Article Text

Abstract
Aims This study explored the association of active acute anterior uveitis (AAU) with depressive feelings and patients’ general health.
Methods This case-control study comprised 80 participants: 35 patients with an active case of AAU and 45 healthy peers were analysed to compare their depressive moods (Beck depression inventory (BDI), Zerssen Mood Scale (ZMS)) and general health (Short form-8 health survey (SF8)). Furthermore, patients were questioned regarding the presence of distress, occupational satisfaction and impairment in performing daily life tasks.
Results During an acute attack, AAU patients were shown to suffer from depressive moods more often than their healthy peers (BDI 54% vs 9%, respectively; ZMS 2.7-fold shift in mood levels towards depression) and experienced a reduction in mental and physical scores (SF8). Patients felt impaired reading (94%), driving (69%) and working (69%). In all, 74% of the patients believed that distress was a probable trigger. Lack of occupational satisfaction was associated with a persistence of depressive feelings and a reduction in physical health.
Conclusions AAU patients exhibited a significant psychopathology towards depression, a reduction of general health and impairment of performing daily life tasks. Patients who were unsatisfied at work seemed to suffer even more. The results underline the importance of offering psychological support to the patients and providing information to patients and close social contacts.
- Immunology
- Inflammation
Statistics from Altmetric.com
Acute anterior uveitis (AAU) is a painful and vision-impairing eye disease that requires intensive treatment and close patient follow-up. Currently, the mainstay treatment is a topical anti-inflammatory and cycloplegic therapy, extended by topical steroid injections or systemic medication if necessary. The deterioration of visual acuity, pain, frequent application of eye drops and necessity of repeated visits to an ophthalmologist constitute a burden for the patient. In addition, patients are impaired in performing daily tasks, such as reading and driving, and face difficulties performing their jobs effectively. Many patients cannot be on sick leave for several days, or cannot leave work easily for scheduled control visits. Often, patients report a total lack of understanding of their diagnosis. Socially, uveitis remains a ‘red eye’ disease, raising the suspicion of hypochondria, laziness or a lack of enthusiasm for work. In cases of repeated attacks, patients visiting our uveitis clinic have reported being under considerable strain at their work place, and have a fear of losing their jobs.
The disease itself, the therapy and the interference with daily life cause distress. Distress is a term used by psychologists to describe negative forms of stress caused by wearing situations. By contrast with positive, pleasant forms of stress, so-called ‘eustress’, distress can induce depressive moods. In a previous study, we found a higher percentage of depression among 171 patients with a history of AAU.1 However, the majority of patients had inactive AAU. Only 13 suffered from an acute attack, exhibiting even higher depression scores. It was concluded that it is necessary to investigate the association of an active recurrence of AAU with depression and quality of life. Following these findings, the aim of the present study was to evaluate whether depressive feelings are frequent in active AAU and corroborate our hypothesis that there is a relevant impact on general health and the ability to perform daily life tasks. The results could provide further insight into the psychopathology of AAU.
Materials and methods
Patient and control group recruitment
This clinic-based, case-control study was performed between April 2010 and May 2012 at the Department of Ophthalmology of the Hietzing Hospital in Vienna, Austria. Thirty-five consecutive, previously untreated patients with an acute attack of anterior uveitis in one eye (anterior chamber inflammation graded ≥1 +cells according to the SUN criteria2), and 45 healthy peers were included in the study. The healthy peers had to meet the following inclusion criteria: no eye disease or serious chronic or current illness, and coming from the same geographical area. Beginning at an original peer group sample of 94 persons, a stratified matching was performed. A control group of 45 persons was calculated, matching for age, gender, ethnicity and educational level. Follow-up data for the control group were collected 6 months after the first assessment to prove that the values of healthy peers did not change over time. Institutional review board approval and informed consent were obtained in accordance with the Declaration of Helsinki.
The survey contained questions related to sociodemographic data and uveitis details. If not known previously, a spondyloarthropathy (SpA) was ruled out if a patient reported one of the two entry criteria of the European Spondylarthropathy Study Group guidelines3 (inflammatory spinal pain or synovitis that is either asymmetric or predominantly in the lower limbs), intestinal/skin/urogenital problems or a family history of SpA. Furthermore, patients were asked about the presence of distress or life events before an attack, occupational satisfaction and impairment in performing daily life tasks. The three psychometric instruments that were applied are listed below.
