Article Text

Abstract
Aims/Background Rhegmatogenous retinal detachment (RRD) is a potentially blinding condition. Obtaining an accurate estimate of RRD incidence in the population is essential in understanding the healthcare burden related to this disorder.
Methods A systematic review of all population-based epidemiology studies of RRD published between January 1970 and January 2009 from Medline database searches was performed.
Results RRD incidence demonstrates significant geographical variation and its incidence has been reported to be between 6.3 and 17.9 per 100 000 population. For studies with a sample size >300 the median annual incidence per 100 000 population was 10.5 (IQR 8.1–13.2) and the mean proportion of bilateral RRD was 7.26%. Overall, the mean prevalence of lattice degeneration was 45.7±20.3% and myopia was 47.28±12.59%.
Conclusions Estimates of RRD incidence have varied threefold, but inclusion criteria and other design features have differed across studies making direct comparisons difficult. The overall incidence of RRD is not yet well established: more incidence studies of adequate methodology are needed to explore temporal changes in incidence. RRD incidence varies with ethnicity and is strongly associated with increasing age, myopia and certain vitreo-retinal degenerations. Due to changes in cataract surgery trends, the proportion of pseudophakic RRD presenting to specialised centres appears to be increasing.
- Epidemiology
- retinal detachment
- incidence
- retina
- public health
- epidemiology
Statistics from Altmetric.com
Introduction
Rhegmatogenous retinal detachment (RRD) is caused by separation of the neurosensory retina from the underlying retinal pigment epithelium. Despite treatment advances, functional results remain poor, with only 42% achieving 20/40 vision and only 28% if the macula is involved.1
The features distinguishing population-based epidemiological studies are careful delineation of the population from which cases derive and the effort to ascertain every eligible case.2 Since 1970, several studies have investigated the epidemiology, characteristics and risk factors associated with RRD. These studies differ in methodology and case definition, making comparison of data over time and between locations problematic. In this article we review the epidemiology of RRD and associated clinical features in population-based studies.
Methods
We conducted a Medline database search from January 1970 to January 2009 using the search terms ‘incidence’, ‘population’, ‘epidemiology’ and ‘rhegmatogenous’, ‘retinal detachment’ in different combinations. The search engine Google Scholar was also used to identify relevant articles published in books, journals and websites. Further articles were identified by tracking the references of relevant publications. Studies were eligible if they were observational and designed to estimate RRD incidence. Paediatric studies were excluded. Articles published in other languages were included and if needed translated. Articles published as letters or abstracts were excluded (see figure 1).

Flowchart of literature search on population based studies of rhegmatogenous retinal detachment (RRD).
The titles and abstracts of all articles found were reviewed. We developed a checklist (Appendix 1), based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations,3 and each article was given a methodology score out of 20. A consensus on inclusion criteria was agreed by the investigators and studies meeting the following criteria were included:
Recruitment period of at least 1 year
Clear case inclusion criteria
Clear statistical data and an effort to report 95% CIs for incidence rate
Reporting of age-specific incidence rates
If necessary, the 95% CIs of incidence rates were calculated from demographic data assuming Poisson distribution. The age- and sex-specific incidence and geographical distribution of incidence estimates were examined.
Results
Selected studies
A total of 14 studies were included. Eight were retrospective assessments from hospital records (five) or International Classification of Disease (ICD)-coded data (three). Four studies established prospective recruitment from treatment centres. One was a questionnaire survey and another was a local population survey. Only two studies achieved the maximum methodology score. All studies principally report the incidence of RRD cases attending hospital services for diagnosis or treatment.
Incidence and geographical variation
The first comprehensive population-based estimates of RRD were conducted in Iowa and Minnesota, USA.2 4 The former was based on a hospital register and a questionnaire to all 24 ophthalmologists in Iowa City and surrounding regions. The latter study involved a database search for all patients presenting to hospitals in Rochester, Minnesota, between 1970 and 1978. Despite a large difference in case size and methodology, both reported an overall annual incidence of approximately 12 per 100 000.
