Article Text

Abstract
Background/aims To review the indications and types of keratoplasty performed in the West of Scotland between 2001 and 2010.
Methods A retrospective analysis of the histopathological diagnoses of all corneal buttons submitted to the regional Ocular Pathology Laboratory (Glasgow, UK) between January 2001 and December 2010 was performed.
Results Between 2001 and 2010, a total of 921 keratoplasties were performed in the West of Scotland. These included 646 (70.1%) penetrating keratoplasties and 275 (29.9%) lamellar keratoplasties (LK). Keratoconus (n=264, 28.7%) was the leading indication for keratoplasty, followed by graft failure (n=177, 19.2%), Fuch's endothelial dystrophy (n=124, 13.5%), keratitis (n=106, 11.5%), pseudophakic/aphakic bullous keratopathy (n=88, 9.6%), endothelial failure (n=67, 7.3%), non-Fuch's corneal dystrophies (n=21, 2.3%), trauma (n=19, 2.0%), autoimmune/inflammatory diseases (n=16, 1.7%) and others (n=39, 4.2%). A significant increase in the proportion of LK over penetrating keratoplasty was observed during this 10-year period: from 14.1% LK (2001–2005) to 40.4% LK (χ2=71.78, p value<0.001).
Conclusion Keratoconus was the leading indication for keratoplasty in the West of Scotland. Both anterior LK and endothelial keratoplasty seemed to show an emerging trend as the procedures of choice for dealing with anterior and posterior corneal pathologies, respectively.
- Keratoplasty
- lamellar keratoplasty
- indication
- keratoconus
Statistics from Altmetric.com
Introduction
Ever since the first successful keratoplasty was performed more than a century ago,1 the field of keratoplasty has undergone rapid evolution.2–4 Currently, keratoplasty is one of the most commonly performed transplantations worldwide. According to the statistics of the Eye Bank Association of America and the UK National Health System Blood and Transplant (NHSBT), approximately 40 000 and 2000–3000 keratoplasties were performed in the USA and the UK each year, respectively.5 6
Until recently, penetrating keratoplasty (PK) was the predominant surgical modality over lamellar keratoplasty (LK) because LK—a procedure that aims to remove and replace only the diseased corneal layers—is a highly skilled procedure, and the limitations of technology and microsurgical techniques can result in suboptimal visual outcome and a higher risk of complications.7 However, a few studies have demonstrated that the long-term corneal graft survival rates following PK were unsatisfactory, attributed mainly to the endothelial immunological allograft rejection and the continual loss of the endothelial cells from the donor cornea.8 9
This explains why LK has increasingly been valued in the recent years because it obviates the need to replace healthy corneal endothelium in isolated anterior corneal pathologies, which then eliminates the risk of endothelial rejection.2 3 In addition, continuous refinement in microsurgical techniques and instrumentation10 11 have overcome the inherent technical barrier of using LK. However, there are few studies available in the literature reporting the resurgence of LK12 13 and, so far, there was none performed in the West of Scotland.
In addition, it is interesting to note that the indications for keratoplasty can vary considerably across different regions and time.13–16 For instance, Kang et al17 reported graft failure as the emerging leading indication for keratoplasty in certain part of US over a 20-year period. The latest study examining the indications for keratoplasty in the West of Scotland was performed as far back as 15 years ago,18 highlighting the need for an updated examination of the indications for keratoplasty in this region.
In light of the changing trend in keratoplasty, our study aimed to review the indications and the types of keratoplasty employed in the West of Scotland between 2001 and 2010.
Materials and methods
A retrospective analysis of the histopathological records of all corneal buttons submitted to the regional Ocular Pathology Laboratory (Western Infirmary, Glasgow, UK) between January 2001 and December 2010 was performed. From a computerised histopathological database (Telepath), data pertaining to the demographic factors, the indications and the types of keratoplasty performed, and the histopathological diagnoses of the recipient corneal button were collected and analysed.
Types of keratoplasties were grouped into PK and LK. LK was further subcategorised into deep anterior lamellar keratoplasty (DALK) and Descemet's stripping automated endothelial keratoplasty (DSAEK). In addition, indications for keratoplasty were classified into ten main groups: keratoconus, graft failure, Fuch's endothelial dystrophy (FED), aphakic/pseudophakic bullous keratopathy (ABK/PBK), keratitis, endothelial failure, non-Fuch's corneal dystrophies (NFCD), trauma, autoimmune/inflammatory diseases and others. Diagnoses that were undetermined by the histopathological examination were grouped under ‘others’. Arbitrarily, indications were subgrouped into anterior, posterior and mixed corneal pathologies for analytical purposes. Anterior corneal pathologies include keratoconus, keratitis, NFCD and inflammatory diseases,whereas posterior corneal pathologies include FED, ABK/PBK and endothelial failure. The rest were considered as mixed corneal pathologies.