Psychometric instruments
The Beck Depression Inventory (BDI) is a self-report inventory for differentiation of a depressive mood and was the primary outcome variable.4 Twenty questions are asked to document the actual severity of depressive moods, indicated by a sum score (0–63 points). The sum score also is allocated to one of three clinically relevant groups: ‘not depressed’ (0–9 points), ‘minimal depressive mood’ (10–18 points) and ‘clinically relevant depressive mood’ (19–63 points).
The Zerssen Mood Scale (ZMS, Zerssen- BF-S’-Befindlichkeits-Skala) is a 28-item, subjective rating scale to measure the current psychological mental state.5 A sum score indicates the patient's present mood: ‘euphoric’ (0–6 points), ‘well-balanced’ (7–16 points), ‘aggrieved’ (17–26 points), ‘mildly to moderately depressive’ (27–41 points) and ‘pronounced to extremely depressive’ (42–56 points).
The Short Form-8 health survey (SF8) is an 8-item, self-rating measure evaluating a person's general health status over the past weeks.6 Domains measured are physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems and mental health. These are merged in two summary measures: the Physical (SF8-PCS) and the Mental Component Summary (SF8-MCS). Healthy controls should reach a mean score of 50±10. A higher/lower score indicates a better/worse level of functioning or general health.
The BDI, the ZMS and a visual analogue pain scale (VAS, ranging from 0 mm, indicating no pain at all, to 100 mm, indicating unbearable pain) were applied twice: at the patient's first visit before starting therapy (initial visit), as well as 8±2 weeks later (follow-up visit (f/u visit)). The SF8 was applied only once at the f/u visit. A f/u measurement could be obtained in all AAU patients and 36 healthy peers (80%). Anterior chamber inflammation according to the standardization of uveitis nomenclature criteria2 and best-corrected visual acuity (BCVA (Snellen/logMAR)) were recorded at both visits.
Sample size calculation
The sample size was calculated using the results of a previous study on patients with a history of AU.1 The inference for means was calculated with the BDI score as the primary outcome variable (patients with anterior uveitis=8.7, healthy controls=4.4), α=0.05, power=0.08, and a mean standard deviation of 6. A sample size of 31 patients was proposed.
Statistics
The SPSS 16.0 software was used for the statistical analysis. For the descriptive analysis, data were expressed as total numbers (n), percentage relating to group (%), and means±SD. The t test, analysis of variance, χ2-test, Mann–Whitney U test, or Wilcoxon rank-sum test were used as appropriate. Correlations were calculated using the Pearson's rank correlation method. The cut-off level for statistical significance was set at p<0.05; all tests were performed in a two-tailed manner. In case of multiple testing within a group, a Bonferroni–Holm correction was applied to adjust the p value.7
Results
The study included 80 subjects: 35 patients with an acute attack of anterior uveitis (AAU) with a gender distribution of female:male=1 : 1.7 (p<0.001; table 1), and 45 healthy controls (matched by age, gender, ethnicity, educational status; see Methods section). The AAU patients’ sociodemographic characteristics and other parameters evaluated are shown in table 1.
AAU patients’ sociodemographics, disease history, occupational satisfaction and distress as trigger
At the initial visit, the anterior chamber inflammation was counted as grade 1.8 cells (range 1–3) and 1.6 flare (range 1–4). Patients graded their pain to be 59±22 mm (range 19–92). At the f/u visit, cells and flare both dropped to grade 0.1 (range 0–0.5; p<0.001), and pain dropped to 2±1 mm (range 1–3; p<0.001).
Table 2 shows the results of the psychometric instruments, as obtained from the AAU patients and their peers. The seven AAU patients with an associated SpA did not differ from those without.
Results of the psychometric instruments applied to patients with AAU at the initial visit (before start of treatment) and the follow-up visit (8 weeks later), as well as those of the controls
Beck depression inventory
The mean sum score obtained in patients with AAU was significantly higher than the value obtained from controls (p<0.001, table 2), indicating a higher level of depressive mood. In all, 54% of AAU patients (n=19) vs 9% of controls (n=4) were classified to be outside the normal range. Thirteen AAU patients were in a ‘minimally depressive mood’, and six were in a ‘clinically relevant depressive mood’. The controls were scored as ‘normal’ or ‘minimally depressive’ (figure 1).

Percentages of AAU patients as allocated to the three clinically relevant BDI groups (no depressive mood—minimally depressive mood—clinically relevant depressive mood) at initial visit and follow-up visit, as well as the controls’ results. AAU, acute anterior uveitis; BDI, Beck Depression Inventory.
Females tended to have higher BDI sum scores than males, although the difference was not statistically significant (table 2). The BDI sum score obtained at the initial visit correlated well with the other mood scales (SF8-MCS, p<0.001, r=−0.6; ZMS, p<0.001, r=0.7) but was significantly lower than the SF8-PCS (p=0.029, r=−0.4). The BDI was not influenced by the pain level.
At the f/u visit, the drop in the BDI sum score was statistically significant (p<0.001) and was equal between females and males (p<0.01 each). The BDI sum score still was slightly higher in patients than in the peers, although the difference was not statistically significant (p=0.11). In all, 23% of AAU patients then were classified to be in a ‘minimal’ or ‘clinically relevant’ depressive mood (figure 1).
Zerssen Mood Scale
The mean ZMS score in AAU patients reached a value 2.7-fold higher than in the controls (30±14 and 11±10, respectively; p<0.001), indicating a high level of mood affection directing to depressive feelings. The allocation to the five clinically relevant groups is shown in figure 2.

Percentages of AAU patients as allocated to the five clinically relevant ZMS groups (euphoric; well-balanced; aggrieved; minimal and moderate depressive; markedly and extremely depressive) at initial visit and follow-up visit, as well as the controls’ results. AAU, acute anterior uveitis; ZMS, Zerssen Mood Scale.
At the f/u visit, the score had dropped (20±12, p<0.001) but was still higher than in controls (p<0.001). Female and male AAU patients did not differ in their results: both had a significant reduction in the score at the f/u visit (p<0.001 each). AAU patients with elevated ZMS scores also had impaired SF8-MCS scores (initial visit p=0.020, r=−0.4; f/u visit p=0.001, r=−0.5).
Short form-8 health survey (SF8)
Compared with controls, AAU patients had lower values on the SF8-PCS (p<0.001) and SF8-MCS scales (p<0.001), indicating an impairment in physical and mental health dimensions (table 2). Females did not differ from males (table 2).
Visual analogue scale
At the initial visit, females marked their pain level to be 69±20 mm on the VAS. Males indicated their pain to be at a lesser level (53±21 mm, p=0.040). In both genders, a higher pain level was associated with a higher number of sick days taken (p=0.027, r=−0.4). At the f/u visit, pain had improved significantly (p=0.001).
Visual acuity
Starting with a BCVA of 20/40 Snellen (0.3±0.4 logMAR, range 1.5 to 0), all patients improved to a BCVA of 20/20 (0.01±0.03, range 0.1 to 0) at the f/u visit. At the f/u visit, a better BCVA or a larger range of improvement was correlated with fewer sick leave days (r=0.4, p=0.012 and r=−0.4, p=0.010, respectively). At both visits, no correlation was found between the BCVA achieved and the scores of the BDI, ZMS or SF8.
Impairment in daily life
The majority of AAU patients reported having difficulties in reading (book or computer; n=33, 94%), and two-thirds had problems driving a car (n=24, 69%) or doing their job properly (n=24, 69%). One-third of patients (n=11, 31%) found it difficult to pursue sports or hobbies. Having difficulties concerning one of the tasks listed above was not associated with a significant difference related to the psychological questionnaires or any of the other parameters investigated.
Occupational satisfaction
