Article Text

Abstract
AIMS To determine functional results after unilateral and bilateral cataract surgery in children with different aphakic optical correction.
METHODS In this retrospective study, we evaluated visual acuity and binocular vision in 107 children who underwent cataract surgery during the 10 year period from 1985 to 1995. Aphakia was corrected by an intracapsular intraocular lens (IOL), spectacles or contact lenses.
RESULTS Mean visual acuity was >20/40 (<0.3 log MAR) with normal binocular vision in 58 children over 7 months of age operated on for bilateral cataracts. Pseudophakic eyes regained visual acuity >20/63 (<0.5 log MAR) more often (90%) than aphakic eyes (46%) (p<0.001). Binocular vision was also achieved more often after IOL implantation (p<0.001). Visual outcome of early bilateral cataracts was less satisfactory in children with abnormal foveolar function. For 49 children who had surgery for unilateral cataracts, prognosis was poor when surgery was performed before the age of 7 months. For cataract surgery in older children (⩾7 months) mean visual acuities were better with IOL implantation (p<0.05).
CONCLUSION Cataract surgery with unilateral and bilateral IOL implantation can provide a beneficial effect on final visual outcome in children who are operated on before abnormal foveolar function develops.
- binocular vision
- intraocular lens
- paediatric cataract
- visual outcome
Statistics from Altmetric.com
The aim of cataract surgery in children is to enable the acquisition or the restoration of a normal visual function. While contact lenses are a simple procedure to correct aphakia in children after cataract surgery,1 2 intraocular lenses (IOLs) have been quite successful and are used as a standard means of optically correcting vision.3-6 If cataract surgery fails in infants, the development of deprivation amblyopia determines final visual prognosis.
We retrospectively assessed final visual outcome in 135 children who underwent surgery for unilateral or bilateral cataracts, studying the effect of age at surgery and aphakia correction with or without intraocular lenses.
Patients and methods
Over a 10 year period, from January 1985 to December 1995, 165 eyes in 107 children aged 1 month to 16 years were operated on for unilateral or bilateral cataract and followed up at the ophthalmology unit, Purpan University Hospital, Toulouse, France.
Unilateral cataract surgery was performed in 49 children; 11 under the age of 7 months (group U1); 17 aged over 7 months (group U2); and 21 with unilateral traumatic cataract (group U3).
Bilateral cataract surgery was performed in 58 children; 21 under the age of 7 months (group B1) and 37 over 7 months (group B2).
Visual outcome was thus assessed for 49 eyes operated on for unilateral cataract and 116 eyes for bilateral cataracts.
In the 11 cases in group U1 (under 7 months) the diagnosis was total cataract and surgery was performed immediately upon diagnosis. For bilateral cataracts, the both eyes were operated during the same week.
The decision for surgery in children over 7 months of age was based on loss of best corrected visual acuity (<20/40), onset of strabismus or nystagmus and loss of binocular vision.
Exclusion criteria were associated ocular anomalies (glaucoma, severe microphthalmia, posterior segment pathology, retinopathy of prematurity), systemic or mental disorders, surgery within the past 12 months and absence of follow up at the ophthalmology unit at the University of Toulouse Hospital.
SURGICAL TECHNIQUE
The surgical procedure consisted in an anterior limbal incision (3.2 mm), continuous anterior capsulorhexis, and phacoaspiration. Surgery was completed with peripheral iridectomy under miosis and single suture wound closure. Before the age of 5 years, primary posterior capsulotomy with a needle combined with central anterior vitrectomy through the same anterior limbal incision was performed to prevent secondary opacification of the posterior capsule. In the cases of implantation, a PMMA single piece intracapsular intraocular lens (IOL) measuring 5.5–7 mm in optical diameter was placed in an intracapsular position via an enlarged incision.7-9
Aphakia was corrected by spectacles or contact lenses in most of the children with early bilateral cataracts or when anatomical conditions were unsatisfactory for implantation (large rupture of posterior capsule, early miosis, or impossibility to place the IOL in an intracapsular position). Implantation was preferred in all cases of unilateral cataract and in cases of bilateral cataracts in children over 5.
AMBLYOPIA TREATMENT
Amblyopia therapy was initiated immediately after surgery and adapted to visual gain. Patch occlusion during the day varied from 3 hours to 6 hours for the first month after surgery and was maintained thereafter if necessary.