The study period was divided into 2001–2005 and 2006–2010 for descriptive and analytical purposes. An χ2 contingency table testing of the observed frequency of types of keratoplasty between the two time periods was performed. A p value of <0.05 was considered statistically significant.
Results
A total of 921 keratoplasties were performed between January 2001 and December 2010 in the West of Scotland: mean age 55.62 (range 9–100) years, 57.1% male.
Types of keratoplasty
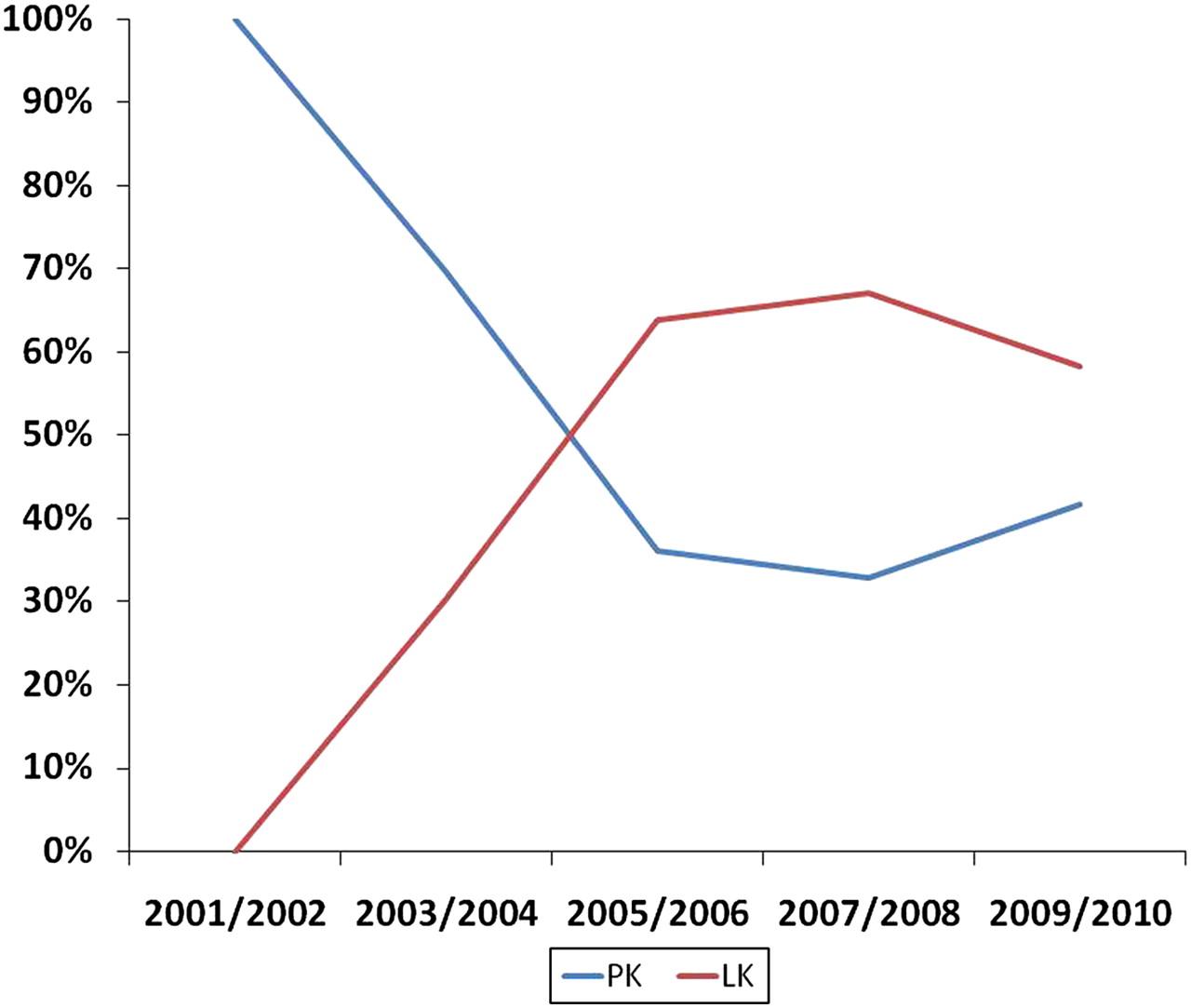
Of the 921 keratoplasties, 646 (70.1%) were PK and 275 (29.9%) were LK. The latter group comprised 225 (24.4%) DALK and 50 (5.5%) DSAEK (figure 1). Proportions of PK and LK, encompassing both DALK and DSAEK, during this 10-year period are plotted in figure 2. In 2001–2005, there were 317 (85.9%) PK, 52 (14.1%) DALK and 0 (0%) DSAEK procedures. However, during 2006–2010, a dramatic increase in DALK (173, 31.3%) and DSAEK (50, 9.1%) with a corresponding decrease in PK (329, 59.6%) was observed. Overall, there was a significant trend towards the use of LK over PK during this 10-year period: from 14.1% LK (2001–2005) to 40.4% LK (2006–2010) (χ2=71.78, p<0.001).