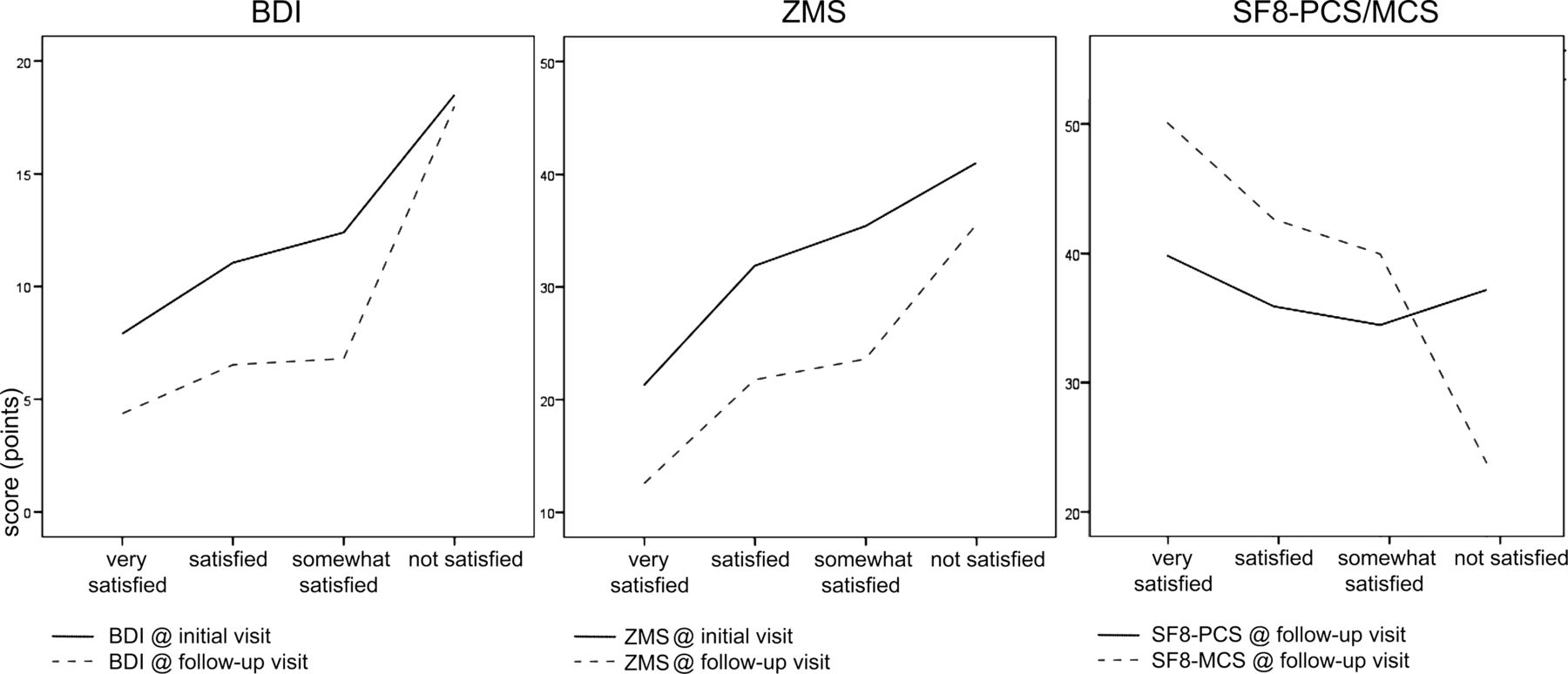
Lack of occupational satisfaction was associated with a persistence of depressive feelings even after healing of the AAU attack, indicated by elevated BDI and ZMS scores at the f/u visit (p=0.038 and p=0.037, respectively; figure 3). The scores ranged from BDI=4±4 and ZMS=13±7 in AAU patients who are very satisfied at their workplace to BDI=18±7 and ZMS=36±9 in those who are dissatisfied. The latter group also exhibited lower SF8-MCS values (p=0.006). SF8-MCS values ranged from 50±10 in very satisfied patients to 24±2 in dissatisfied patients (figure 3). Furthermore, the numbers of sick days taken increased with the level of dissatisfaction (p=0.005).

{kind=link}
{kind=link}
{kind=link}
Influence of AAU patients’ occupational satisfaction on the results of psychological questionnaires (BDI at initial and follow-up visit, ZMS at initial and follow-up visit, SF8 PCS and MCS at follow-up visit). AAU, acute anterior uveitis; BDI, Beck Depression Inventory; MCS, Mental Component Summary; PCS, Physical Component Summary; SF8, Short Form-8 health survey; ZMS, Zerssen Mood Scale.
Distress and/or life events as triggers for AAU relapses
In all, 74% of patients (n=26, p<0.004) had the impression that distress had an influence in triggering the AAU relapse (table 1). Six patients could state a specific life event after which the current attack had occurred. Patients who believed distress to be a possible AAU trigger did not differ from other patients concerning the BDI at the initial visit but had higher BDI scores at the f/u visit (distress=8±7, no distress=3±2, p=0.003). Patients with a subjective impression of distress as a trigger had higher ZMS scores at presentation compared with other patients (distress=33±14 vs no distress=19±15; p=0.010).
Discussion
This study explored the impact of active AAU related to depression (BDI, ZMS) and general health (SF8). We compared 35 patients with an acute case of AAU with 45 healthy control subjects matched by age, gender and educational level. AAU patients suffered from depressive moods more often than the controls (54% vs 9% according to the BDI, respectively) and had a higher level of depression compared with the controls (six AAU patients were classified as ‘clinically relevant depressive’ vs none of the controls). Similarly, AAU patients experienced a 2.7-fold shift in mood levels towards depressive feelings (ZMS).
The finding that patients with AAU have an increased risk of suffering from depressive feelings is consistent with the findings of our previous study. Patients with a history of recurrent B27-AAU were shown to have pathologically elevated BDI sum scores (8.7±7.0).1 A subgroup of 13 patients suffering from an acute flare during study participation scored even worse (11.3±7.7). The patients investigated in the current study showed comparable values, thus confirming the results of the preceding study and proving our hypothesis that AAU is associated with depressive feelings.
