Article Text

Abstract
Objective To evaluate the anatomical and visual outcomes of patients treated with ocriplasmin for the treatment of symptomatic vitreomacular adhesion (sVMA), including vitreomacular traction syndrome and macular holes.
Design Retrospective, interventional, single centre, case series.
Participants Patients with sVMA.
Intervention Patients were treated with a single intravitreal injection of 0.125 mg ocriplasmin (Jetrea, Thrombogenics Inc, USA, Alcon/Novartis EU) with the reconstitution technique recommended by the manufacturer.
Main outcome measures The primary study endpoint was the resolution of sVMA by spectral domain optical coherence tomography (SDOCT) at day 28. Secondary outcome measures included time to vitreous release, visual acuity (VA), changes in the optical coherence tomography (OCT) thickness and structure and macular hole closure rate.
Results 17 patients were included in the study and resolution of vitreomacular adhesion (VMA) was verified by SDOCT in eight patients by day 28 (overall response rate of 47.1%, 8/17 eyes) with most patients experiencing VMA release by 7 days (41.2%, 7/17 eyes). Those who did not have VMA resolution showed no statistically significant change in VMA diameter as measured by horizontal and vertical 5-line raster scans at final follow-up (p=0.82 and p=0.75, respectively). The mean baseline Snellen VA was 20/49 and at final follow-up was 20/46 (p=0.59). The average central subfield thickness was 371 microns prior to treatment and 324 microns at final follow-up (range 191–767 microns, p=0.25). Patients meeting three of four positive predictors criteria (eg, no epiretinal membrane (ERM) at baseline, VMA diameter ≤1500 µm and phakic lens status) showed a response rate of 50.0% (seven of 14 patients); those meeting all four criteria (eg, younger than 65, no ERM at baseline, VMA diameter ≤1500 µm and phakic lens status) showed a response rate of 75.0% (three of four eyes). Transient outer segment ellipsoid zone loss was documented in seven patients and subretinal fluid presence following injection was noted in five patients. Four of the five patients with macular holes at baseline experienced resolution of their macular hole after injection.
Conclusions This is the first study to quantify the extent of outer retinal changes seen in patients receiving ocriplasmin. Our initial experience with ocriplasmin shows a significant anatomical effect and is accompanied by transient changes in the outer retinal structures visualised by SDOCT.
- Optic Nerve
Statistics from Altmetric.com
Introduction
Up until recently, vitrectomy was the only treatment for vitreomacular traction and macular hole. Given the complications and side effects of vitrectomy such as infection, retinal detachment, haemorrhage and cataract formation, other methods for safe release of this vitreomacular adhesion (VMA) have been investigated. Pharmacologic vitreolysis involves the use of an enzyme to degrade the molecular substrates responsible for VMA and allows for a different biologic approach to the treatment of this disorder. Ocriplasmin (Jetrea, Thrombogenics USA, Alcon/Novartis EU) is a recombinant protease recently approved for the treatment of symptomatic vitreomacular adhesion (sVMA) that cleaves laminin and fibronectin which mediate attachments of the cortical vitreous to the retina, as well as leads to vitreous liquification.1
The MIVI-TRUST trials were two, parallel, phase III randomised control trials comparing the effectiveness of a single ocriplasmin injection with a placebo saline injection in the treatment of sVMA, including macular holes.2 A total of 652 eyes underwent a single intravitreal injection of ocriplasmin (125 µg) with 26.5% showing resolution of VMA by day 28 in comparison with 10.1% treated with placebo injections (p<0.001). The trials also correlated a positive clinical outcome with certain baseline characteristics: age less than 65 years of age, absence of an epiretinal membrane (ERM) at baseline, VMA diameter of ≤1500 µm and phakic lens status. Release rates were better when these baseline characteristics were present.
While randomised clinical trials help establish the effectiveness of any therapy, real-life experience offers more fine-tuned commentary from the clinic setting. In addition, since the MIVI-TRUST study employed only time domain optical coherence tomography (TDOCT), the evaluation of spectral domain optical coherence tomography (SDOCT) findings and outcomes following treatment may provide more insights into ocriplasmin's structural effects following treatment. The purpose of this study was to evaluate the structural and visual outcomes of patients treated with ocriplasmin for the treatment of symptomatic vitreomacular traction syndrome.
Methods
After Cleveland Clinic institutional review board approval, patients were identified from a chart review of a retrospective case series of patients seen at the Cole Eye Institute (Cleveland Clinic, Cleveland, Ohio, USA) from March 2013 to July 2013 who met the following inclusion criteria: receipt of an intravitreal injection of ocriplasmin for the diagnosis of sVMA with the ICD-9 diagnosis code of 379.27. Patients who had both baseline and follow-up SDOCT scans and at least 28 days of follow-up since their initial injection were included in the analysis. sVMA was defined as cortical vitreous adhesion to the macula within a 6 mm central retinal field surrounded by elevation of the posterior vitreous cortex on SDOCT. Patients were excluded from the analysis if they had active proliferative diabetic retinopathy, neovascular age-related macular degeneration, retinal vascular occlusion, aphakia, high myopia (more than −8 diopters) and uncontrolled glaucoma. Given these exclusion criteria, only one patient who received ocriplasmin was removed from the analysis. The presence of an ERM was not a criterion for exclusion.