At a similar time in Europe, two studies reported differing annual incidences of 6.9 and 10.6 per 100 000 in Finland and Sweden.5 6 The Finnish study was an operative series from Helsinki University Hospital between 1978 and 1981. The Swedish study included all patients admitted with RRD to a medical centre over 10 years (1971–1981). From the data, it is unclear why the reported incidences vary by 40%. Excluding aphakia, the reported incidence of RRD varied between 5.4 and 8.5 per 100 000 of population.
Epidemiological analyses of RRD have also used large centralised computer databases. The Rochester Epidemiology Project identified Olmstead county residents admitted with RRD over 20 years (1976–1995), giving the highest reported overall incidence of 17.9 per 100 000.7 One Swedish study established a complex, computer-based national register and analysed more than 1000 patients with RRD, reporting an overall incidence of 14 per 100 000.8 The first Asian study reviewed 1126 Singapore residents having operative repair of RRD over 4 years, reporting a constant annual incidence of 10.5 per 100 000.9 Overall, centralised databases may provide higher case capture; however, previous reports have demonstrated a large (∼twofold) variation.
Two Chinese studies10 11 have estimated differing annual incidences between 7.98 and 14.4 per 100 000, with the proportion of myopia being high (66–68%) in both studies. In Beijing, patients were recruited bimonthly from 35 centres. The Shanghai study included hospital cases and outpatients from the local health network, showing an annual increase in incidence over the 4-year study period from 11.3 to 17.9 per 100 000 of population. Similarly, a 5-year review of UK patients undergoing surgical repair showed the incidence of two regions only 8 miles (13 km) apart varied between 11.3 per 100 000 (Wolverhampton) and 6.3 per 100 000 (Walsall).12
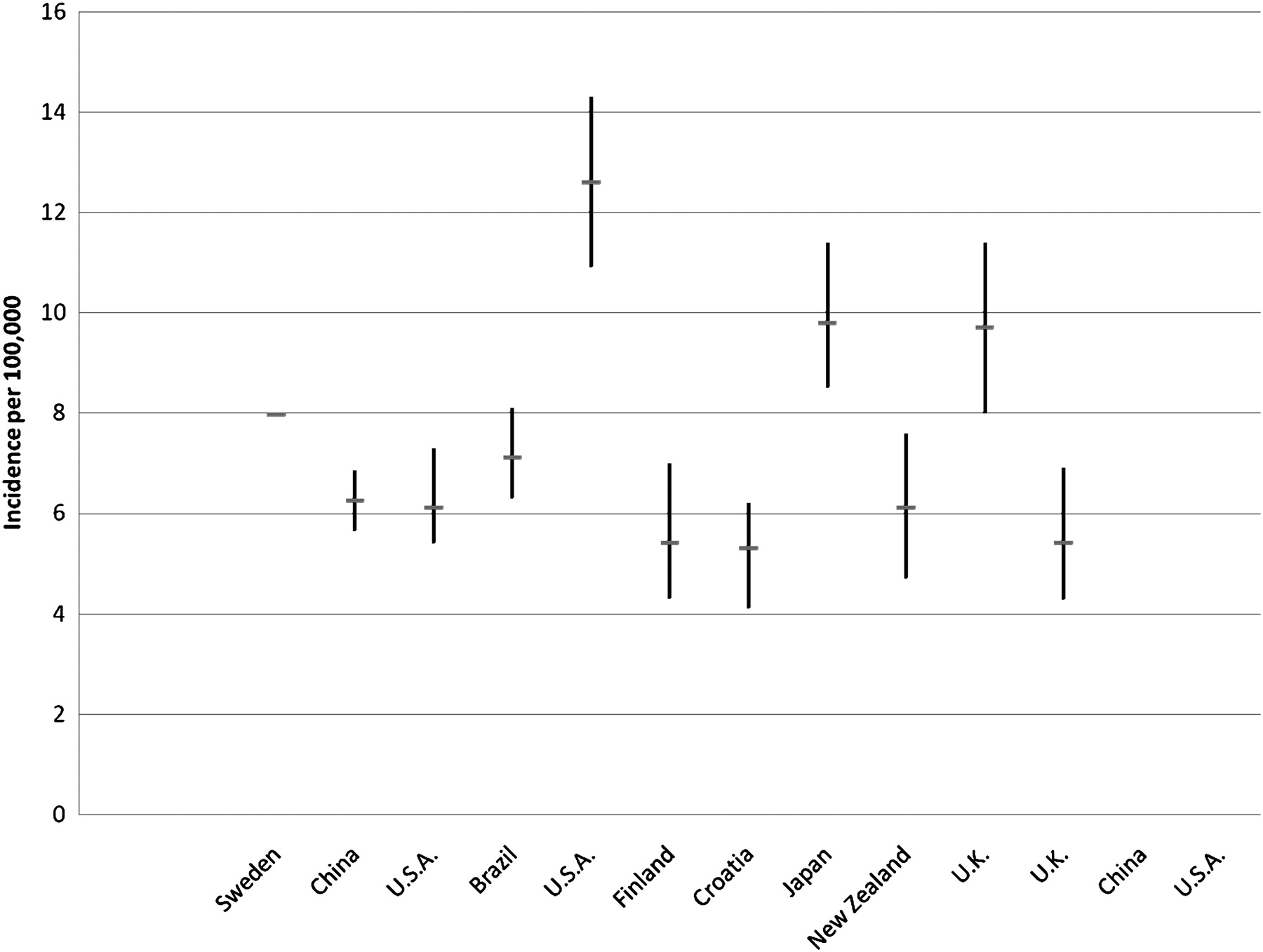
The reported incidence, study design, case inclusion and relative sample size of population based epidemiological analyses of RRD is summarised in table 1 and figure 2, demonstrating the wide range reported. Of the prospectively conducted studies, only two have attempted to include outpatient cases.10 11 Several studies have a small sample size introducing a potential for sampling error. Examining the eight studies with a sample size >300 cases reveals a median annual incidence rate of 10.5 (IQR 8.1–13.2) per 100 000 of population. However, the inclusion of trauma and re-operations differs between all reports, with seven of 14 studies not specifying if re-operations were included. Excluding all other cases and examining non-traumatic phakic cases only reveals a similar variation between 5.3 and 12.6 cases per 100 000 of population (see figure 3).
Reported incidence of rhegmatogenous retinal detachment (RRD) (per 100000 of population), clinical characteristics and inclusion criteria as reported in previous population-based epidemiology studies ordered by sample size
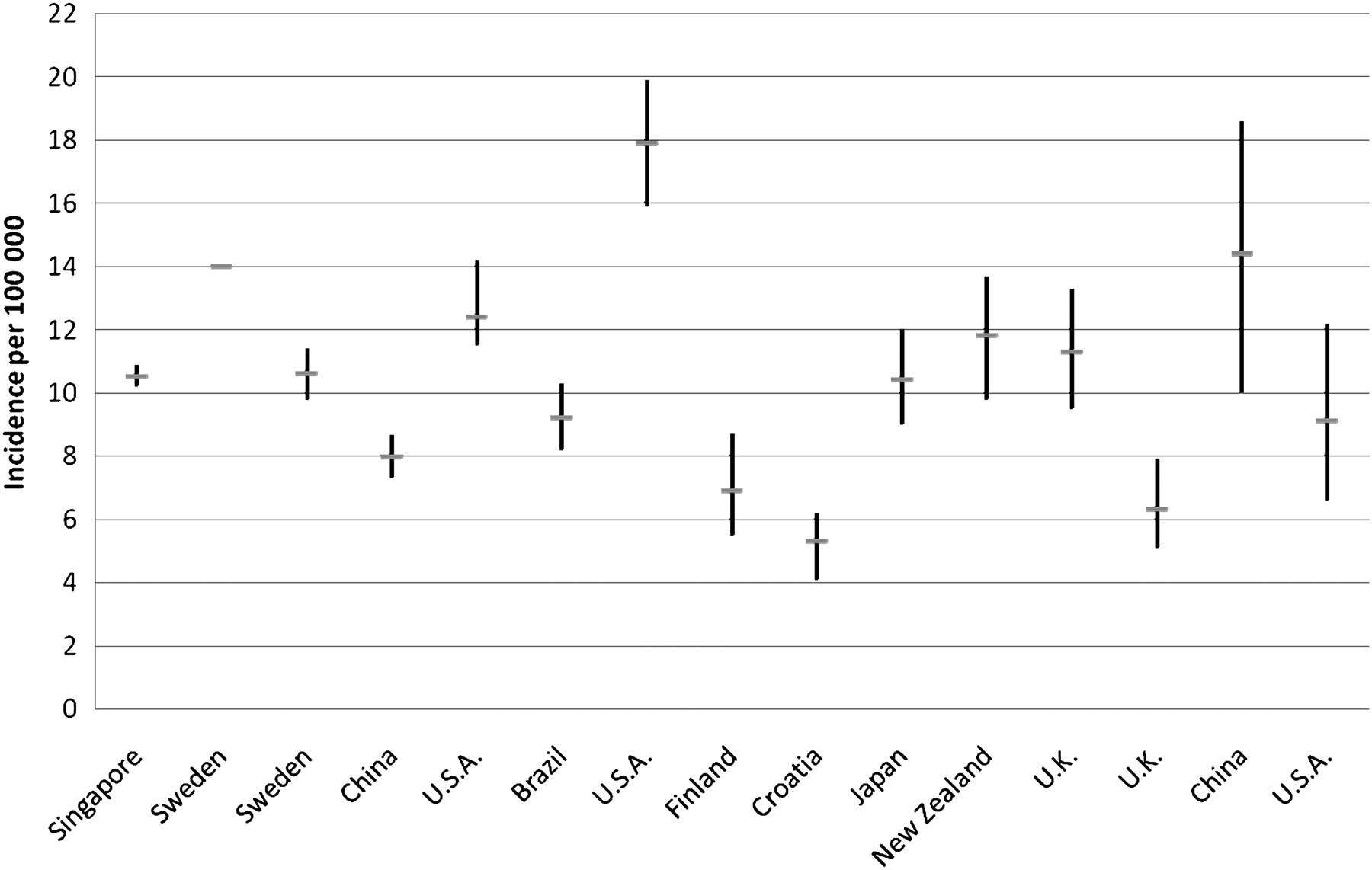
Overall reported total incidence rates (per 100 000 of population) and associated CIs of rhegmatogenous retinal detachment (RRD) in previous population-based epidemiology studies ordered by sample size.
{kind=link}
{kind=link}
{kind=link}
Overall reported incidence rates and associated CIs of non-traumatic phakic rhegmatogenous retinal detachment (RRD) in previous population-based studies ordered by sample size.