VISUAL REVIEW
The Teller acuity cards and Snellen acuity test adapted for children of verbal or preverbal age were used to measure visual acuity. Binocular vision was assessed with the Wirt and Lang tests. One orthoptist consultant in our ophthalmology unit performed the visual review in all the children.
STATISTICAL METHODS
Visual acuities were converted into a log scale using the method outlined by Holladay and Prager.10 Quantitative data (visual acuity) were compared with the Student–Fisher test for sample sizes ⩾10 or with the Mann–Whitney U test for sample sizes ⩽10. Qualitative data (binocular vision) were analysed with the Yates’s corrected χ2 test for sample size ⩾5 or the exact calculation method (contingency table) for sample size ⩽5.
Results
Visual outcome after cataract surgery in 116 eyes is shown in Table 1.
Distribution of functional results
VISUAL ACUITY
The distribution of visual acuity after surgery for unilateral cataracts is illustrated in Figure 1. In group U1, early unilateral cataracts, an IOL was implanted in four of the 11 eyes. Mean visual acuities were poor for aphakic (1.029 log MAR) and pseudophakic eyes (0.925 log MAR) without significant difference. Visual acuity >20/63 (<0.5 log MAR) was recovered in only two eyes.

Unilateral cataracts. Distribution of visual acuities in pseudophakic (IOL) and aphakic (No IOL) eyes after surgery for early (group U1), late (group U2), and traumatic (group U3) cataracts.
For late unilateral cataracts, group U2 results were better. IOLs were implanted in 15 of the 17 operated eyes. Mean post-surgery visual acuity (0.322 log MAR) was significantly higher (p <0.05) in the 15 IOL pseudophakic eyes than in the two aphakic eyes (1 log MAR). Although the sample size was insufficient to evidence a significant difference in this group, the proportion of pseudophakic eyes with a visual acuity >20/32 (<0.2 log MAR) was high (40%) compared with the aphakic eyes which were both <20/63 (>0.5 log MAR). These latter two children were aged 13 months at surgery and contact lenses where chosen because satisfactory implantation is quite difficult to achieve at this age.