The primary outcome of the study was OCT-verified resolution of sVMA at day 28. This was defined as vitreous release from the macula within a 6 mm central retinal field by SDOCT. Secondary outcome measures included Snellen visual acuity (VA), change in OCT centre subfield thickness, change in retinal structure on SDOCT, macular hole closure on SDOCT and the incidence of serious and non-serious ocular adverse events (AEs).
Treatments and assessments
All patients received an intravitreal injection of ocriplasmin (125 μg in a 0.10 mL volume) drawn from a vial containing ocriplasmin into which 0.75 mL of commercial saline had been injected (1875 μg of ocriplasmin in a 0.75 mL drug vehicle).
At baseline and each follow-up visit, an SD-OCT macular cube and horizontal and vertical 5 raster scan protocols were performed with a Zeiss Cirrus HD-OCT (Cirrus V.6.1 software). SDOCT measurements included the central subfield thickness (internal limiting membrane (ILM)–retinal pigment epithelium (RPE)), cystoid macular oedema (CMO) grade and the presence or absence of an ERM, subretinal fluid and the outer segment ellipsoid zone (aka inner segment/outer segment (IS/OS) junction).3 Gass staging criteria of macular holes were used to classify the baseline OCTs.4 CMO was graded based on a five-point scale, with grade zero being no CMO, grade one being extrafoveal CMO, grade two being foveal CMO with a flat fovea, grade three being CMO with fovea slightly raised and grade four being CMO with fovea significantly