Article Text

Abstract
Aims To compare the ability to detect cystoid macular edema (CME) and its late complications between spectral-domain optical coherence tomography (SD-OCT) and fluorescein angiography (FA).
Methods Retrospective, observational, case series. 85 Eyes who had FA and SD-OCT performed on the same day at first visit and/or at follow-up visits were included. FA and SD-OCT images were evaluated for the evidences associated with CME and other structural changes of macula. FA and SD-OCT images were then superimposed to determine the relationships of diagnostic features between the two images. Main outcome measure was the correlation between FA and SD-OCT findings of macula in patients with CME.
Results The common causes of CME in our study were retinal vein occlusion (RVO, 63%), diabetic retinopathy (DR, 21.18%) and posterior uveitis (3.53%). CME associated with RVO, age-related macular degeneration and DR were missed by FA in 18.52%, 33.33% and 33.33% of cases, respectively. Subretinal fluid was undetectable by FA in 54.55%, which mainly were in the RVO group. SD-OCT gave earlier CME diagnosis than FA in three (3.53%) eyes. Residual CME at follow-up visits were missed by FA in one (1.18%) eye. Late complications of long-standing CME (secondary macular hole (two eyes), secondary subretinal fluid (five eyes), retinal pigment epithelium detachment (one eye) and photoreceptor atrophy (one eye)) were detectable only by SD-OCT.
Conclusions SD-OCT demonstrated greater sensitivity than FA in detecting CME, particularly those associated with RVO, DR and age-related macular degeneration. SD-OCT was also more sensitive than FA for detecting subretinal fluid and late complications of long-standing CME.
- Cystoid macular edema
- fluorescein angiography
- optical coherence tomography
- diabetic retinopathy
- retinal vein occlusion
Statistics from Altmetric.com
- Cystoid macular edema
- fluorescein angiography
- optical coherence tomography
- diabetic retinopathy
- retinal vein occlusion
Cystoid macular edema (CME) is a common pathological condition of the macula that is the result of cystic accumulation of extracellular intraretinal fluid in the outer plexiform and inner nuclear layers of the retina, as a result of breakdown of the blood-retinal barrier.1 Common causes of CME are postsurgical (cataract, glaucoma and laser surgeries), intraocular inflammatory diseases, medications, diabetic retinopathy and retinal vein occlusions.2 Treatments of CME vary from observation, medical and surgical.3 4 The visual outcomes are basically related to retinal structural changes of the macula especially in the long-standing cases. The ability to characterise the existence of CME is important in providing early treatment and knowing when to stop the treatment. This is critical in prevention of structural damages in long-standing CME that takes effect on the patient final visual outcomes.
The conventional standard tool for the diagnosis of CME is fluorescein angiography (FA), which is an invasive contrast-assisted modality. Doctors recognise CME as a classic “flower petal” leakage pattern in FA.5 However, the FA finding is dynamic and sometimes difficult to be interpreted, especially with the presence of retinal hemorrhages and exudates.
Optical coherence tomography (OCT) is a non-invasive and non-contact method that allows quantitative measurements of retinal thickness and volume. It provides cross-sectional images of the retina and useful information on vitreoretinal morphological changes associated with a variety of posterior segment diseases.6–8 Spectral-domain OCT (SD-OCT) is the latest generation of the technique and can provide images with high axial resolution and fewer motion artefacts.9–11 It allows identification of individual retinal layers approaching histological details with significant clinicopathological information in several retinal conditions.12 13 CME appears as cavitations of the outer plexiform and inner nuclear layers in the OCT scan. The present study correlates the SD-OCT and FA findings of CME at exact locations within the lesions.
Materials and methods
A retrospective chart review was conducted by analysing the image database of patients with the clinical diagnosis of CME who underwent SD-OCT and FA examinations on the same day as the clinical examination at the Retina Center of the New York Eye and Ear Infirmary between October 2007 and October 2008. New York Eye and Ear Infirmary Institutional Review Board approval was obtained before performing this retrospective observational study. Patients who met the following criteria were included: (1) clinical diagnosis of CME by a retina specialist based on slit lamp with contact lens examination and indirect ophthalmoscopy, regardless of the severity and comorbidity, and (2) having had SD-OCT and FA performed on the same day at the first visit and/or the follow-up visits. The exclusion criteria were (1) eyes with poor quality in OCT scans or FA images or (2) FA images showed severe pre-retinal or intraretinal blood at the macula area, which blocks the appearance of the underlying structures. Only one eye from each patient was included in this study. In the patient with bilateral CME, only the primary study eye on FA examination was analysed. A total of 85 eyes from 85 patients were included. Medical records of all eligible patients were reviewed to gather information regarding age, sex, types of clinical diagnosis of the retinal diseases, comorbidity, treatment and the duration between first and follow-up visits if any.