For group U3, traumatic cataracts, results were similar to those in group U2. IOLs were implanted in 18 of the 21 eyes. Mean visual acuity was better in pseudophakic eyes (0.230 log MAR) than in aphakic eyes (0.540 log MAR), although the significance threshold was not reached due to the small sample size. Again, there were more eyes with visual acuity >20/63 (<0.5 log MAR) in the pseudophakic group (88%) than in the aphakic group (33%).
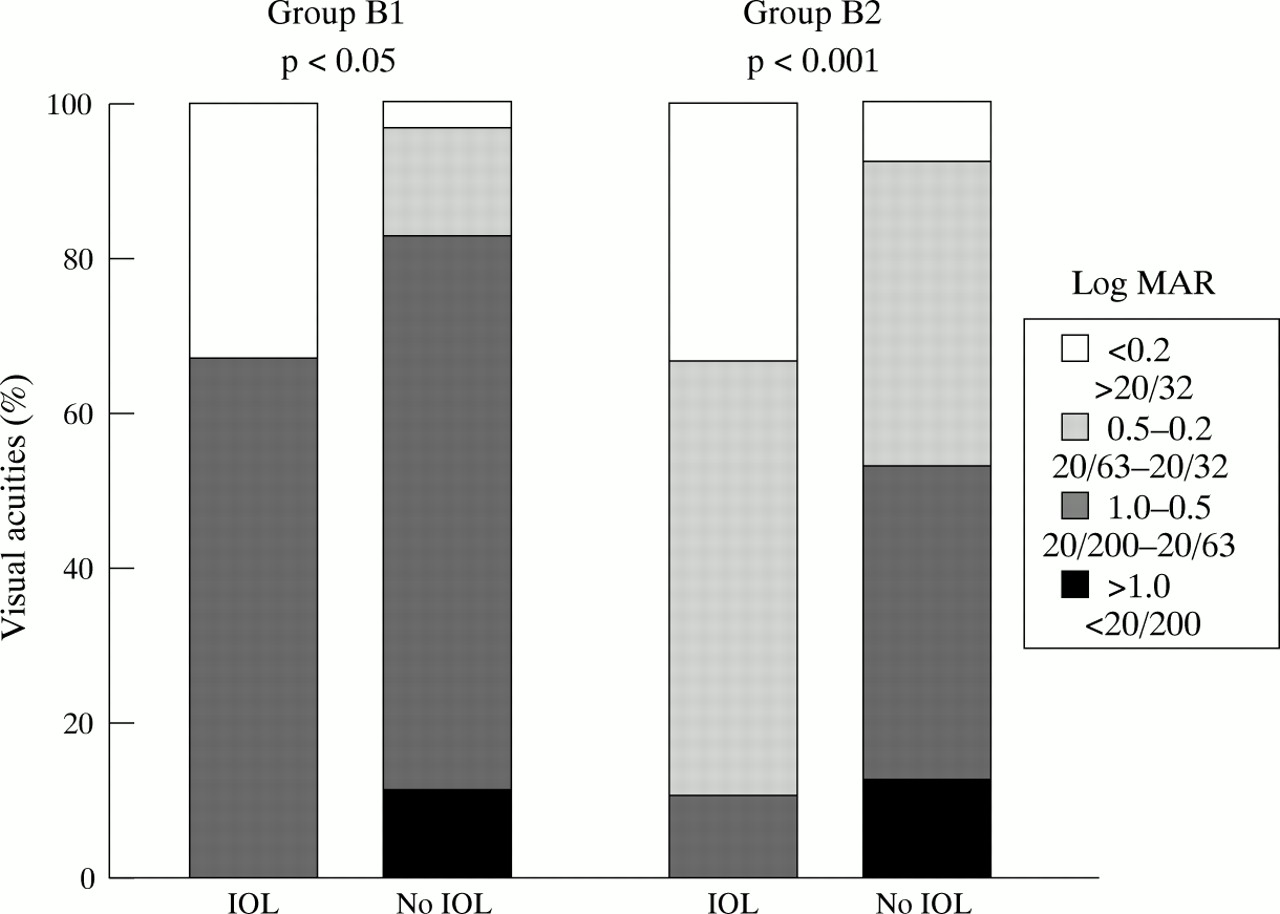
Figure 2 shows the distribution of visual acuity outcomes for bilateral cataracts. In group B1 of early bilateral cataracts (42 eyes), six eyes were implanted. The mean visual acuity was significantly higher (p<0.05 ) in the pseudophakic eyes (0.425 log MAR) than in the aphakic eyes (0.728 log MAR). Visual acuity > 20/63 (<0.5 log MAR) was achieved more often in implanted eyes (33%) than in non-implanted eyes (17%).

Bilateral cataracts. Distribution of visual acuities in pseudophakic (IOL) and aphakic (No IOL) eyes after surgery for early (group B1) and late (group B2) cataracts.
The best visual outcomes were obtained in group B2, late bilateral cataracts. Of the 74 eyes operated on, 50 received an IOL. There was a highly significant difference (p <0.001) between mean visual acuity in pseudophakic eyes (0.206 log MAR) and in aphakic eyes (0.607 log MAR). Moreover, the proportion of eyes with a visual acuity >20/63 (<0.5 log MAR) was significantly higher (p <0.001) in the implanted eyes (90%) than in eyes corrected with spectacles or contact lenses (46%). Visual acuity >20/32 (<0.2 log MAR) was achieved in 33% of the pseudophakic eyes.
BINOCULAR VISION
As shown in Figure 3, the presence of binocular vision for the unilateral cataract groups tended to vary with age at surgery (group U1: 25%; group U2: 53%; group U3: 85.7%). Moreover, we found a difference between the age of patients in group U2 who received IOLs (67.7 months) compared with those who did not (13 months). This difference was also observed for binocular vision which was present in 53% of the patients with IOL implantation and never found in patients without the IOL procedure.

{kind=link}
{kind=link}
{kind=link}
Binocular vision; difference in patients with (IOL) and without (No IOL) lens implantation.
However, binocular vision was found more often in children in all three unilateral groups for whom aphakia had been corrected with an IOL. The results are similar in the bilateral groups where a highly significant difference (p<0.001) was found for the pseudophakic eyes.
