Article Text

Abstract
This study describes a novel surgical technique of limbal transplantation, which combines the benefits of existing techniques while avoiding their difficulties. Six patients with unilateral and total limbal stem cell deficiency following ocular surface burns underwent a single-stage procedure. A 2×2 mm strip of donor limbal tissue was obtained from the healthy eye and divided into eight to ten small pieces. After surgical preparation of the recipient ocular surface, these tiny limbal transplants were distributed evenly over an amniotic membrane placed on the cornea. After surgery, a completely epithelialised, avascular and stable corneal surface was seen in all recipient eyes by 6 weeks, and this was maintained at a mean±SD follow-up of 9.2±1.9 months. Visual acuity improved from worse than 20/200 in all recipient eyes before surgery to 20/60 or better in four (66.6%) eyes, while none of the donor eyes developed any complications. This technique requires less donor tissue than previously used for conventional autografting and does not need a specialist laboratory for cell expansion. Although long-term results are awaited, this simple limbal epithelial transplantation promises to be an easy and effective technique for treating unilateral limbal stem cell deficiency following ocular burns.
- Limbal stem cell deficiency
- autologous
- cultivated limbal epithelial transplantation
- ocular surface burns
- iris
- sclera and episclera
- ocular surface
- cornea
- immunology
- imaging
- stem cells
Statistics from Altmetric.com
- Limbal stem cell deficiency
- autologous
- cultivated limbal epithelial transplantation
- ocular surface burns
- iris
- sclera and episclera
- ocular surface
- cornea
- immunology
- imaging
- stem cells
Corneal blindness following ocular burns was once considered incurable as it carried an extremely poor prognosis for corneal transplantation.1 Subsequent discovery of epithelial stem cells at the limbal region of the eye2 ,3 demonstrated that ocular surface disease was a manifestation of limbal dysfunction and could possibly be reversed by limbal stem cell transplantation.4 As proof of this principle, Kenyon and Tseng showed that conjunctival limbal autografting (CLAU) successfully cured limbal stem cell deficiency (LSCD).5 In this technique, two donor lenticules, each consisting of three clock hours of the limbus and adjacent conjunctiva, were obtained from the donor eye and transplanted on to the recipient ocular surface. Rarely, the donor eyes developed LSCD.6–9 To avoid this complication, Pellegrini et al devised a technique called cultivated limbal epithelial transplantation (CLET), wherein less than one clock hour of donor limbus could be expanded ex vivo into a transplantable epithelial sheet.10
Currently, opinion is divided about which of the two existing techniques of limbal transplantation is a better surgical alternative. Both techniques are effective in the long-term restoration of the damaged ocular surface in eyes with LSCD,4–16 and the surgeon's preference is often limited by economic and logistic factors. Proponents of CLAU consider ex vivo cultivation unnecessary and expensive, while proponents of CLET consider autografting technically challenging and risky. In this study, we propose a novel simplified technique of limbal transplantation, which combines the benefits of both existing techniques while avoiding the difficulties of either.
Methods
Patients
Six adult patients with unilateral and total LSCD (defined clinically as 360o absence of the limbal palisades of Vogt, dull and irregular corneal epithelium, superficial corneal vascularisation, persistent epithelial defects or conjunctival overgrowth on the corneal surface) following ocular surface burns and no history of limbal transplantation were included in this study.
Surgical technique
This was a single-stage procedure, performed by a single surgeon (VS). Before the procedure, all patients were administered peribulbar anaesthesia in both eyes. In the donor eye, a 2×2 mm area was marked centred on the superior limbus, the conjunctiva was incised, and a sub-conjunctival dissection was carried out until the limbus was reached (figure 1A,B). A shallow dissection was then carried out 1 mm into the clear cornea, and the limbal tissue was excised (figure 1C) and placed in balanced salt solution. In the recipient eye, a 360o peritomy was performed, and the vascular pannus covering the cornea was removed (figure 1D,E and online supplemental video). After cauterisation of the bleeding points, human amniotic membrane (hAM) graft was placed over the bared ocular surface (figure 1F) and secured with fibrin glue (TISSEEL Kit from Baxter AG, Vienna, Austria). The excess membrane was trimmed and its edges tucked under the surrounding conjunctival margins. The donor tissue was then gently held with Lim's forceps and cut into eight to ten small pieces with either Vannas scissors (figure 1G) or a No 15 surgical blade. The small limbal transplants were placed, epithelial side up, on the hAM and distributed in a circular fashion around the centre of the cornea, avoiding the visual axis (figure 1H). The transplants were also fixed in place with fibrin glue. A soft bandage contact lens was placed on the recipient eye, and one drop of 2.5% povidone-iodine was applied to both eyes, followed by overnight patching.

Clinical photographs showing the surgical technique of limbal biopsy from the donor eye and transplantation of the limbal tissue on the recipient eye. (A) A 2×2 mm area is marked across the superior limbus of the donor eye. (B) A sub-conjunctival dissection is carried out 1 mm into the clear cornea. (C) The limbal tissue is excised. (D, E) A peritomy is performed and the fibrovascular pannus is excised from the recipient ocular surface. (F) A human amniotic membrane graft is placed on the bare ocular surface and secured to it with fibrin glue. (G, H) The donor limbal tissue is cut into eight to ten small pieces and secured to the amniotic membrane overlying the cornea with fibrin glue.
Postoperative care
All patients underwent comprehensive ophthalmic examination of both eyes at all follow-up visits. Patients were seen on days 1, 7, 14, 42 and 90 and at 3-month intervals thereafter. Patients were prescribed ciprofloxacin 0.3% eye drops (Cipla India, Mumbai, India) four times a day for 1 week and prednisolone acetate 1% eye drops (Alcon Laboratories Private Limited, Bangalore, India) six times a day tapered weekly over 6 weeks in both eyes. The bandage contact lens was removed from the recipient eye on day 7, and carboxymethyl cellulose 0.5% eye drops (Allergan India Private Limited, Bangalore, India) were added in the recipient eye.
Results
Demographic and clinical details of the six patients are provided in table 1. A completely epithelialised, avascular and stable corneal surface (figure 2 and online supplemental figure) was achieved by 6 weeks and was maintained in all recipient eyes at a mean±SD follow-up of 9.2±1.9 months. Best corrected visual acuity improved from worse than 20/200 in all recipient eyes before surgery to 20/40 or better in four (66.6%) eyes (table 1). The fibrin glue on the ocular surface had disintegrated by the end of the first postoperative week, and the hAM disintegrated gradually over 6 weeks (figure 2). The transplants remained in place and became progressively transparent over time, almost completely disappearing by 6 months (figure 2 and online supplemental figure). None of the donor eyes developed any complications. The donor site epithelialised in all six eyes within 14 days, and none of the donor eyes showed a decrease in best corrected visual acuity or developed conjunctival overgrowth on the donor site, filamentary keratitis or LSCD.
Preoperative clinical characteristics and postoperative outcomes of patients with unilateral and total limbal stem cell deficiency following ocular surface burns who underwent simple limbal epithelial transplantation (SLET)
{kind=link}
{kind=link}
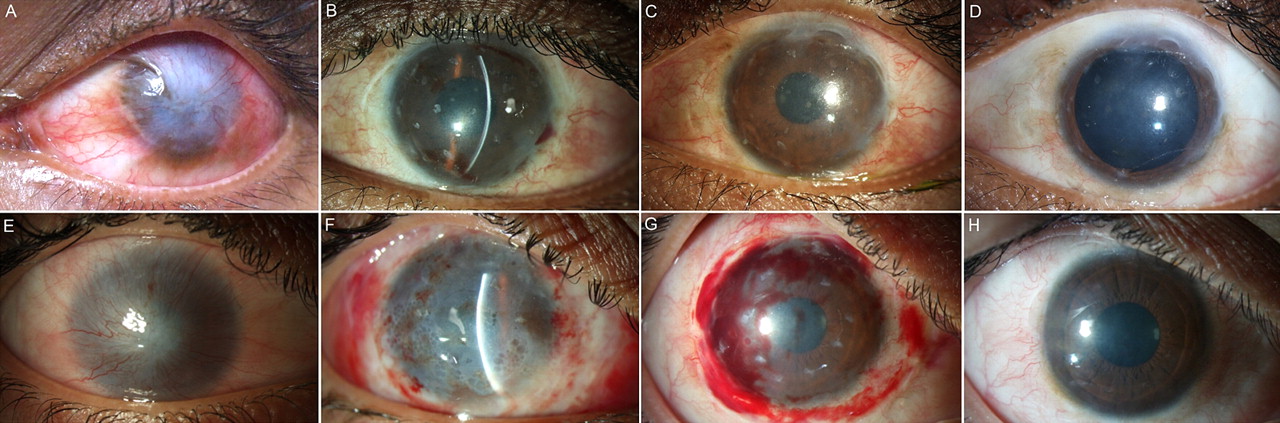
Serial clinical photographs of recipient eyes of two different patients before and after undergoing simple limbal epithelial transplantation (SLET). (A) A 20-year-old college student (case 3) with a history of lime injury to the left eye presented with a conjunctivalised corneal surface, symblepharon in the superior fornix, and visual acuity of counting fingers at 3 m. (B) Six weeks, (C) 3 months and (D) 6 months after SLET, the corneal clarity gradually improved. The visual acuity at 6 months after SLET was 20/20. (E) A 22-year-old car mechanic (case 6) with a history of acid injury to the right eye presented with a completely conjunctivalised cornea and visual acuity of perception of light. (F) One day after surgery the cornea and transplants were covered with fibrin glue. (G) One week after surgery, the corneal clarity markedly improved, revealing the location of the limbal transplants. Haemorrhage under the disintegrating amniotic membrane graft was also seen at this point. (H) Six months after surgery the cornea was clear and avascular, the opacities at the site of the transplants had almost completely disappeared, and the visual acuity had improved to 20/30.
Discussion
The only study directly comparing the two existing techniques of limbal transplantation found that conventional limbal transplantation resulted in delayed corneal epithelialisation, prolonged ocular surface inflammation, and significantly greater scarring than CLET.17 Other proposed advantages of CLET over CLAU include greater safety for the donor eye, as it needs less tissue, and better chances of long-term tissue regeneration, as the number of stem cells transplanted is possibly increased by ex vivo cultivation. However, the cost of establishing and maintaining a stem cell laboratory is prohibitively high. Miri et al estimated in 2010 that, in the UK, a single CLET procedure cost approximately £10 300 (or about €12 000).18 Despite having successfully performed over 500 CLET procedures for the treatment of LSCD since 2001,15 ,19 we felt that, in reality, CLET has become restricted to only a handful of advanced centres worldwide because of these limitations. Similarly, CLAU has also failed to garner universal acceptance because of the perceived risk of donor site complications. Even Tseng and colleagues who pioneered the classical technique4 tried using smaller single two-clock-hour-long lenticules to treat total LSCD, terming the new technique mini-CLAU.20 This study begins to address the challenge of determining how little of the limbus can be clinically effective given a suitable underlying substrate. The results from this study, at least, suggest that less than one clock hour of donor limbal tissue may be sufficient.
Table 2 summarises the comparison of this new technique, which we termed simple limbal epithelial transplantation (SLET), with CLAU and CLET. SLET incorporates the advantages of CLAU by being a single-stage procedure, easily affordable, and not requiring sophisticated laboratory support while retaining the benefit of CLET, using minimal donor tissue. The surgical technique of SLET is relatively straightforward, and our results should be easily replicated by other ocular surface surgeons. Before the study, we were concerned whether the limbal transplants, consisting of epithelium with a thin slice of underlying stroma, would remain opaque over time. Rather surprisingly we found that they almost completely disappeared by 6 months. To explain this, we hypothesise that, as the epithelial cells grow out of the islands of stem cell containing limbal transplants and form a confluent and stratified corneal epithelial layer by 6 weeks, the stromal element undergoes remodelling and is gradually incorporated into the underlying cornea by 6 months. We plan to study this proposed mechanism in greater detail in subsequent cases by performing in vivo confocal microscopy and from the histopathology of corneal buttons obtained from eyes needing keratoplasty surgery. Further refinement of the surgical technique may include avoiding the hAM or by replacing the hAM with biodegradable synthetic polymer scaffolds to support culture of corneal epithelial cells.21
Comparison of the current technique with existing techniques of autologous limbal transplantation for treatment of unilateral limbal stem cell deficiency
As this is a pilot study, the sample size is small and the follow-up is limited. However, as most failures after limbal transplantation usually occur within the first 6 months,13 ,15 the results of this study are truly encouraging. Validation of these initial results in a larger number of patients followed for longer periods of time, possibly on a multicentre basis, is now required. This could significantly simplify the treatment of LSCD, offering a simple approach, easily replicable by practising corneal surgeons, which could benefit many more patients worldwide.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (WMV) - Manuscript file of format wmv
Footnotes
All the authors (VS, SB, SM, DB) contributed equally to the study.
Funding This work was funded by the Department of Biotechnology, New Delhi, India; Champalimaud Foundation, Lisbon; Portugal, and the Hyderabad Eye Research Foundation, Hyderabad, India. None of these had any role in the design, collection, analysis and interpretation of the data.
Competing interests None.
Patient consent Obtained.
Ethics approval The study was approved prospectively by the Institutional Review Board (IRB) and the Institute Committee for Stem Cell Research and Therapy (ICSCRT), L V Prasad Eye Institute, Hyderabad, India. The study followed the tenets of the Declaration of Helsinki, and informed written consent was obtained from all patients enrolled in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors are committed to make materials, data and associated protocols promptly available to others without preconditions.
Linked Articles
- At a glance