Article Text

Abstract
Objective To evaluate minor salivary glands and labial mucous membrane graft in patients with severe symblepharon and dry eye secondary to Stevens–Johnson syndrome (SJS).
Methods A prospective, non-comparative, interventional case series of 19 patients with severe symblepharon and dry eye secondary to SJS who underwent labial mucous membrane and minor salivary glands transplantation. A complete ophthalmic examination including the Schirmer I test was performed prior to and following surgery. All patients had a preoperative Schirmer I test value of zero.
Results Nineteen patients with severe symblepharon and dry eye secondary to SJS were included in the study. There was a statistically significant improvement in the best spectacle-corrected visual acuity in eight patients (t test; p=0.0070). Values obtained in the Schirmer I test improved significantly in 14 eyes (73.7%) 6 months following surgery (χ2 test; p=0.0094). A statistically significant increase in tear production (Schirmer I test) was found in eyes that received more than 10 glands per graft compared with eyes that received fewer glands (χ2 test; p=0.0096). Corneal transparency improved significantly in 11 (72.2%) eyes and corneal neovascularisation improved significantly in five eyes (29.4%) (McNemar test; p=0.001 and p=0.0005). The symptoms questionnaire revealed improvement in foreign body sensation in 53.6% of the patients, in photophobia in 50.2% and in pain in 54.8% (Kruskal–Wallis test; p=0.0167).
Conclusion Labial mucous membrane and minor salivary glands transplantation were found to constitute a good option for the treatment of severe symblepharon and dry eye secondary to SJS. This may be considered as a step prior to limbal stem cell and corneal transplantation in these patients.
- Mouth mucosa
- salivary glands
- entropion
- transplantation
- tears
- ocular surface
Statistics from Altmetric.com
Introduction
Stevens–Johnson syndrome (SJS), also known as erythema multiforme major, is an acute inflammatory reaction involving the skin and mucous membranes, characterised by the eruption of vesicles and bullae, with cicatricial abnormalities developing in the affected areas during the healing phase. The syndrome is commonly associated with a causative agent, usually a drug or an infectious process.1
Ocular involvement occurs in about two-thirds of cases and consists of severe mucopurulent, membranous or pseudomembranous, diffuse, bilateral conjunctivitis. The troubling ophthalmic complications occur during the chronic recovery phase. The conjunctival inflammation with membrane or pseudomembrane formation may lead to cicatricial changes in the conjunctiva and destruction of the limbal epithelial stem cells, resulting in symblepharon, entropion, trichiasis, tear film abnormalities, keratinisation and corneal neovascularisation.2 3
Management of the acute ocular process requires the use of both oral and topical steroids. Additional procedures that may be carried out include the aggressive use of doughnut-shaped conformers, daily lysis of adhesions, and the introduction of plastic wrap or amniotic membrane into the fornix to prevent the formation of symblepharon. Long-term management includes the use of topical lubricants to supplement the patient's tear production as well as surgical correction of entropion, trichiasis and symblepharon. Limbal stem cell and corneal transplantation may be indicated in cases in which there is a total limbal stem cell deficiency and corneal opacification. However, the development of severe dry eye and cicatricial changes often jeopardises functional and visual outcome.4
Denig (1911) was the first to describe mucous membrane grafting for the treatment of symblepharon.5 6 Since then, mucous membrane grafting has been popularised as one of the most effective methods of treating different eyelid and conjunctival disorders such as symblepharon, entropion, ectropion and pterygium.
The use of salivary glands as a source of lubrication to treat severe cases of dry eye has been advocated since 1951, when it was proposed by Filatov and Chevaljev, who described transplantation of the Stensen's duct in the parotid gland to the conjunctival fornix with the objective of replacing tears with salivary secretion. However, complications such as excess tearing and parotiditis limited its functional outcome.7
In 1986, Murube-del-Castillo proposed the submandibular gland transplantation as a better and less invasive alternative.8 In 1997, that same author described transplantation of a minor salivary gland as an option for the treatment of severe dry eyes.1 9 Minor oral salivary glands exist in large numbers in the labial, buccal and palatal mucosa, and account for approximately half the baseline secretion of saliva. They can be transplanted together with the overlying mucosa as a complex graft to the posterior lamella of the eyelids in other to increase ocular surface and reduce discomfort in patients with dry eye.