Procedures
A digital retinal camera system (Topcon TRC-501X FA; Topcon Medical Systems Inc, Paramus, New Jersey, USA) was used for FA examination. One retinal colour, one middle phase and one late phase frames were obtained from each eye. The colour frame was used to exclude the eye with thick preretinal or intraretinal blood at macula from the study. Middle phase and late phase frames were evaluated together to observe the dynamic changes and determine the location and the leakage patterns at the macula.
An SD-OCT device (Spectral OCT/SLO; OPKO/OTI, Miami, Florida, USA) was used together in both SLO and OCT images. The scanning location and direction shown in the SLO image simultaneously correlated with the cross section shown in the OCT image. The most characteristic OCT scan was chosen from each eye studied.
In the interpretation of images, one retina specialist was assigned to interpret the FA images, and another retina specialist was assigned to interpret the SD-OCT images. The interpreters worked in double-blinded fashion to avoid bias. Then, a late phase frame of FA and an image of SD-OCT scan from each eye were overlaid using Adobe Photoshop to correlate the exact location and direction of the cross-sectional scan with the FA findings.
Statistical analysis
The differences of the ability to describe CME and other macular findings between FA and SD-OCT were calculated in percentage for comparison purpose.
Results
We included 85 eyes from 85 patients (40 women and 45 men; mean age, 59.8 years; standard deviation, 8.9). Fifty-four (63%) eyes had retinal vein occlusion, 17 (20%) eyes had proliferative diabetic retinopathy (PDR), 1 (1.18%) eye had non-PDR (NPDR), 4 (4.71%) eyes had posterior uveitis, 3 (3.53%) eyes had vitreomacular traction syndrome (VMT), 3 (3.53%) eyes had age-related macular degeneration (AMD) and 3 (3.53%) eyes had postcataract surgery with vitreous loss.
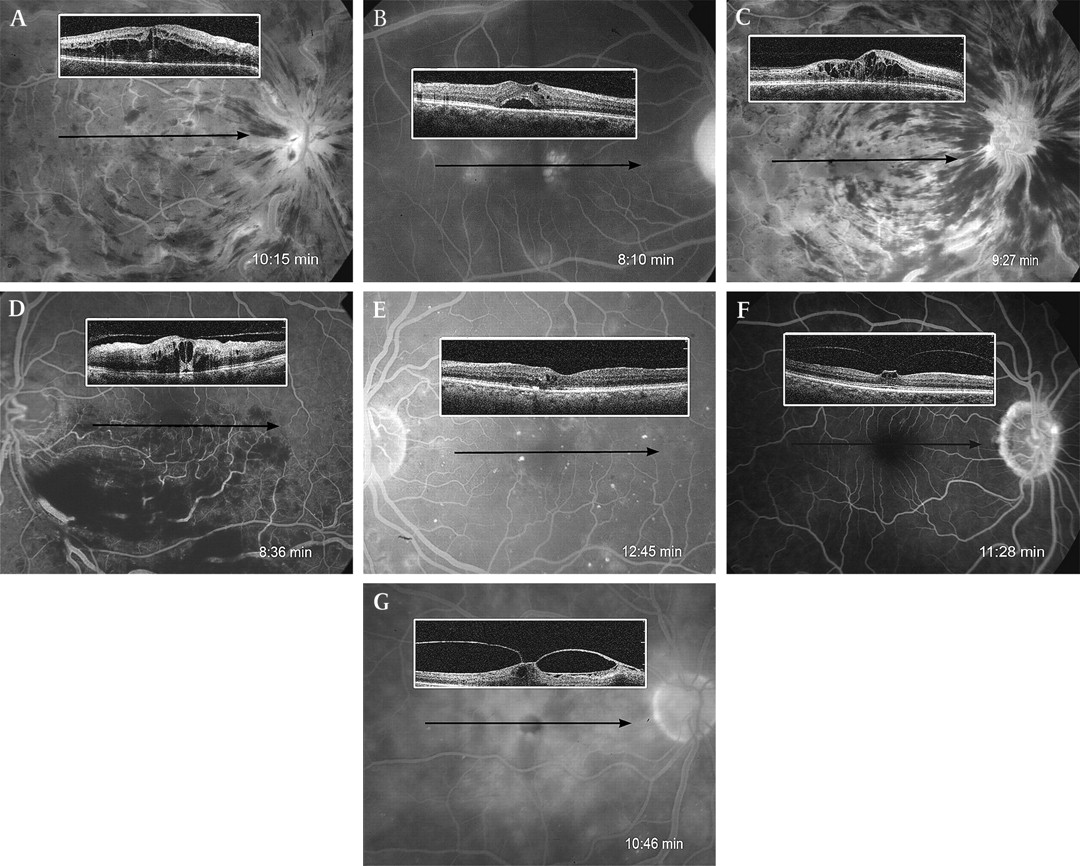
At the primary visits, the common causes of CME in our study were retinal vein occlusion (63%; branch retinal vein occlusion (BRVO), 30 eyes; central retinal vein occlusion (CRVO), 24 eyes), diabetic retinopathy (21.18%; PDR, 17 eyes; NPDR, one eye) and posterior uveitis (3.53%; four eyes). The percentages of cases where CME was missed by FA for RVO, AMD and DR were 18.52%, 33.33% and 33.33%, respectively. FA also missed CME diagnosis in patients with VMT in 66.67%. Subretinal fluid was undetectable by FA in 12 eyes from a total of 22 (54.55%) eyes that were mainly in the RVO group (eight eyes). (Details are shown in figure 1A–G and table 1).