raised.3 Two masked graders (AL and RB) independently read all OCT images. Snellen VA measurements were converted to logMar values for statistical analysis. AEs were obtained from self-reported assessments at each visit. All tests were two-sided, and p values less than 0.05 were considered statistically significant.
Results
A total of 17 patients who met all inclusion and exclusion criteria were identified. The mean age of cohort was 68.8±9.03 years (range 54–85 years). Eleven patients were women and six patients were men. All injections were performed between 3 June 2013 and 17 June 2013. Average Snellen mean baseline logMar VA was 0.36 (Snellen equivalent of 20/49). The mean central subfield thickness prior to injection was 371 microns (range 208–934 microns).
The primary outcome of resolution of sVMA was achieved in eight patients by day 28 (response rate of 47.1%) (figure 1). Most patients experienced vitreomacular release by 7 days (41.2%), but some patients exhibited release as early as 2 days (n=1) and as late as 28 days (n=1) after treatment. The average Snellen logMar VA at 28 days was 0.40 (Snellen equivalent of 20/46, p=0.59). The mean central subfield thickness following injection was 324 microns (range 191–767 microns, p=0.25). The average Snellen logMar acuity in patients achieving the primary outcome of VMA release was 0.360 (Snellen equivalent of 20/40, p=0.44 from baseline) in comparison with average Snellen logMar acuity in patients not achieving release was 0.435 (Snellen equivalent of 20/62, p=0.65 from baseline). While there was a trend of improved acuity in the VMA release group, this was not statistically different from the patients without VMA release (p=0.29).