Impairment of general health in patients with AAU has also been reported previously by Carrim et al,8 wherein 42 patients were shown to achieve poorer scores on a general health questionnaire during a flare-up than did controls.
There are a variety of theories regarding why depressive moods might arise in a human being. Based on genetic susceptibility, disadvantageous personal living conditions, such as the loss of a loved one, the loss of employment or the development of a disease, are suspected to play a major role in depression. Illnesses associated with pain often are shown to be associated with depression.9 In this sense, the experience of a painful disease such as uveitis might influence the shift to a depressive mood. Another theory for the development of depressive moods in AAU patients is the so-called ‘gratification crisis’, caused by lack of recognition of an individual's efforts despite a great willingness to perform.10 Such situations can arise in a person's professional life or family or private life. The feeling of being short-changed can cause negative emotions and distress, which again may lead to depression. In the present study, patients with a lack of occupational satisfaction continued to suffer from depressive feelings (BDI and ZMS) and to exhibit low physical health (SF8-PCS). Moreover, they were also on sick leave longer than patients who were satisfied with their situation at work. Of course, we do not exactly know why some patients were not satisfied at their work place. A lack of understanding regarding their disease by their colleagues might be a possible explanation as to why unsatisfied patients continued to feel depressive, whereas those who were satisfied at work and felt understood by their colleagues understood may have experienced an improvement in mood. In 1994, Mayer et al11 published a paper on the psychosomatic aspects of uveitis in the context of work life. By interviewing 21 uveitis patients with a life-change scale, they found that psychological and social factors were perceived as triggers, especially those connected to patients’ work life. The authors concluded that there is a subjective importance of patients’ professional life on their flare-ups.
Independent of the time period that had elapsed since the uveitis diagnosis and how often it had recurred, AAU patients seemed to encounter serious problems in mastering their daily life during a flare-up. AAU patients reported a significant impairment concerning both physical health dimensions (SF8-PCS) and described problems in reading, driving and doing their daily work. Those with a higher physical impairment and a higher pain score also reported taking more sick days. The AAU patients still exhibiting a depressive mood at the 8-week f/u visit were those who are dissatisfied at work and those who believe distress to be a trigger.
In addition, a visual component must be taken into account when evaluating strains during an acute flare, composed of reduced visual acuity per se, reduced contrast sensitivity and increased glare. A recent study on patients with various forms of uveitis found an association between vision loss and depression.12
In conclusion, the results of the present study emphasise the increased risk of patients with an acute case of AAU of suffering from depressive moods and experiencing a reduction of the perception of their general health. Distress and patients’ work situation seem to play an important role as well. The sample size, and the restriction to the psychometric inventories chosen, have to be mentioned as limitations of the study. Although we calculated the required sample size, when interpreting the data, we found that a larger patient group would have been helpful in interpreting secondary outcome variables of occupational satisfaction, distress and triggers. It is also important to acknowledge the problem of retrospective recall bias. Patients are more likely to remember stressful events when they are suffering an acute event, such as a uveitis flare-up, because they are thinking about triggers for their attack. A prospective log of stressful events in patients with AAU would be a thorough way to obtain further insight into this topic. Moreover, the current data make it impossible to draw any conclusions concerning patients with an underlying SpA. Not every patient was sent for a rheumatologic check-up, only those with complaints suspicious of a SpA. Nevertheless, we believe that if a SpA was missed in our patients because it is subclinical and causes no complaints, then this also should not be relevant concerning general health and depression.
As most of the patients affected by AAU are in the prime of their life, it is important to offer support for avoidable or treatable psychological impairment. Information about the disease, its relapsing nature and its imminent impact on psychological well-being should be provided to patients and also close social contacts (eg, family members, friends, supervisors and colleagues). Specialists should be conscious of and alert to the probable depressive reactions of their patients and foster an interdisciplinary management plan, including psychological counselling or guidance.
Acknowledgments
The authors would like to thank K Gruber (University of Economics, Vienna) and AW Schiesser (Sigmund Freud University, Vienna) for their kind advice on specific questions concerning the use and interpretation of the psychological questionnaires used.
Footnotes
-
Collaborators K Gruber; A W Schiesser.
-
Contributors SM: conception and design. SM: execution of the study. SM, JW: analysis and interpretation of data. SM: drafting the article. JW, BW, VV: revising it critically for important intellectual content. SM, JW, BW, VV: final approval of the version to be published.
-
Competing interests None.
-
Ethics approval Ethics Committee of the City of Vienna.
-
Provenance and peer review Not commissioned; externally peer reviewed.