Article Text

Abstract
The presented Z-suture is a simple, rapid and safe knotless technique that facilitates transscleral suture fixation of various intraocular implants in the ciliary sulcus, such as sutured intraocular lenses, artificial iris prostheses and iris diaphragms. As the knotless approach reliably avoids suture erosion, external fixation can be performed without any protecting scleral flaps or lamellar grooves. The needle is simply passed through the sulcus and the emerging polypropylene suture is secured in the sclera using a zigzag-shaped intrascleral suture (Z-suture). Each pass starts directly adjacent to the exiting site. Five passes are sufficient to reliably fix the suture so that it resists even maximum tractive forces. Once this procedure is done, the suture can be cut without any knot. By avoiding suture knots, and hence the need for intrascleral flaps, this knotless approach may help to reduce suture-related complications such as scleral atrophy, suture erosion and infections.
Statistics from Altmetric.com
Transscleral suturing is a standard technique to fix various intraocular implants in the sulcus. Since the early 1990s, the ab-externo technique of Lewis1 and the refined ab-interno technique of Smiddy et al2 are the basis for multiple variations in transscleral suturing. However, all techniques need a reliable external fixation in the sclera without direct knot exposure. Leaving a suture knot directly under the conjunctiva often leads to suture erosion and consecutively to an elevated risk for endophthalmitis (figure 1). Therefore, it is generally recommended that the knot be protected, for example, by burrowing it under a scleral flap.3 However, late atrophy of the scleral flap is often observed in the long-term and causes late suture erosion through the conjunctiva.4 Alternative techniques by creating a scleral groove or a scleral pocket are less invasive, but share the same limitations.5–8

Representative slit-lamp photography after transscleral suture fixation of posterior chamber intraocular lens using a standard scleral flap technique (A) or the knotless Z-suture technique (B). A scleral flap does not reliably prevent suture erosion. Eight months after surgery the knot erodes through the atrophic scleral flap and the conjunctiva demonstrating the risk of late endophthalmitis (A). Fourteen months after using Z-suture technique the fixation is firm and shows no signs of scleral atrophy, suture erosion or chronic inflammation. The intrascleral polypropylene suture is barely visible under a quiescent conjunctiva (B).
We present a completely knotless technique (Z-suture) that is fast, easy to perform and suitable for transscleral suture fixation of various intraocular implants regardless of the type of implant or the suturing technique used.
Surgical technique
Various implants were placed in the sulcus and sutured transsclerally. Foldable intraocular lenses (IOLs) (AF-1; Hoya, Frankfurt, Germany) were fixed using a modified ab-externo technique with a double-armed 10-0 polypropylene suture as described previously.9 Other implants, such as the artificial iris prosthesis (HumanOptics, Mannheim, Germany), open iris diaphragm (PD1; Acri.Tec, Glienicke b., Berlin, Germany) and closed iris diaphragm (ID1; Acri.Tec), were fixed using the ab-interno technique with three single-armed looped 10-0 polypropylene sutures with a slip knot.10
All manoeuvres finally resulted in two (IOL) or three (artificial iris prosthesis and iris diaphragms) sutures emerging from the outer sclera (figure 2A).

Z-suture technique for external fixation of a transscleral polypropylene suture. After emerging from the sclera at about 1.3 mm distance from the limbus the needle is reintroduced for an intrascleral suture pass directly adjacent to the exiting site (A). To assure an acute angle and hence a firm adhesion the suture is introduced again close to the outlet and passed in the opposite direction (B). The manoeuvre is repeated five times resulting in a zigzag-shaped pattern with five suture passes (C). Finally, the suture is simply cut at the level of the sclera and left without any knot (D).
In all cases, external suturing was performed with a new knotless Z-suture technique: The external suturing was started with an intrascleral pass adjacent to the transscleral penetration site parallel to the limbus. This intrascleral pass was repeated in the respective opposite direction (figure 2B) finally resulting in a zigzag pattern with five indentations (figure 2C). Each pass (3–4 mm) should start directly beneath the exiting site. With each pass the resistance force increased and, once the five zigzag passes were done, the suture was cut without any knot (figure 2D).