A, Dx: CRVO, CME OD FA: no CME, SD-OCT: CME. B, Dx: foveal telangiectasia, CME, SRF OD FA: no CME, focal leakages, SD-OCT: CME with SRF. C, Dx: CRVO, CME OD FA: no CME, SD-OCT: CME. D, Dx: BRVO with CME OS FA: no CME, SD-OCT: CME. E, Dx: PDR, CME OS FA: no CME, SD-OCT: CME. F, Dx: VMT with CME OD FA: normal macula, SD-OCT: vitreous traction at fovea, CME. G, Dx: VMT, CME OD FA: CME, suspected MH, SD-OCT: Vitreo-retinal traction at fovea with CME. AMD, age-related macular degeneration; BRVO, branch retinal vein occlusion; CME, cystoid macular edema; CRVO, central retinal vein occlusion; Dx, diagnosis; EMM, epimacular membrane; FA, fluorescein angiography; MH, macular hole; NPDR, nonproliferative diabetic retinopathy; OD, oculus dexter; OS, oculus sinister; PDR, proliferative diabetic retinopathy; RPE, retinal pigment epithelium; SD-OCT, spectral-domain optical coherence tomography; SRF, subretinal fluid; VMT, vitreomacular traction syndrome.
The ability of FA and SD-OCT to characterise CME and SRF in the primary visit
At the follow-up visits (mean duration, 35.45 days; SD, 5.9), 97.65% of cases came back at the follow-up visit. Residual CME at follow-up visits were missed by FA in one (1.18%) eye. SD-OCT gave earlier CME diagnosis than FA in three (3.53%) eyes. (Details are shown in table 2.)
The ability of FA and SD-OCT to characterise residual CME in the follow-up visit
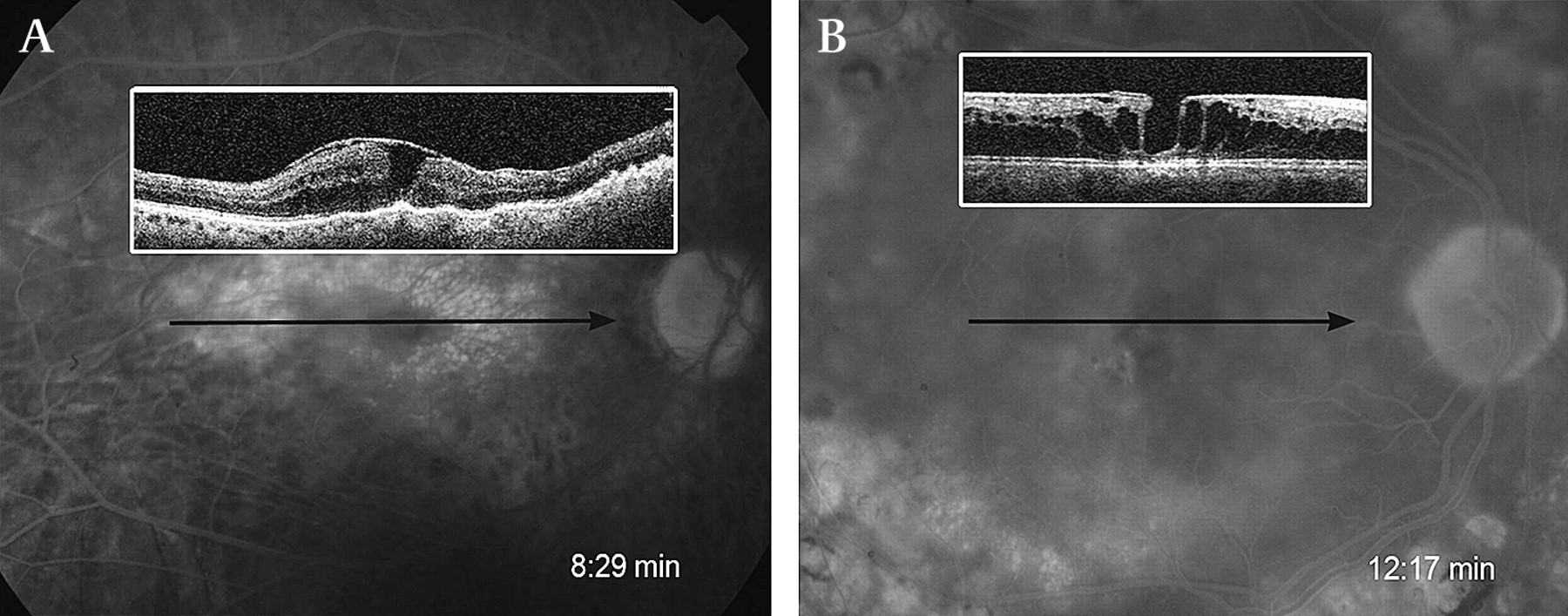
Follow-up SD-OCT revealed late complications of long-standing CME: secondary macular holes (two eyes), secondary epimacular membrane (three eyes), secondary subretinal fluid (five eyes), retinal pigment epithelium detachment (one eye) and photoreceptor atrophy (one eye). Compared with the SD-OCT, FA was able to demonstrate only secondary epimacular membrane (three eyes). (Details are shown in figure 2A,B and table 3.)

{kind=link}
{kind=link}
A, Dx: chronic CME with secondary MH, EMM OD FA: diffuse leakage c EMM SD-OCT: CME with progression to MH c EMM. B, Dx: CME, secondary MH OD FA: CME, SD-OCT: CME with secondary MH. CME, cystoid macular edema; Dx, diagnosis; EMM, epimacular membrane; FA, fluorescein angiography; MH, macular hole; NPDR, nonproliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy; RPE, retinal pigment epithelium; SD-OCT, spectral-domain optical coherence tomography; SRF, subretinal fluid; VMT, vitreomacular traction syndrome.
The ability of FA and SD-OCT to detect the complications of long-standing CME
Discussions