The purpose of the present study was to evaluate salivary gland and labial mucous membrane graft in patients with severe symblepharon and dry eye secondary to SJS.
Patients and methods
In this prospective, non-comparative, interventional case series, patients who had developed sequelae to the ocular surface and severe dry eye secondary to SJS were recruited from the Cornea and External Diseases and Oculoplastic Unit of the Federal University of Sao Paulo, Sao Paulo School of Medicine, Sao Paulo, Brazil, between 2006 and 2009.
Only patients with poor visual acuity, 20/100 or worse, and a Schirmer I test result of zero were included in the study. When it proved impossible to place the paper strip of the Shirmer test in eyes with symblepharon or ankyloblepharon, the test was considered not measurable.
Of all patients with SJS attending the clinic, only those with a Schirmer test of zero were selected for inclusion in the study. If the Schirmer test was zero in both eyes, the eye in which symblepharon was worse, in which visual acuity was poorer and in which keratinisation was greater was selected. Exclusion criteria consisted of any active infection and corneal melt or perforation.
Surgical procedure
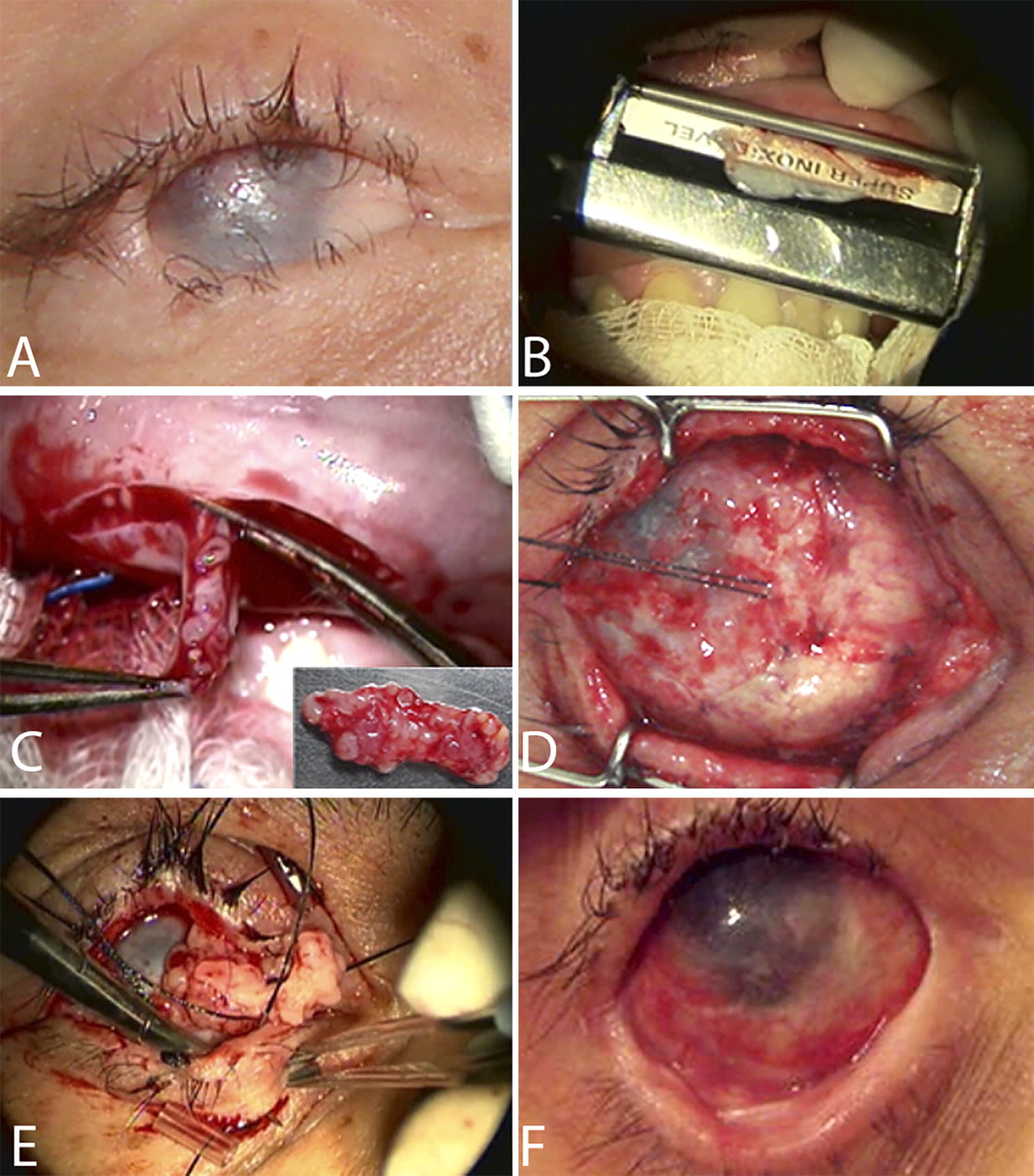
The same surgeon (AEBPPS) operated all the patients and general anaesthesia was used in all cases. A mucotome (Ficas Mucotome, São Paulo, Brazil) was used to obtain a thin split-thickness graft to correct symblepharon. Minor salivary glands were obtained en block from the mucous membrane of the patient's own upper or lower lip, above the orbicularis oris muscle. The thin split-thickness graft of mucous membrane was sutured to the sclera using absorbable sutures (poliglactyn, 8-0). The minor salivary