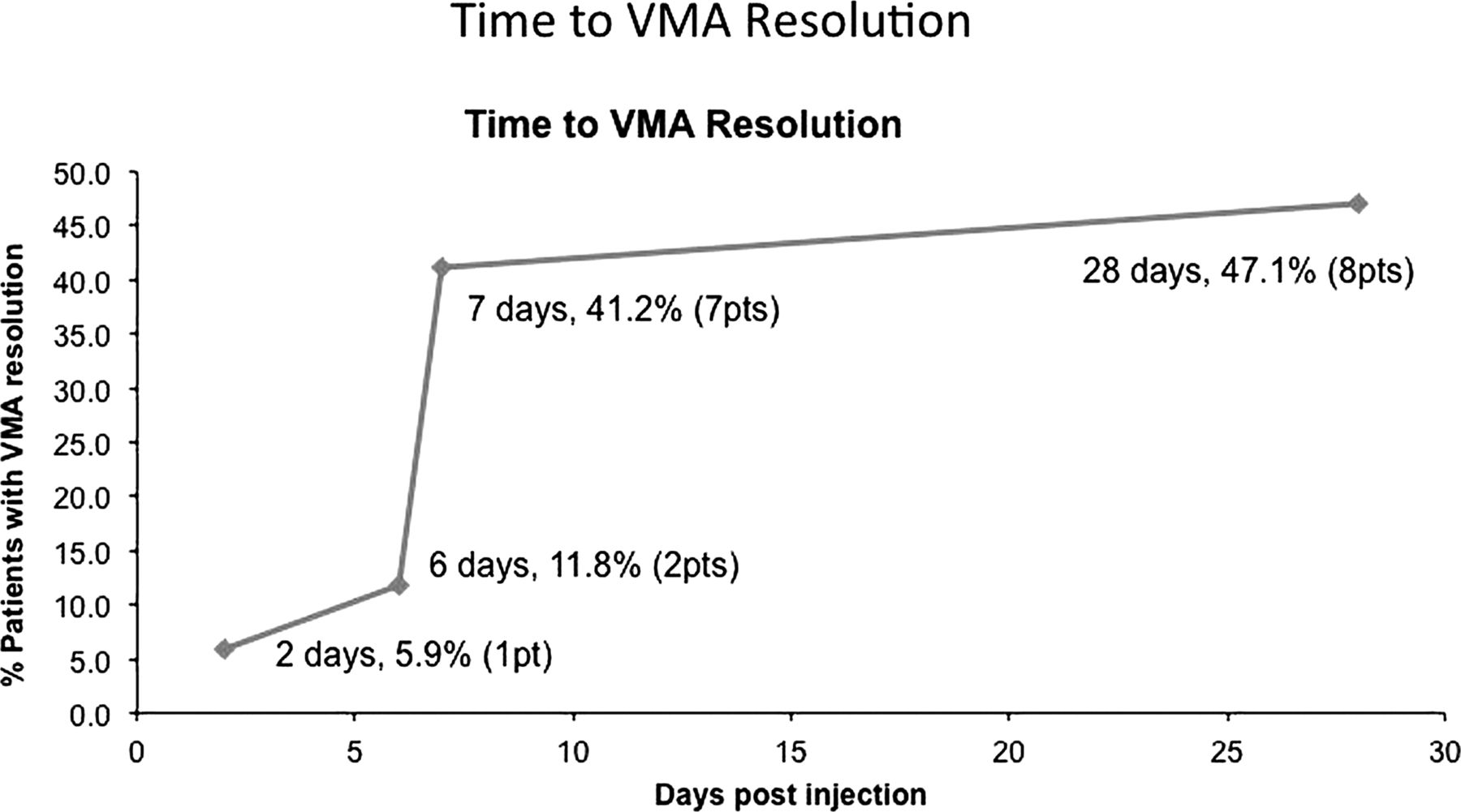
Time to vitreomacular adhesion (VMA) resolution following ocriplasmin injection. pts, patients.
Those who did not have VMA resolution showed no statistically significant change in VMA diameter as measured in horizontal and vertical 5-line raster scans at 4 weeks. The mean baseline and post-injection horizontal adhesion diameters were 888 and 903 µm, respectively (p=0.82), and the mean baseline and post-injection vertical adhesion diameters were 631 and 620 µm, respectively (p=0.75).
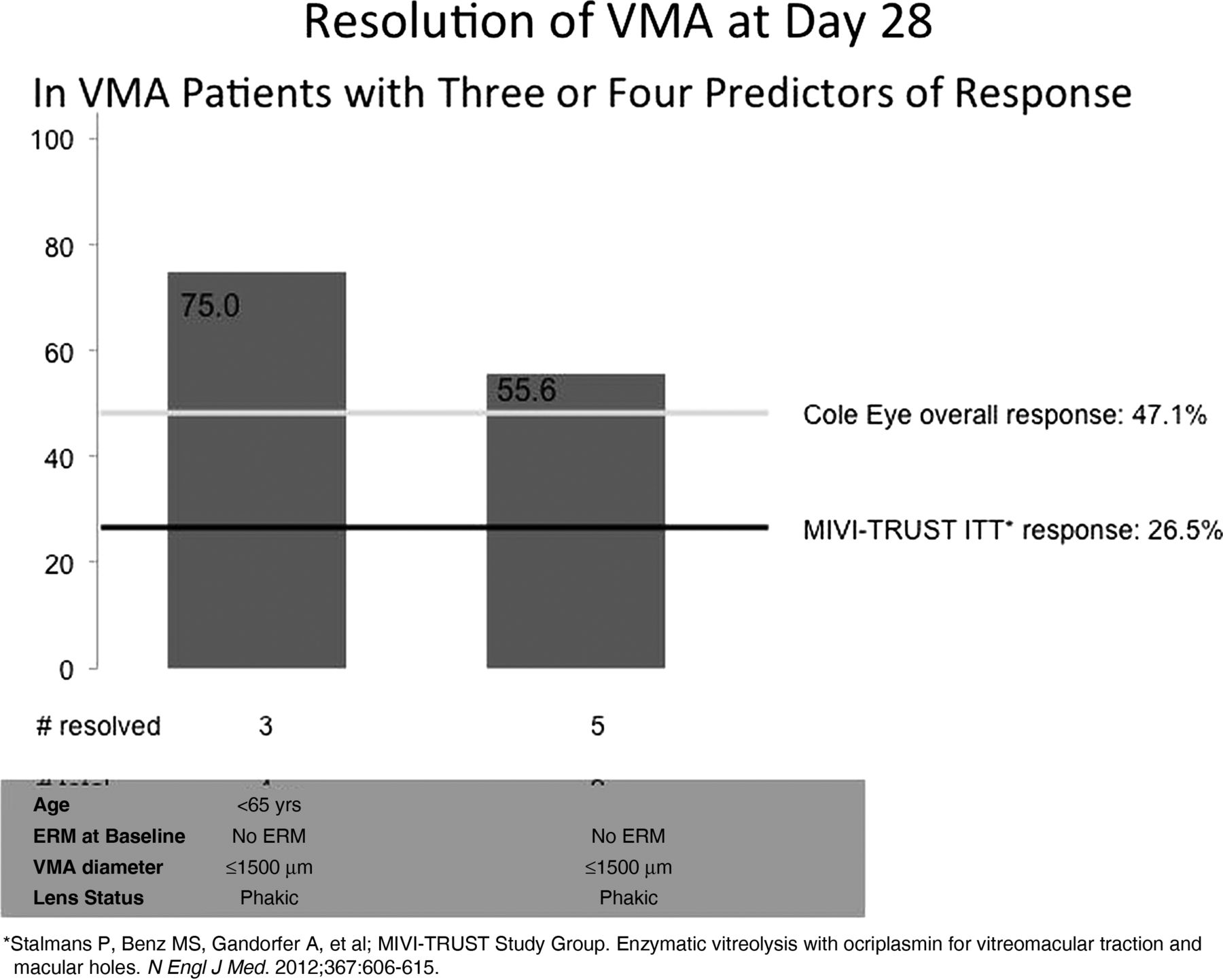
Patients who exhibited one or more of the positive predictors were indeed more likely to respond to treatment at day 28 (figure 2). Furthermore, patients meeting three or more predictors had a much greater rate of response than described in the clinical trials. Those meeting three of the four criteria (eg, no ERM at baseline, VMA diameter≤1500 µm and phakic lens status) showed a response rate of 50.0% (seven of 14 eyes); those meeting all four criteria showed a response rate of 75.0% (three of four eyes) (figure 3).
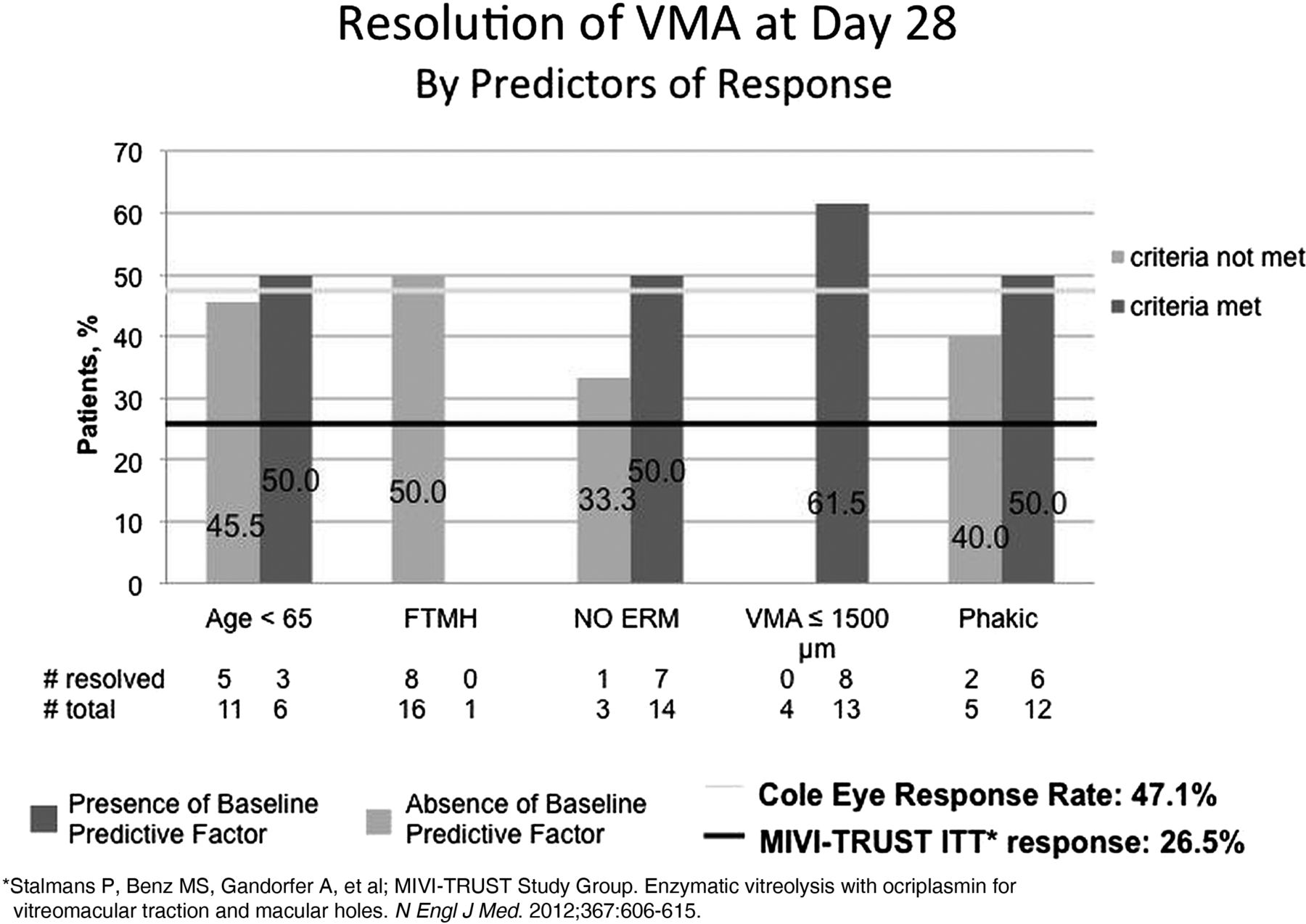
Resolution of vitreomacular adhesion (VMA) at day 28 by predictors of response. ERM, epiretinal membrane; FTMH, full thickness macular hole. *Adapted from Stalmans et al [2].
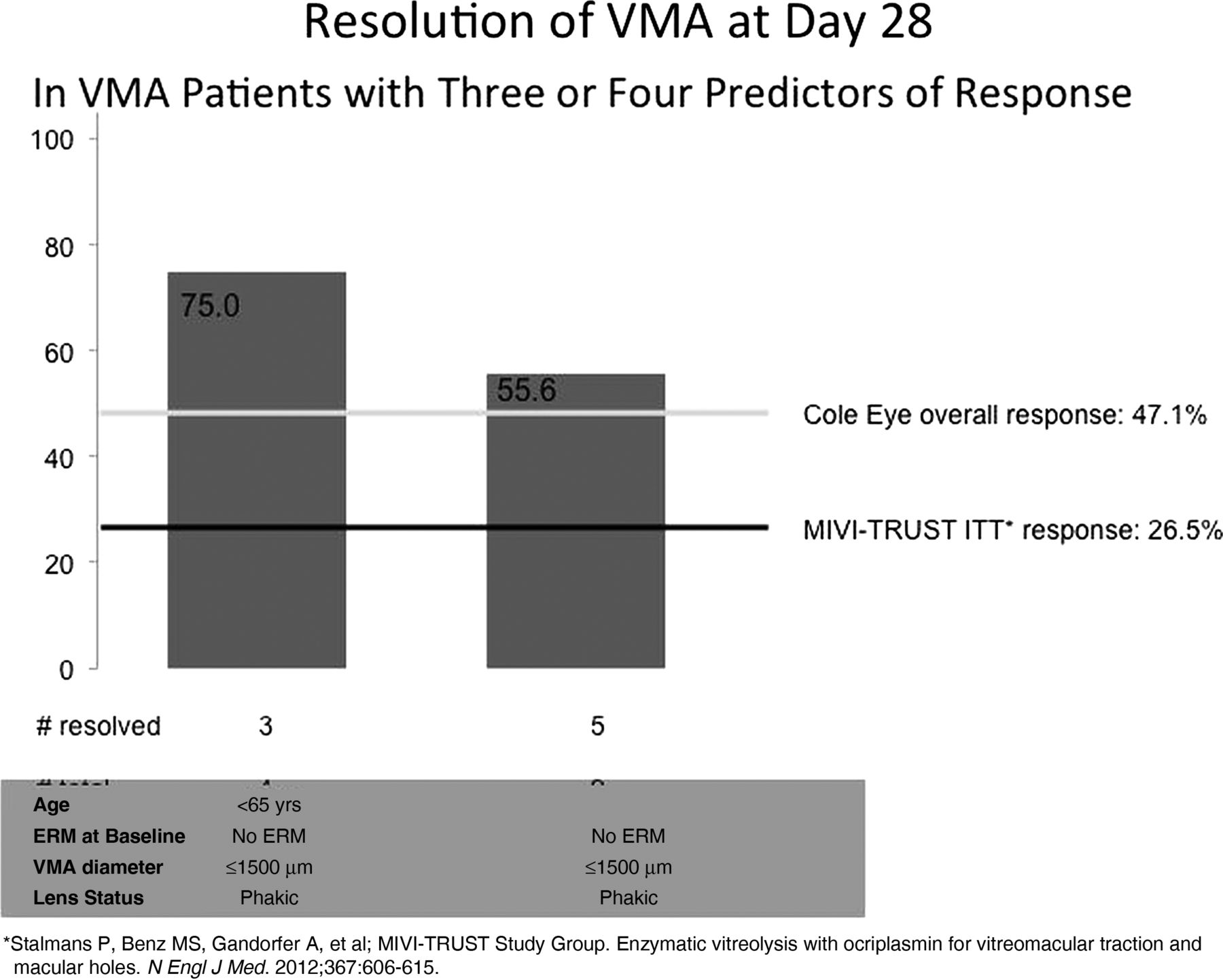
Resolution of vitreomacular adhesion (VMA) with three or four predictors of response. ERM, epiretinal membrane. *Adapted from Stalmans et al [2].