Discussion
Many studies reporting visual outcome after cataract surgery in paediatric patients focus on the type of cataract encountered (unilateral or bilateral) and the different methods used to correct aphakia.11 12 Lens implantation in paediatric aphakia remains a controversial issue.13
In our study, mean visual acuity in early unilateral cataracts remained poor (0.981 log MAR), with no statistically significant difference between aphakic and pseudophakic eyes. Only one child treated for unilateral cataract recovered binocular vision; he had received an IOL. This lack of recovery of binocular vision is linked to the development of irremediable amblyopia in early unilateral cataracts. Many studies in the literature emphasise the advantage of very early surgery so visual acquisition can be achieved before abnormal binocular interaction develops.14 Wright et al 15 have shown that sensorial fusion exists in 60% of children with eye surgery 9 weeks after birth. Birch et al 16 found that visual acuity reached 20/40 if surgery is undertaken before the age of 6 weeks. Moreover, Sinskeyet al 17 have demonstrated that IOLs can be implanted without major surgical complications as early as 17 days after birth. Gregg and Parks18 have also described the visual outcome of a 1 day old infant who achieved a visual acuity of 20/25 (0.1 log MAR) with binocular vision at 8 years. Finally, the work reported by Lewis et al 19 also demonstrated the advantages of very early surgery owing to its effect on contralateral amblyopia induced by a central amblyogenic process.
For aphakia correction, visual outcome was better with a primary intracapsular implantation than with contact lenses although the difference between aphakic and pseudophakic eyes was not statistically significant.
In children with early bilateral cataracts, we found a significant difference (p <0.05) in mean visual acuities in favour of lens implantation. In addition, only two children with aphakic eyes acquired binocular vision. It should be noted that in early bilateral cataracts, the existence of nystagmus plays a determining role in functional visual prognosis. The work of Robb and Petersen20 has shown poor visual results in children who had nystagmus before surgery. There are few data on implantation. Markham et al 21 published their visual outcome results in infants operated on for early bilateral cataracts at 3 and 7 months of age. Their results were similar to ours for this type of cataract. Consequently, poor visual outcome following surgery for early bilateral cataracts would appear to be related to the existence of pre- and postoperative nystagmus. Since at the present time few results have shown long term benefit from IOL, the decision to implant in these children must be weighed carefully.
For late unilateral and bilateral cataracts, however, visual outcome is more satisfactory. In our study, mean visual acuities were always significantly higher in pseudophakic eyes. Likewise, the percentage of eyes with visual acuity >20/63 (<0.5 log MAR) was higher in cases with lens implantation, with a highly significant difference (p <0.001) for late bilateral cataracts. Moreover, binocular vision was significantly more frequent in pseudophakic eyes. Gimbel et al 22 23 operated 24 pseudophakic eyes in children over the age of 2 and found that visual acuity was >20/40 (<0.3 log MAR) 4 years after surgery in 79.2% of cases. Our results are in agreement with these findings.
Finally, Ben Ezra and Paez24 found foveolar fixing with a visual acuity >20/40 (<0.3 log MAR) in nine children operated on for unilateral cataract with primary implantation performed after the age of 1½, without any major postoperative complications.
Our findings and those reported by Koenig et al,25 who showed that 87% of children implanted with an IOL recovered visual acuity >20/40 (<0.3 log MAR), also suggest that lens implantation would be the appropriate choice for traumatic cataracts if operating conditions are favourable and retinal damage can be avoided.
Conclusion
IOLs implantation is generally considered to be a safe surgical technique for the correction of paediatric aphakia.26Visual outcome after surgical treatment of cataracts depends on the type of cataract encountered. For early unilateral and bilateral cataracts, good prognosis for visual acuity and binocular vision depends on early diagnosis and surgery before the development of abnormal foveolar function. Detection plays a crucial role here. The problem is different in late unilateral and bilateral cataracts because vision was acquired before cataract development. The question which is raised is one of identifying correct indications for lens implantation. The surgeon’s decision should be based on personal experience and family consent after discussion with the medical team, essential for successful rehabilitation.
The mean visual acuities reported here after IOL implantation in children show that excellent visual outcome can be achieved with statistically significant differences between early and late bilateral cataracts, and late unilateral cataracts. Thus implantation would be indicated for unilateral and bilateral cataracts if surgery is undertaken before the development of abnormal foveal function. Foveal function and not age at surgery is the determining factor for visual outcome after paediatric cataract surgery.
Acknowledgments
The authors have no financial or proprietary interest in this study.