glands, attached to the submucosa, were sutured in the superior and inferior conjunctival fornices using absorbable sutures (poliglactyn 8-0) and a transpalpebral 4-0 silk suture. At the end of the procedure, a scleral shield was placed over the eye and central blepharorraphy was performed (figure 1).
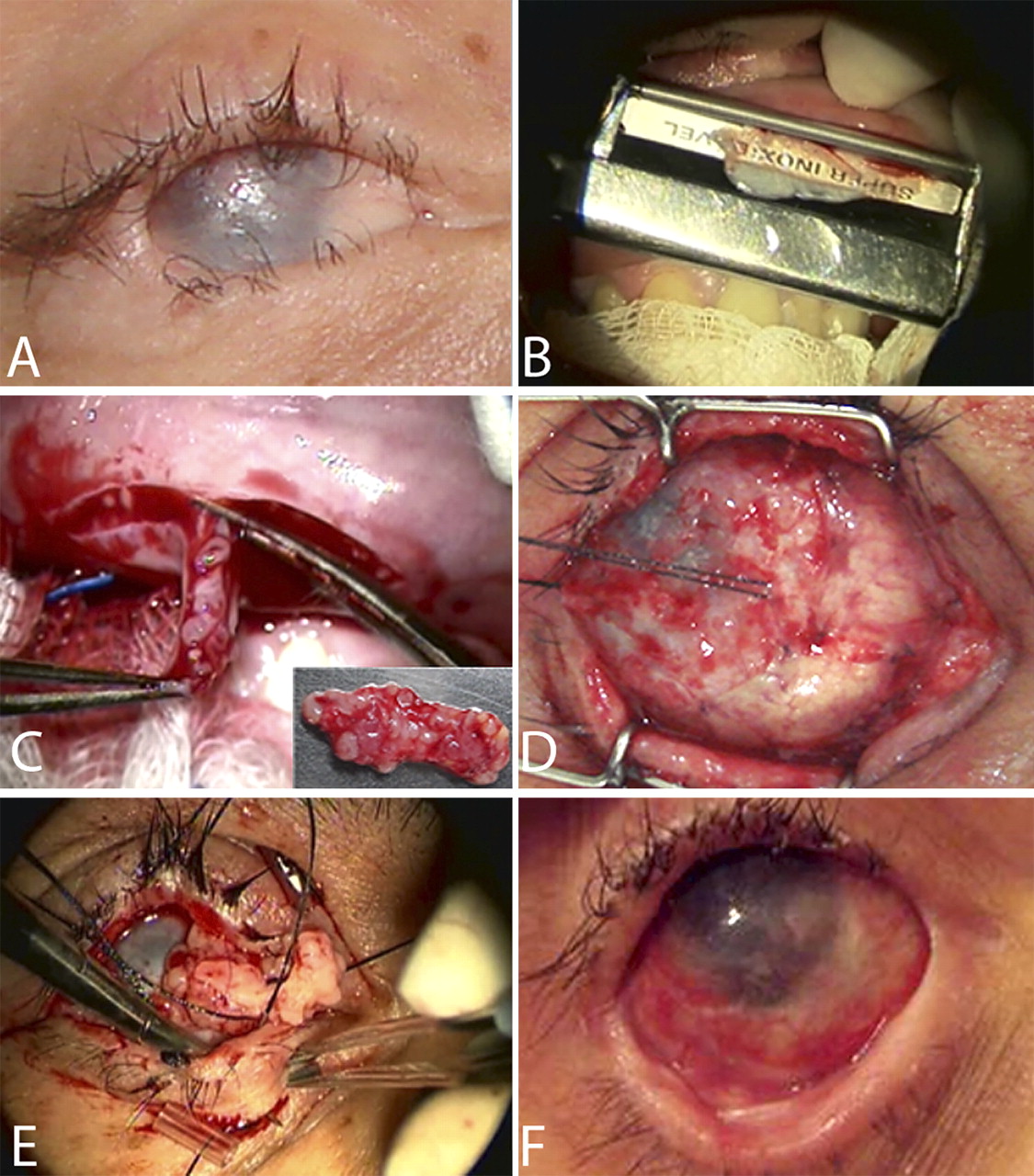
Surgical steps: (A) preoperative; (B) obtaining mucous membrane graft from the lower lip using a Ficas mucotome; (C) obtaining the salivary glands; (D) labial mucous membrane attached to the sclera; (E) fixing the salivary glands; (F) postoperative.
The following day, the blepharorraphy was opened and patients were instructed to use eye drops containing dexamethasone 0.1% and tobramycin 0.3% four times daily for 7 days. After this period the medication was gradually reduced over the following 3 weeks until the first removal of the scleral lens 1 month after surgery. Patients were then instructed to return to the clinic at weekly intervals, at which time the sclera lens was removed, rinsed with saline solution and replaced. Cold saline compresses were prescribed postoperatively for 1 month, and patients were instructed to apply them more often in the first 2 days after surgery.
The absorbable sutures (poliglactyn, 8-0) were removed after 7 days and the transpalpebral 4-0 silk suture was removed after 15 days.
It is worth mentioning that this technique differs from that used by other authors, since in this clinic the treatment of symblepharon and minor salivary gland transplantation is performed as a single surgical procedure.
Pre- and postoperative evaluation
A complete ophthalmic examination including Schirmer I test, slit lamp examination, funduscopy whenever possible (if impossible ocular ultrasonography was then performed) and measurement of intraocular pressure (using a Goldman tonometer or finger tension) was performed prior to surgery, and 1 and 6 months following surgery. Clinical photographs were also taken before and after surgery.
The visual acuity of the patients was evaluated before and after surgery using decimal notation. It the case of patients were unable to see the visual acuity charts from a distance of 1 m, visual acuity was assessed by asking them to count the number of fingers shown by the examiner. If they were unable to do this, visual acuity was then recorded as the ability to see the examiner's hand movements or, in the worse cases, the ability to perceive light projected into the eye.10 11
Corneal transparency was evaluated and graded as: 1, completely transparency; 2, hazy; 3, iris partially visible; 4, iris not visible. Vascularisation of corneal surface was monitored photographically and graded according to its extent and intensity; grade 1 indicating peripheral vascularisation; grade 2, peripheral and midperipheral vascularisation; grade 3, modest vascularisation, involving the entire cornea; and grade 4, massive vascularisation of the entire cornea.12
Patients were requested to complete a questionnaire on symptoms such as foreign body sensation, dryness, photophobia, pain and itching, and eye movements, indicating to what extent the symptoms had improved following surgery compared with before surgery. Answers were given on a scale from 0 to 5 for each symptom, with 0 representing hardly any improvement and 5 representing great improvement.13
Six months after surgery, these patients were referred for the next step: to evaluate reconstruction of the ocular surface with limbal and corneal transplants.
Statistical analysis
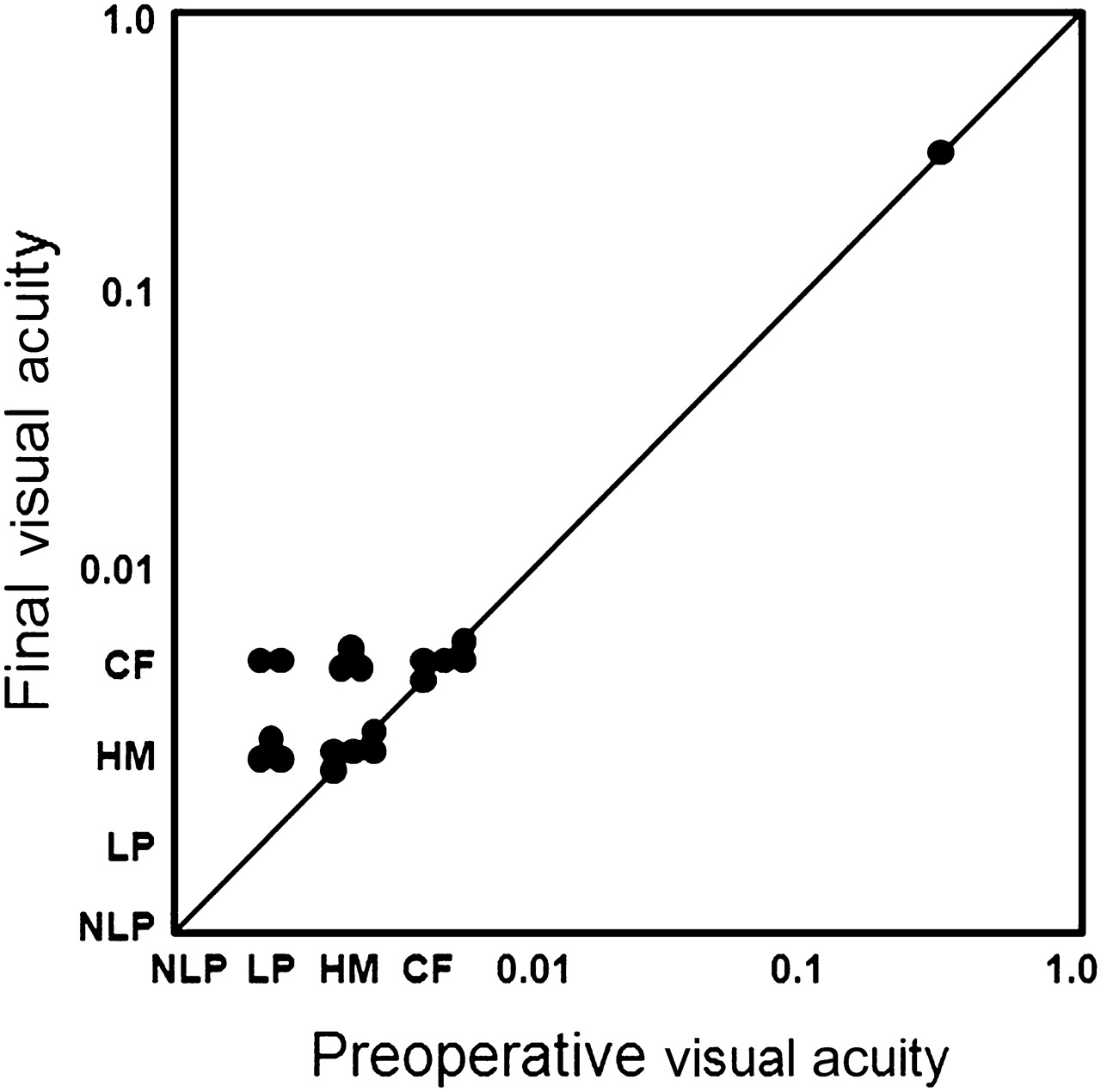
For purposes of statistical analysis, counting fingers was rated as acuity of 0.004, the perception of hand motion as 0.002 and the perception of light as 0.001, whereas no perception of light was ranked as 0.0001. Final postoperative visual acuity was defined as the visual acuity measured at the most recent visit. These values were compared with preoperative values using the non-parametric Wilcoxon signed-rank test.10
The statistical tests used to compare variables between two groups were McNemar test of paired proportions, the χ2 test with Yates' correction for proportions, Student t test and analysis of variance. The SPSS statistical software program, version 12 (SPSS Inc., Chicago, Illinois, USA) was used to perform statistical analysis. p Values <0.05 were considered statistically significant. The Bonferroni correction was used for repeat tests to correct for cumulative type I errors.
Results
Nineteen patients with severe symblepharon and dry eye secondary to SJS were included in the study. Mean age of patients was 31.5±13.9 years (mean±SD).
Of the 40 patients diagnosed with SJS and registered at corneal diseases unit of the Federal University of São Paulo only those with severe symblepharon and a Schirmer I test of zero were selected; however, the rarity of the disease did not allow patient selection to be limited exclusively to those who had not undergone any previous surgery.
All patients were submitted to unilateral surgery and there were no serious intraoperative complications. Two patients developed hypoesthesia of the lower lip, which improved within 5 months, and one patient had graft decentration that required a second surgical procedure 2 weeks later. In addition, a second procedure was required in six patients (31.6%) to correct residual symblepharon and the cicatricial entropion, while one patient (5.3%) had to undergo a third surgical procedure to correct the residual entropion.
Although the surgical procedure to correct symblepharon was performed at the same time as transplantation of the minor salivary glands at the same donor site, this had no negative effect on the final outcome of surgery.
There was a statistically significant improvement in the best spectacle-corrected visual acuity in eight (42.1%) of the 19 patients after surgery (paired simple t test; p=0.0070) (table 1, figures 2 and 3).
Outcome of salivary gland and labial mucous membrane transplantation in the treatment of severe symblepharon and dry eye in patients with Stevens–Johnson syndrome

Preoperative (A, C, E, G) and postoperative (B, D, F, H) pairs of photographs in five patients.

{kind=link}
{kind=link}
{kind=link}
Preoperative versus final visual acuity. CF, counting fingers; HM, hand movements; LP, light perception; NLP, no light perception.
Schirmer I test values improved significantly in 14 eyes (73.68%) when evaluated 6 months after surgery (χ2 test; p=0.0094). In one case, the Schirmer I test improved from 0 to 11 mm in the first month after surgery. In five eyes, the Schirmer I test result was still zero.
Ten of the 19 patients (52.6%) received 10 salivary glands or fewer in the submucosal graft, while nine patients (47.4%) received more than 10 glands. A statistically significant increase in tear production (according to Schirmer I test) was found in eyes that received more than 10 glands per graft compared with eyes that received fewer glands (χ2 test; p=0.0096) (table 2).
Schirmer I test (without anaesthesia) 6 months postoperatively
Corneal transparency improved significantly in 11 (72.2%) out of 18 eyes, decreasing in severity from grade 4 to grade 3 within 6 months of surgery (McNemar tests on paired proportions; p=0.001) (table 3). Similarly, corneal neovascularisation improved significantly in 5/17 eyes (29.4%), which decreased in severity from grade 4 to grade 3 within 6 months of surgery (McNemar test on paired proportions; p=0.0005) (table 4).
Corneal transparency
Corneal neovascularisation
Eighteen of the 19 patients (94.7%) completed the questionnaire on symptoms in which foreign body sensation, dryness, photophobia, pain and eye movements were evaluated individually (table 5). An improvement was found in foreign body sensation in 53.7% of the patients, in photophobia in 50.2% and in pain in 54.8% of the patients (Kruskal–Wallis test; p=0.0167) (table 5).
Symptoms questionnaire results
Discussion
Murube-del-Castillo8 was the first to describe mucous membrane and minor salivary gland transplantation for the treatment of severe cases of dry eye syndrome.6 Soares and França described a successful outcome with the same surgical treatment in 21 cases of severe dry eye, 12 (57.1%) of which occurred secondary to SJS. Surgery consisted of transplantation of salivary glands to the superior conjunctival fornix, with graft survival and integration into the host tissue in 97.2% of cases.14 In the present study, only patients with SJS were analysed and salivary glands were implanted into the superior and inferior conjunctival fornix. All grafts were still intact 6 months following surgery.
Several authors have presented different techniques for the treatment of symblepharon using substitutes for conjunctiva that range from alloplastic material such as polytetrafluoethylene to nasal or amniotic membranes, egg membrane, rectal mucosa, preputial mucosa and maxillary sinus mucosa. The most popular technique is the use of oral mucosa and the outcome is successful in about 85–100% of cases of symblepharon. In the present study, symblepharon was corrected with the use of oral mucous membrane graft.5 6 15–25
One of the difficulties found in operating on these patients was the cicatricial changes found in their eyes and oral mucosa, which were probably caused by the disease itself and by previous surgeries (18 of the 19 patients reported having previous surgeries to corrected symblepharon, trichiasis and entropion). It is possible that if this surgery had been performed in naïve eyes, more salivary glands could have been transplanted, with less conjunctival cicatrisation and a better outcome.
It was surprising that the number of salivary glands was sufficient for transplantation in more than 50% of the patients with SJS in the present study. Compared with cicatricial diseases, prognosis may be poorer in the case of diseases such as Sjögren's syndrome that affect the salivary glands. SJS and ocular cicatricial penphigoid are more severe than Sjögren's syndrome because of the cicatricial changes.
The Schirmer I test improved in 14/19 eyes (73.7%). Greater tear production was observed in patients who received submucosal grafts containing more than 10 glands. Although difficult to estimate, it is reasonable to assume that this variable would interfere directly with clinical outcome and this assumption was confirmed by the finding in the present study that lubrication was better in eyes that received more glands per graft.
Corneal transparency and neovascularisation improved in 11/19 eyes (72.2%) and 5/19 eyes (29.4%), respectively, 6 months after mucous membrane and salivary gland transplantation. These results may explain the improvement in best spectacle-corrected visual acuity in 8/19 eyes (42.1%).
It must be emphasised that the sample population in the present study was very homogeneous compared with those in other similar studies. All the patients had a value of zero in an initial Schirmer I test and achieved an improvement in the regularity of the ocular surface and in humidity. It is also important to take into consideration the fact that salivary secretion is denser and the Schirmer I test values may therefore have been underestimated following surgery.
The results of the questionnaire showed an improvement in symptoms, foreign body sensation improving in 53.6%, photophobia in 50.2% and pain in 54.8% of cases. This may be related to the correction of symblepharon and cicatricial entropion, which improved eye movement and decrease foreign body sensation.
As the severity of dry eye is a major prognostic factor for limbal and corneal graft in patients with SJS,17 it is reasonable to believe that improving lubrication may lead to an improvement in the outcome of ocular surface reconstruction using mucous and salivary gland transplantation. Since experience with this technique is still very limited, prospective controlled studies will have to be performed to establish the long-term survival of the transplanted glands and to classify the salivary tear film and evaluate its impact on the ocular surface.
In conclusion, salivary gland and oral mucosa transplantation appears to constitute an effective method of treating severe dry eye secondary to SJS and should be considered as a step prior to limbal and corneal graft in these patients.
Further studies involving larger numbers of patients need to be performed to investigate this subject further; however, this may represent the first step in successfully treating this disease.
References
Footnotes
Competing interests None to declare.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Research Ethics Committee of the Paulista School of Medicine (CEP0427/08).
Provenance and peer review Not commissioned; externally peer reviewed.