Patients’ self-reported ocular AEs following ocriplasmin injection were analysed. Most symptoms occurred within 2 days of injection and usually resolved by 1 week. The most common complaint was photopsias, which was reported by 63% (n=5) of responders and 40% (n=2) of non-responders. Other patient-reported AEs in order of most common to least include blurry vision, reduced VA, vitreous floaters, eye pain, tearing, eye redness, foreign body sensation, dryness, loss of contrast sensitivity and photophobia (table 1).
Ocular adverse events (AEs) following injection by number
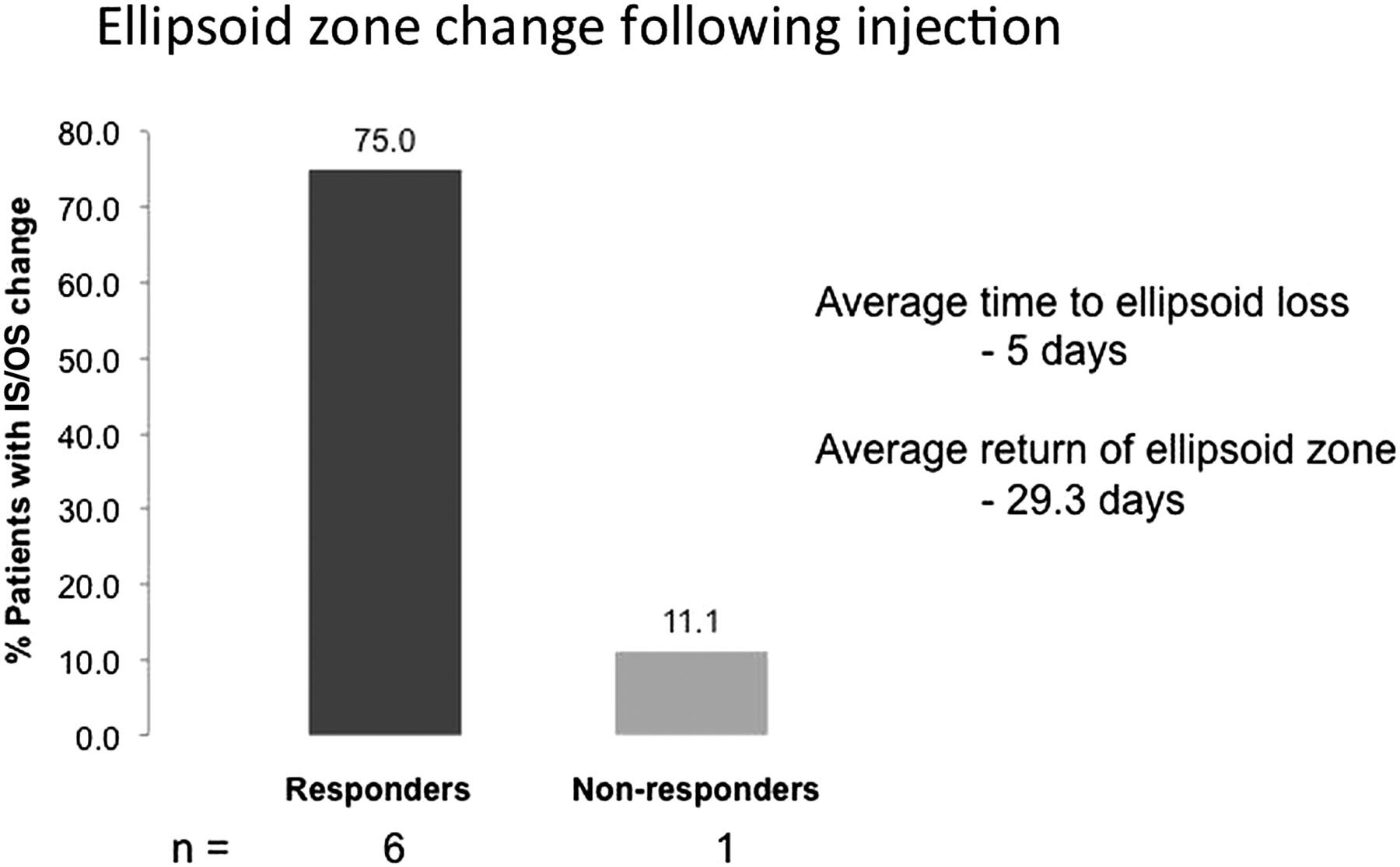
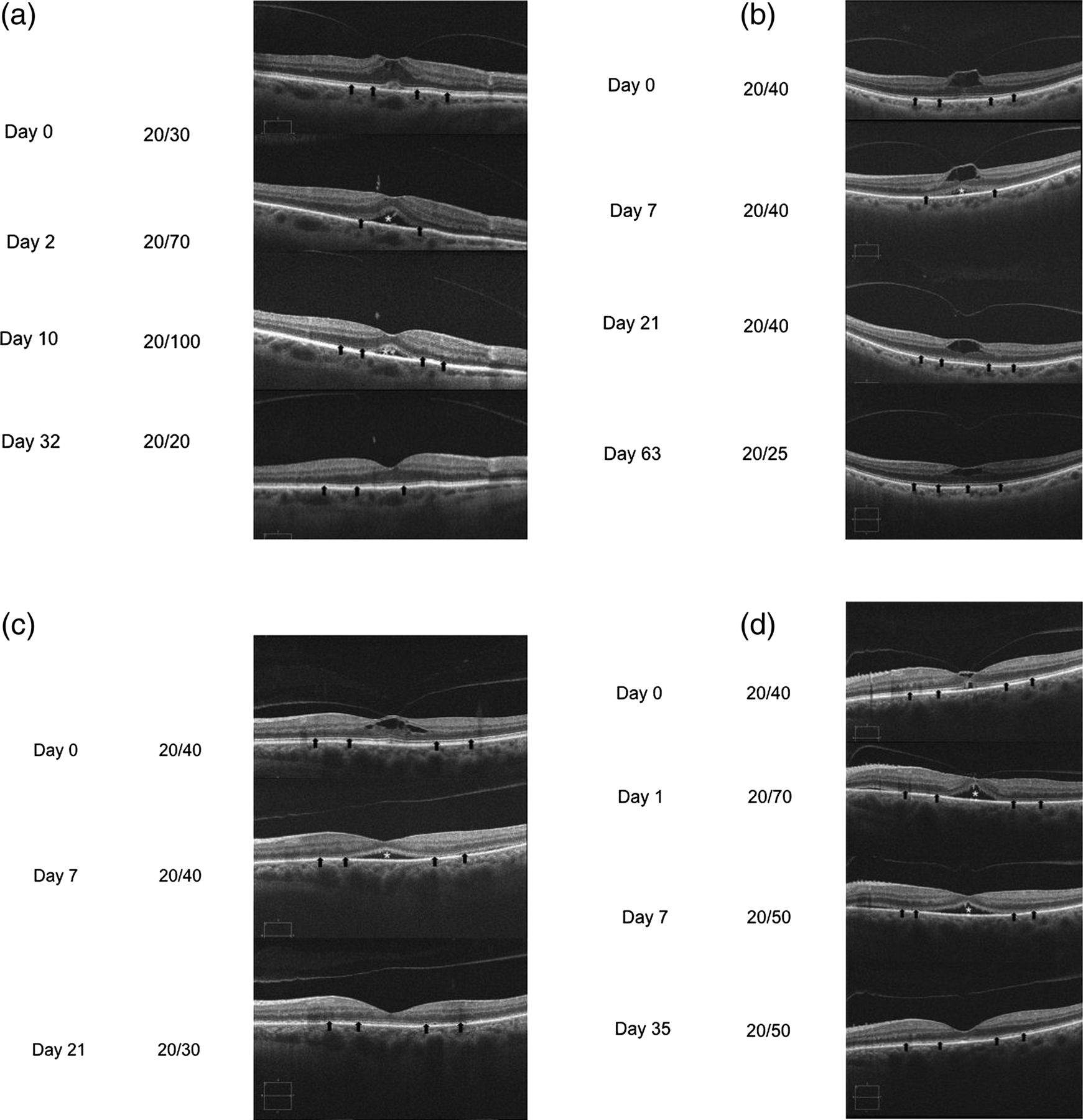
Seven patients experienced OS ellipsoid zone loss on SDOCT. Of the patients experiencing loss of the OS ellipsoid zone, almost all (six patients) had a positive outcome with VMA release with only one patient not having VMA release. One patient experienced VMA release without OS ellipsoid zone loss. In all patients, the OS ellipsoid zone loss was transient. The average time to loss of the OS ellipsoid zone was 5 days and the average time to return of the OS ellipsoid zone on OCT was 29.3 days (figure 4). Interestingly, this finding was temporally correlated with the presence of subretinal fluid in patients (the average time to presence of subretinal fluid (SRF) was 4.8 days and resolution by 30 days). A total of five patients experienced worsening subretinal fluid following injection. Of these five patients, all patients were also observed to have transient OS ellipsoid zone loss (figure 5A–D).

Ellipsoid zone change following injection in responders and non-responders groups. IS/OS, inner segment/outer segment junction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of ellipsoid zone loss and subretinal fluid accumulation following ocriplasmin injection. (A) Patient example 1, (B) Patient example 2, (C) Patient example 3, and (D) Patient example 4. *refers to areas of subretinal fluid. The arrows show the IS/OS layer at multiple time points.