Our study revealed that SD-OCT was more sensitive than FA for the diagnosis of CME in some specific diseases. CME was most commonly missed by FA in patients with retinal vein occlusion, diabetic retinopathy and AMD in 18.52%, 33.33% and 33.33% of cases, respectively. SD-OCT was also more sensitive than FA in the diagnosis of the CME in the VMT in 66.67%. SD-OCT provided earlier CME diagnosis than FA in 3.53%. Furthermore, most complications of long-standing CME were diagnosed by SD-OCT whereas FA missed. However, CME associated with posterior uveitis and post–cataract surgery were found to have good correlation between SD-OCT and FA findings (no misdiagnosis found in our series).
Ozdek SC et al14 reported a series of diabetic retinopathy patients with associated CME that was detected by OCT but missed by FA in 63.3% of cases. Tran et al15 16 reported in two studies that FA and OCT were in agreement in 86% and 86.8% of cases for the diagnosis of CME associated with uveitis. These studies compared the ability between FA and time-domain OCT, whereas our study compared the ability between FA and spectral-domain OCT.
We found that SD-OCT was more sensitive than FA in detecting CME structural changes and in characterising complications of long-standing CME. In this series, we included three eyes with a clinical diagnosis of VMT; the FA study revealed minimal CME leakage in one eye and normal macula in two eyes, whereas SD-OCT showed intraretinal cavitations at the macula in three eyes. This may be because SD-OCT is more sensitive in detecting minor structural changes, which would only be detected later by FA if they manifested leakage. Some specific diseases (nicotinic acid retinopathy, Goldmann-Favre disease, X-linked juvenile retinoschisis and retinitis pigmentosa) present with CME but do not manifest FA leakage.17–20 None of the eye associated with these diseases were included in our study. In addition, FA study is frequently difficult to be interpreted with the presence of exudates or retinal blood at macula. This may explain why FA misdiagnoses the CME in the eye associated with diabetic retinopathy, retinal vein occlusions and wet AMD, which frequently present with hard exudates and retinal blood at macula. FA, however, continues to be the criterion standard for studying macular pathological conditions because it provides anatomic structural diagnosis, vascular perfusion dynamics and evidence of blood-retinal barrier breakdown.
We conclude that SD-OCT has a higher ability than FA in characterising the existence of CME, which is important in providing early treatment and knowing when to stop the treatment. This is critical in the prevention of structural damages in long-standing CME, which takes effect on the patient final visual outcomes.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Ethics Committee of the New York Eye and Ear Infirmary, New York, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance