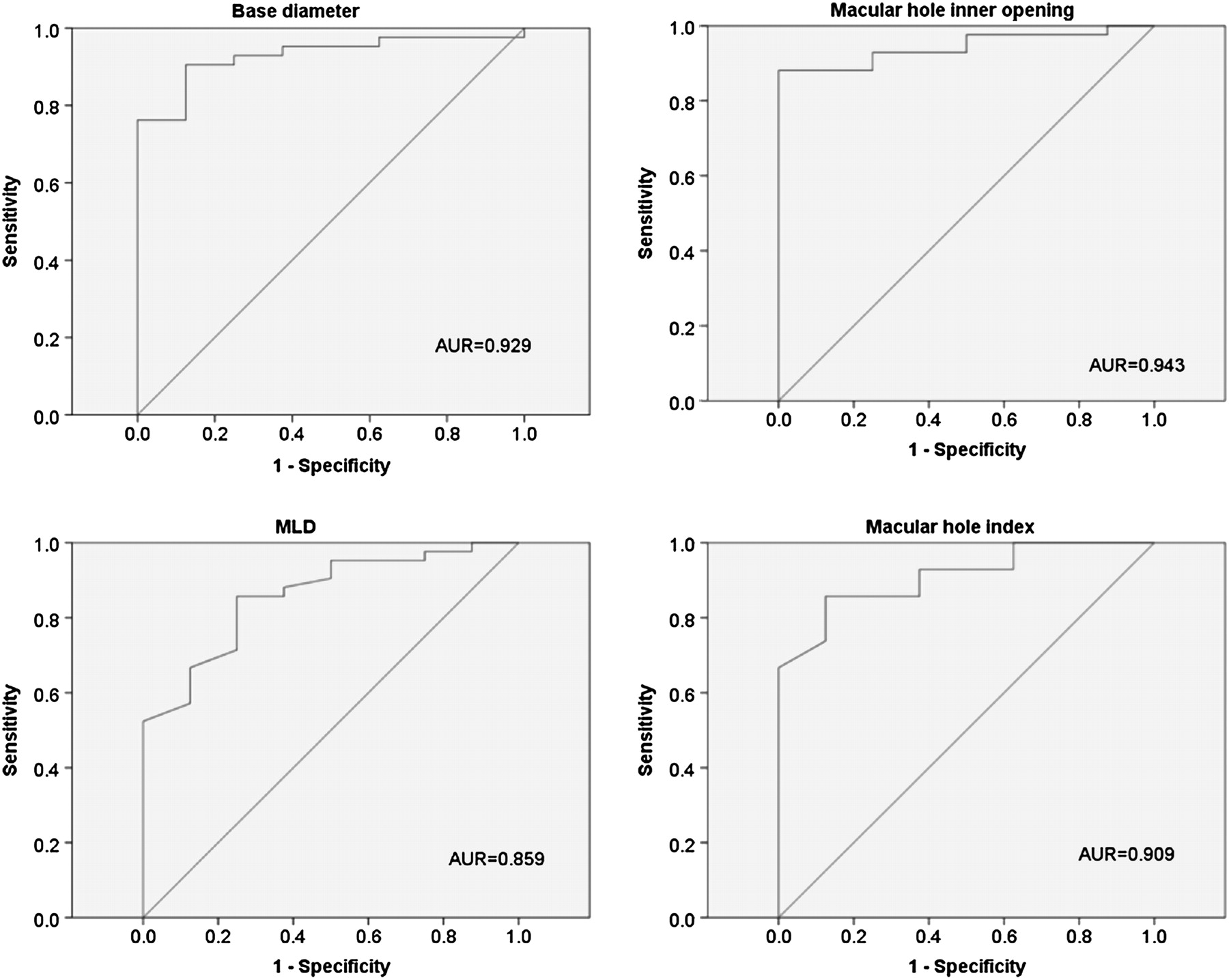
Logistic regression analyses considering each of the demographic and ophthalmic parameters determined that the basic ophthalmic parameters base diameter, macular hole inner opening and MLD, plus the derived parameters MHI and THI, were significantly associated with visual success (table 2). The areas under the ROC curves corresponding to each of these variables indicated that these parameters could be used as fairly effective predictors of visual success (figure 3). Other ophthalmic and demographic variables and derived ophthalmic parameters were not found to be significantly associated with visual success, or to exhibit good model discrimination.
Assessment of variables associated with visual success

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves for base diameter, macular hole inner opening, minimum linear dimension (MLD), macular hole (MH) index and tractional hole index (outcome measure visual success). AUR, aea under ROC curve. Diagonal segments are produced by ties.
Discussion
The first study to use OCT to analyse macular holes preoperatively was published by Ip et al1 in 2002. Continuing on from the original Gass classification,8 which itself uses biomicroscopic estimation of macular hole size to distinguish stage II from stage III holes, these authors used OCT measurement of the least horizontal diameter of the macular hole to aid classification of the hole into less than 400 μm (stage II) and greater than 400 μm (stage III). Using a series of logistic regression analyses they found that anatomical closure was associated with macular hole diameters smaller than 400 μm. Given the limitations imposed by OCT resolution at this time, this measurement was the most easily reproducible one. It has been named the MLD or the ‘maximum minimum linear dimension’ taking into account the need for accurate selection of an OCT image that represents the true extent of the hole. Significant correlations between MLD and visual outcomes after macular hole surgery have been described.6
At around the same time, Ullrich et al2 presented data based on measurement of the HFF. This made use of the base diameter measurement as well as the overlying tissue dimensions in a derived trapezium shape (figure 1). However, as the MLD may be measured at varying heights within the same scan, and the right and left arms are usually diagonally orientated, it is difficult to reproduce the measurements accurately. These authors found no correlation between HFF and postoperative gain in lines, or between base diameter and MLD and postoperative gain in lines. MLD was a better predictor of anatomical success than HFF. However, postoperative visual outcome was demonstrated to be positively correlated with a higher HFF value.
In 2004, Kusuhara et al3 formulated the MHI, defined as the ratio of the macular hole height to the base diameter. They wished to demonstrate a method of measurement that would represent the putative tangential and anteroposterior vitreomacular traction or retinal hydration thought to be acting on the fovea and causing the macular hole to develop. In addition, in calculating the MHI as a ratio, they were able to avoid the influence of axial length measurement on transverse measurement dimensions. They found a significant correlation between MHI and postoperative macular thickness, and the MHI was associated with postoperative BSCVA in a logistic regression analysis.
Two further indices were described by Ruiz-Moreno et al4 in 2008. The first, the DHI, was defined as the ratio of the minimum diameter of the macular hole to the base diameter. The authors proposed that the DHI indicates the strength of the tangential traction at the fovea. They observed that the minimum diameter may equal the base diameter if the tangential traction reaches its maximum. No correlation between DHI and BSCVA at 3 months postoperatively was found. The second, the THI, was defined as the ratio of the maximal height of the macular hole to the minimum diameter. The authors proposed that the THI represents the two tractions responsible for the macular hole, and is the ratio between the anteroposterior vitreomacular traction and/or retinal hydration, and tangential traction. THI was found to correlate significantly with postoperative BSCVA at 3 months.
To our knowledge, this study is the first to compare these different methods of macular hole measurement in the same cohort of patients. The indices HFF, MHI and THI were originally proposed in order to reflect changes in macular morphology and tractional forces thought to be acting upon the macula during hole formation. However, our results indicate that there is no real advantage to be gained by calculating derived indices from the basic ophthalmic measurements.
The logistic regression analyses of the current study indicated that the basic ophthalmic parameters base diameter, macular hole inner opening and MLD are associated with both anatomical and visual success, and exhibit good discrimination with respect to either outcome measure. A reasonable alternative measure for the prediction of anatomical and visual success is the derived variable MHI, which is also associated with both of these outcome measures and exhibits comparable model discrimination to the basic ophthalmic parameters with respect to either outcome measure. The alternative derived variable THI is statistically significantly associated with visual success only, and exhibits inferior model discrimination with respect to either outcome measure than either MHI or the basic ophthalmic parameters. Overall, model discrimination using visual success as the outcome measure is substantially inferior to that using anatomical success as the outcome measure.
Of the basic ophthalmic measurements, MLD exhibited the lowest level of model discrimination with respect to the key outcome measure of anatomical success, and macular hole inner opening is probably the hardest variable to measure reliably and consistently. We therefore suggest that the base diameter is the strongest contender when considering which variable to use as a predictor of anatomical or functional success in macular hole surgery. The choice of base diameter seems sensible when one considers that this parameter—the hole at the level of the retinal pigment epithelium—is itself the basic retinal lesion being treated.
One potential limitation of this study is the relatively small sample size. However, by restricting analysis to univariate models, simulation studies9 indicate that our regression coefficients will not be biased using this sample.
From the ROC curve corresponding to anatomical success using the base diameter parameter, optimum discrimination may be obtained with a value of 747.5 μm, corresponding to 76.2% sensitivity and 100% specificity. Holding specificity at 100%, sensitivity of over 70% may be obtained from a range of base diameter values of 721.0 μm to 747.5 μm.
From the ROC curve corresponding to visual success using the base diameter parameter, 100% specificity may be obtained only at the expense of low sensitivity. Under this constraint, sensitivity cannot exceed 11.4%, which may be achieved with a base diameter value of 286.5 μm. A specificity level of 80% may be obtained only with a corresponding sensitivity of under 43%.
The best estimate OR for base diameter correspond to a 10% reduction in the odds of anatomical success for every 13 μm increase in base diameter; and a 10% reduction in the odds of visual success for every 26 μm increase in base diameter.
In this cohort of patients, macular hole surgery involved peeling of the internal limiting membrane and gas tamponade using 20% sulphur hexafluoride in all cases. In the future, an alternative treatment strategy could be planned in those patients with higher base diameter measurements, for example, using a longer-acting gas tamponade or the use of a postoperative posturing regime, in order to improve the chances of anatomical and functional success.
Footnotes
Competing interests None.
Ethics approval This study was a retrospective analysis of OCT images acquired in the course of the standard treatment of macular hole, with no alteration in normal patient management.
Provenance and peer review Not commissioned; externally peer reviewed.