Numbers of penetrating keratoplasty (PK), anterior lamellar keratoplasty (ALK) and endothelial keratoplasty (EK) employed in each year.

Proportions of penetrating keratoplasty (PK) and lamellar keratoplasty (LK) (including both anterior lamellar keratoplasty and endothelial keratoplasty) performed during 2001–2005 and 2006–2010.
Common indications for keratoplasty
The distributions of the corneal diseases requiring keratoplasty between 2001 and 2010 are shown in table 1. During this 10-year period, keratoconus (264, 28.7%) was the leading indication for keratoplasty, followed by graft failure (177, 19.2%), FED (124, 13.5%), keratitis (106, 11.5%), ABK/PBK (88, 9.6%), endothelial failure (67, 7.3%), NFCD (21, 2.3%), trauma (19, 2.0%), autoimmune/inflammatory diseases (16, 1.7%) and others (39, 4.2%). The final group included non-specific corneal scarring (10, 1.1%), aniridia-related keratopathy (7, 0.8%), stem cell deficiency (3, 0.3%), iatrogenic (3, 0.3%), iridocorneal endothelial syndrome (2, 0.2%), severe band keratopathy (2, 0.2%), pellucid marginal degeneration (2, 0.2%), and unknown causes (10, 1.1%).
Distributions of corneal diseases requiring keratoplasty during 2001–2005 and 2006–2010
Comparing between the two time periods, the leading indications for keratoplasty remained rather consistent. During the first time period (2001–2005), the leading indications for keratoplasty were keratoconus (92, 24.9%), graft failure (70, 19.0%) and ABK/PBK (50, 13.6%). Similarly, in the second time interval (2006–2010), the leading indications remained as keratoconus (172, 31.2%) and graft failure (107, 19.4%), except that the third most common indication shifted from ABK/PBK to FED (80, 14.5%).
Proportions of LK employed for each indication
Between 2001 and 2010, 225 (24.4%) DALK and 50 (5.5%) DSAEK were employed. Keratoconus (136, 60.4%) and FED (29, 58%) were shown to be the most common indications for DALK and DSAEK, respectively (table 2). From the first to the second time period, there was a significant increase in the number of DALK procedures for keratoconus (from 27 (29.3%) to 109 (63.4%)), keratitis (from 11 (23.9%) to 27 (45%)) and NFCD (from 2 (20%) to 9 (81.8%)). Similarly, increased use of DSAEK was observed in FED (from 0 (0%) to 29 (36.3%)) and ABK/PBK (from 0 (0%) to 8 (21.1%)) over the two time intervals. Figures 3 and 4 illustrate the changing trend of keratoplasty for keratoconus and FED, respectively.
Proportions of lamellar keratoplasty (LK) employed for different indications during 2001–2005 and 2006–2010

Proportions of penetrating keratoplasty (PK) and deep anterior lamellar keratoplasty (DALK) performed for keratoconus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportions of penetrating keratoplasty (PK) and endothelial keratoplasty (EK) performed for Fuch's endothelial dystrophy.
Discussion
To the best of our knowledge, our study provides the first detailed report on the trend of keratoplasty in the West of Scotland. We also update the common indications for keratoplasty in this region that were last published in 1997.18 Our study observed that there was a significant increase in DALK and DSAEK in the West of Scotland: from 14.1% and 0% (in 2001–2005) to 31.3% and 9.1% (in 2006–2010), respectively (χ2=71.78, p<0.001). This finding parallels the changing trend reported in other countries such as the UK and China.12 13 Keenan et al,13 who investigated the changing trend of keratoplasty in the UK, have reported that there was a significant increase in DALK (from 4% to 13%) and endothelial keratoplasty (EK) (from 0.1% to 23%) activities from 1999/2000 to 2008/2009. Comparing our findings with the published NHSBT data, it appears that the corneal surgeons in the West of Scotland have been keeping up with the changing trend of keratoplasty. In fact, there were considerably more DALK activities in this particular region (31.3% in 2006–2010) compared with the rest of the UK (13% in 2008/2009). This was mainly due to an overall increase of DALK activities in the majority of isolated anterior corneal pathologies in the second time period (2006–2010), including keratoconus (from 29.3% to 63.4%), keratitis (from 23.9% to 45%) and NFCD (from 20% to 81.8%). In addition, during this 10-year study period, we found that as many as 407 (44.2%) cases of keratoplasty were for isolated anterior corneal pathologies, which might explain the much higher rate of DALK procedure in this particular region.