The average Snellen logMar acuity in patients exhibiting the ellipsoid zone change was 0.404 (Snellen equivalent of 20/56, p=0.16 from baseline) at day 28 in comparison with the average Snellen logMar acuity in patients not experiencing ellipsoid zone change was 0.397 (Snellen equivalent of 20/57, p=0.60 from baseline).
The average central subfield thickness for responders was 253 µm at day 28 and the average central subfield thickness for non-responders was 387 µm at day 28. These values were statistically different from each other (p=0.05).
A total of five macular holes were found at baseline using the Gass staging criteria (Stage 3=one patient, Stage 2=two patients and Stage 1=two patients). Four of the five patients experienced resolution of their macular hole after injection. The patient with a Stage 3 full thickness macular hole at baseline demonstrated no resolution after injection and underwent conventional surgical repair.
Eleven patients were found to have CMO at baseline and were graded based on the CMO five-point grading scale (Grade 4=five patients, Grade 3=four patients, Grade 2=two patients). Two patients demonstrated complete resolution of CMO by days 1 and 7 post-injection. Six of the eleven patients demonstrated stable CMO grading without improvement or worsening of CMO post-injection. Three patients demonstrated decline in one grade of CMO. Six patients did not have CMO at baseline, of which one patient exhibited Grade 3 CMO at day 7 and day 28 post-injection.
Discussion
Patients treated with ocriplasmin in our series for sVMA experienced a 47.1% (8/17 eyes) resolution within 28 days post-injection. These results were better than seen in the overall outcomes from the MIVI-TRUST trials and support the efficacy of ocriplasmin in the treatment of sVMA. Reasons for a higher response in this study may include the use of positive predictive factors identified in the MIVI-TRUST trial in selecting patients for therapy, the use of SDOCT to monitor vitreomacular separation in comparison with TDOCT and potentially sampling as this was a much smaller cohort that what was studied within the phase III trial. Another retrospective study of 19 patients treated with ocriplasmin found similar results with careful case selection based on these characteristics and reported a similar (42%) adhesion release rate.5 As was shown in the pivotal trials, time to response occurred in the majority of patients within 7 days of initial injection with a trend showing improved macular oedema over time. Similar to the phase III trials, VA of the responders were better than the non-responders.
AEs were observed in this study and some were attributable to ocriplasmin. These side effects included photopsias and reduced VA, both of which were acute and temporary changes that resolved with VMA resolution. In the clinical trials of ocriplasmin, blurred vision, photopsias, dyschromotopsia and electroretinographic (ERG) changes occurred in a significantly greater number of patients receiving ocriplasmin versus those receiving a placebo (drug vehicle diluted with saline). ERG changes were also reported (a-wave and b-wave amplitudes decrease).1 ,2 Freund et al recently reported a case demonstrating changes seen in the outer photoreceptor segments by SDOCT.6 The disruption occurred in the ellipsoid zone and was reversible in this single case report. However, since the MIVI-TRUST trial used only TDOCT with inferior resolution to SDOCT, it is possible that these cases may have been overlooked.
In our series, almost all the patients who responded to the treatment had OS ellipsoid zone changes on the SDOCT. These patients also had transient acute VA reduction and demonstrated subretinal fluid during the release process with almost the exact time course as the loss of the OS ellipsoid zone. This finding may suggest a transient toxicity of ocriplasmin at the level of the outer retina and RPE possibly due to disruption of the photoreceptors. If this transient affect occurs for both rods and cones, it may explain the dyschromatopsia, contrast sensitivity changes, dark adaptation issues and ERG changes seen in the ocriplasmin clinical trials. All cases had eventual resolution of this fluid and return of the OS ellipsoid zone. Larger clinical studies employing SDOCT will be necessary to validate these initial findings.
Given the retrospective nature of the study, there are certain inherent drawbacks of the analysis conducted. While the ellipsoid zone losses and subretinal fluid occurrence have been confirmed, the time courses of these changes cannot be determined exactly since clinicians varied in their length of follow-up. As mentioned prior, the smaller cohort studied here might also have inherently had some selection bias leading to better outcomes than in the MIVI-TRUST trial. Finally, the use of standard Snellen acuity rather than protocol VA and short follow-up period might have blunted the VA outcomes. It was not uncommon to see delayed anatomical improvement in VA and anatomy within the MIVI-TRUST so this may account for these findings.
Despite the transient OCT changes noted, it appears that ocriplasmin has significant benefits in separating the posterior hyaloid in cases of sVMA and the rates of resolution appear to be better than in clinical practice. This is the first case series to quantify the percentage of patients noted to have these significant changes in their outer retinal structure. Future studies would help in elucidating the cause of these transient changes, which may better explain ocriplasmin's mechanism of action.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.