In order to evaluate the number of passes necessary for secure fixation of the suture within the sclera, an ex vivo study was carried out using porcine eyes. As was done in humans, a transscleral ab-interno pass with a consecutive Z-suture using 10-0 polypropylene was performed. After each pass the tractive forces necessary to mobilize the suture were measured with a Newton dynamometer (#314151; Leybold, Hürth, Germany).
Results
The laboratory evaluation showed that the resistance to tractive forces increases with each pass of the Z-suture. Five suture passes were enough to resist a maximal tractive force of 0.41 (median 0.38) N. At this point the tractive forces exceeded the tensile strength and the suture ruptured. Hence, five passes reliably prevented mobilisation of the suture (table 1).
Tractional forces (N) necessary to pull back a Z-suture measured after each intrascleral pass
This Z-suture technique with five passes has been used in 67 patients including 45 cases of sutured IOLs, 18 cases of iris prostheses and four cases of iris diaphragms. No complications were observed except a transient mild ciliary haemorrhage in three eyes. In all patients, the implant stayed firmly fixed within the sulcus even after a mean follow-up time of 22.4 (range 6.1–38.1) months. At the final examination, the sutures were barely visible. No evidence of suture erosion, suture loosening, scleral atrophy or chronic inflammation was observed in any of these patients (figure 2). In all cases, the implants were smoothly positioned in the ciliary sulcus and showed a stable and centred position without any tilt or torque (figure 3).
{kind=link}
{kind=link}
{kind=link}
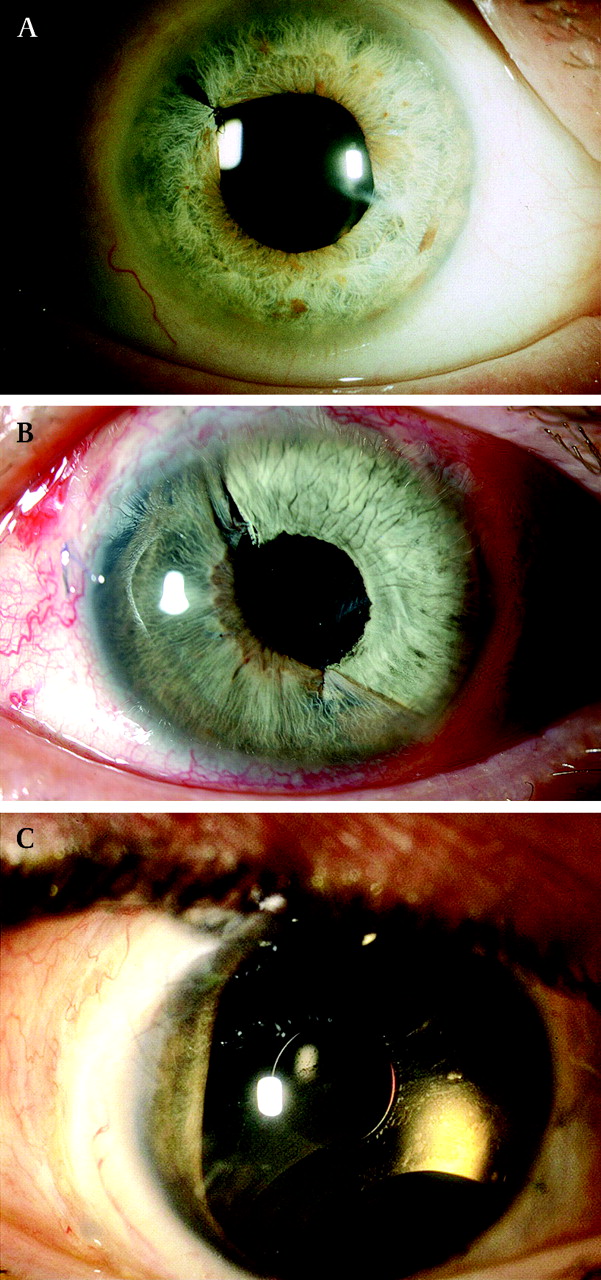
Representative slit-lamp photography after transscleral suture fixation of a posterior chamber intraocular lens (IOL) (A), partial iris prosthesis (B) or open iris diaphragm (C) using knotless Z-suture technique. (A) Four months after iris reconstruction and transscleral sulcus-suturing of a foldable IOL the implant is well-centred and the intrascleral zigzag suture invisible. (B) Two weeks after partial iris replacement over 6 clock hours the artificial iris prosthesis is firmly fixed by three transscleral Z-sutures at the 12, 4 and 8 o'clock positions. Besides the transscleral fixation two additional side-to-side sutures are used. (C) Three Z-sutures are also used for transscleral fixation of an open iris diaphragm that has been implanted in combination with revisional retinal surgery and silicone oil tamponade in relapsing proliferative vitreoretinopathy. Six months after surgery the implant is well-centred and the anterior chamber free of silicone oil. Note the temporal natural iris remnants, the lower artificial ando-iridectomy and the artificial pupil safely retaining the silicone oil bubble.
Discussion
The Z-suture offers a number of advantages over previous approaches to transscleral suturing. First, fixing the external suture to the sclera is rapid and easy to perform with minimal opening of the conjunctiva (3–4 mm). The second advantage is its universal applicability: the Z-suture can be used regardless of the type of implant (sutured IOL, closed and open iris diaphragms, artificial iris prostheses), the haptic design (with or without eyelets), the suturing technique (ab-externo or ab-interno), the fixation type (two-, three- or four-point fixation), the type of needle (straight or curved), the suture size (polypropylene 9.0 or 10.0) and the suture design (single- or double-armed). In all cases, the transscleral suture emerging from the sclera can be rapidly fixed within the sclera and then simply cut without any knot left behind.
More important, this technique is safe and reliable in firmly fixing the suture within the sclera. Five zigzag passes are sufficient to resist any traction from the implant as shown in the ex vivo series. Although the results from porcine eyes cannot be directly transferred to human conditions, this strong fixation has been confirmed clinically in all cases. No loosening of the suture or dislocation of the implant has been observed in the long term.
The main advantage is the knotless approach. By avoiding suture knots it may help to reduce complications such as scleral atrophy and suture erosion. Late suture erosion with knot exposure is a major problem in transscleral IOL suturing that may result in an increased incidence of endophthalmitis.4 Hence, burying the suture knots under a scleral flap3 or in a scleral groove5 is generally recommended. However, Solomon et al found a 73% rate of suture erosion even through scleral flaps in the long-term, suggesting that this approach delays but does not prevent this complication.4 Other techniques using corneal tissue or scleral patch graft often maintain a better protection of the knot, but are time-consuming and unreasonably invasive.11
In contrast, the Z-suture technique reliably secures the external suture in the sclera without any knot and thereby obviates the need for scleral flaps or grooves. No scleral atrophy or chronic inflammation was observed in the long term. The intrascleral Z-suture seems to be well-tolerated and is less invasive than scleral flaps or other lamellar techniques.
This technique neither influences general complications of transscleral suturing like cystoid macular oedema, glaucoma, haemorrhage or late suture breakage nor contributes to the unsettled controversy about the value of suture fixation compared to alternative techniques.12 However, if sulcus-suturing of ocular implants is pursued, the Z-suture technique considerably facilitates the procedure and might avoid knot-related complications. Long-term results have to be awaited until the value of this technique can be finally judged.
In summary, the Z-suture is a simple and rapid technique for transscleral fixation of various sulcus implants that is applicable for a broad spectrum of surgical situations. It needs only little conjunctival opening, obviates the need for scleral flaps or grooves, and avoids suture-related complications due to the knotless approach.
Footnotes
Presented at the 24th Congress of the European Society of Cataract and Refractive Surgery (ESCRS), London, UK, 11 September 2006 and at the Annual Congress of the American Society of Cataract and Refractive Surgery (ASCRS), San Diego, California, USA, 29 April 2007.
Competing interests None declared.
Ethics approval Obtained.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.