The preference for DALK observed in recent years is mainly attributable to the improved understanding of endothelial allograft rejection and the advancement in microsurgical techniques and instruments.2–4 8 9 One of the key advantages of performing DALK instead of PK is that the former obviates the unnecessary need of replacing the healthy endothelium in anterior corneal pathologies. This eliminates the risks of endothelial graft rejection and continual loss of endothelial cells of the donor cornea—major factors in graft failure following PK.8 9 In addition, comparable outcomes of the visual acuity and postoperative astigmatism between DALK and PK have been reported in many studies.19 Nonetheless, the outcome of DALK may be undermined by the surgeons' experience as DALK is a highly skill-demanding procedure.20 Therefore, it will be interesting to investigate the outcome of these two surgical approaches in the future when the steep learning curve of DALK is overcome.
In addition to the favourable short- and long-term outcomes, DALK can substantially increase the numbers of potential donor corneas being used as only the anterior portion of the donor cornea is required for DALK. This means that donor corneas with endothelial pathology or low endothelial cell density can still be used for DALK. Muraine et al21 investigated the impact of the DALK on the eye bank activity in France and reported that as many as 72.7% of the donor corneas that were unsuitable for PK were used for DALK, considerably increasing the overall keratoplasty activity. This finding should be emphasised because there has been a limited supply of donor corneas in many countries over the past decade, including the UK.5 By employing DALK, it should reduce the pressure on the limited supply of donor corneas in the eye bank.
Similarly, an increase in EK activity was observed in the West of Scotland from 2001–2005 (0%) to 2006–2010 (9.1%)—albeit slowly. In comparison with the NHSBT data, which reported a 22.9% increase from 1999/2000 to 2008/2009 in the UK, our study reported a relatively lower EK activity. We observed that the numbers of EK procedures only started to increase in 2008 following the appointment of a corneal surgeon experienced in DSAEK procedure. Nonetheless, we observed a gradual increase in the total numbers of DSAEK employed in the following 2 years (2009 and 2010), suggesting that this technique has been increasingly valued. In addition, we found that isolated posterior corneal pathologies—including FED, ABK/PBK and endothelial failure—only constituted 279 (30.3%) of all indications during this 10-year study period. This may account for the relatively lower EK activities in this region because there were less suitable cases for EK and less training opportunities for the surgeons to master this challenging technique.
Keratoconus was consistently the leading indication in this particular region during this 10-year period (264, 28.7%). This finding was similarly reported in other countries such as Saudi Arabia22 and Italy.23 However, it is interesting to note that the indications for keratoplasty can vary considerably across different regions.14–16 For instance, the most common indication for keratoplasty in a certain part of US was noted to be pseudophakic bullous keratopathy (27–28%) followed by graft failure (18–22%),24 whereas another study conducted in north China reported keratitis as the most common indication for keratoplasty.16 In addition, even in the same region, the indications for keratoplasty can also change over time. In the previous study, it was shown that the leading indication between 1990 and 1995 in the West of Scotland was ABK/PBK,18 instead of keratoconus observed in our current study. The decreasing trend for ABK/PBK was similarly observed in other studies.17 25 This interesting trend could be explained by the rapid advancement in the microsurgical technique in cataract surgery.
Such heterogeneity of the indications across different regions and time has highlighted the importance of an up-to-date examination of the indications for keratoplasty in a specific area. First, it can facilitate the researchers and clinicians in gaining a better insight into how the limited resources—donor corneas—are being used in a specific region. Second, the search of alternative therapeutic strategies over keratoplasty can be directed towards the more prevalent refractory corneal diseases.
Over this 10-year period (2001–2010), keratoconus was shown to be the most common indication for keratoplasty in the West of Scotland. More compellingly, there has been a significant move to the use of DALK and EK in this particular region, especially for keratoconus and FED, respectively. It will be interesting to follow-up the long-term outcome of these changes in keratoplasty technique over the next decade.
References
Footnotes
Funding None.
Competing interests None to declare.
Provenance and peer review Not commissioned; externally peer reviewed.