Age distribution
RRD develops from retinal breaks occurring at physiological or pathological sites of firm vitreo-retinal adhesion during posterior vitreous detachment (PVD) or from atrophic holes.17 The prevalence of PVD increases with age, occurring in 11% of 60–69-year-olds, 46% of 80–89-year-olds and occurring earlier in myopes.18
The largest annual incidence rate of RRD is seen in the elderly, with studies supporting a bimodal distribution and a secondary peak in younger ages (20–30 years) attributed to highly myopic patients.4 9 10 15 16 The highest incidence rate of RRD was found in the 60–69-year-old age group with rates varying between 19 and 27 per 100 000.4 10–12 15 However, unexplained incidence rates as high as 40 and 70 per 100 000 have been reported7 13 16 (see Supplemental figure 1). The strongest association was noted between advancing age and non-traumatic phakic RRD.4 10 12 15 19 After 60 years of age the risk of developing RRD can be 17–20 times greater than in a cohort under 30 years of age.6 The incidence rate of RRD in under 20-year-olds was the lowest noted: <3 per 100 000, similar to previous paediatric series.4 9 10 13 16 20
Despite a similar distribution of >60-year-olds in study populations, the incidence of RRD in this age group has also shown variation (see table 2) In Beijing and Finland 14% and 15.2% of the population were >60 years old and the incidence rates were comparable at 7.98 and 6.9 per 100 000.5 10 However, in Singapore and Brazil, the proportion of the population >60 years old was <10%, but the reported incidences in this group differed more than twofold, suggesting other influencing factors.9 13
Age specific incidence of rhegmatogenous retinal detachment (RRD) in >60 year-olds as reported in previous epidemiology studies (ordered by sample size) and the proportion of study population >60 years old
Sex
While some reports indicate a sex distribution corresponding with that of the general population,4 5 most indicate a preponderance of men,12–14 16 21(male to female ratio 1.3:1 to 2.3:1) and a minority find that women predominate in the phakic non-traumatic group (male to female ratio 1:1.16 to 1:1.4) 6 15 (see Supplemental figure 2). A large Singapore study found that men are twice as likely to require surgery. This may be related to an inherent sex-related risk, though an increased rate of ocular trauma was contributory.9 Furthermore, in myopic populations men tend to predominate, although with age, this sex-based refractive difference may be less significant.22–28 Nonetheless, the higher proportion of myopia in young men may partly explain the imbalanced sex distribution in some studies.
Seasonality
Seasonal variation in RRD incidence with a summer peak and winter trough has been reported.5 29–31 The effect of light and temperature on the vitreous has been implicated.29 In some studies, no seasonal variation was found,6 11 32 and others note a winter peak and a summer trough.33
Ethnicity
In the few studies performed, ethnic variation significantly affects the incidence of RRD. The reason for this is unknown. In Singapore, RRD incidence in Chinese is three times higher than in Indians (11.6 per 100 000 and 3.9 per 100 000)9 despite minimal variability of risk factors (myopia, lattice degeneration, previous intra-ocular surgery and trauma). A UK study noted a threefold lower incidence in Asians compared with Caucasians.12 Numerous reports suggest the incidence of RRD in Blacks is lower than in Caucasians.34–40 However, to date there have been no population-based studies of RRD incidence in developing countries.40 Despite reported variations, post mortem studies have not demonstrated racial variation in the prevalence of predisposing ocular factors to RRD.41
Trauma
Traumatic RRD shows a male predominance affecting younger age groups. Series in Finland, Sweden, Beijing and Iowa found between 6.3% and 12.2% of RRDs were traumatic with the majority being young men.4–6 10 In New Zealand 16.4% of RRDs were associated with ocular trauma with nearly 90% <50 years old.16 In the majority of studies, the incidence range of traumatic RRD has been consistently low (0.6–2 per 100 000 – see table 1).
Bilateral RRD
Bilateral RRD affects 3–33% depending on case inclusion and study duration.42 Earlier large clinical studies noted a high rate (473/2016 and 1642/5270) of bilateral RRD including re-detachments over 10 years.19 43 Over 1 year, rates of bilateral RRD vary between 3.5% and 5.82%,4 10 15 16 increasing to 9–10% over a 4-year period.5 11 44 In Sweden over 10 years and Minnesota over 20 years, 11.2% (34/538) and 6% (18/293) of subjects had bilateral RRD.6 7 In all series, RRD has affected a proportion of both eyes indicating over time fellow eye involvement is an important consideration.
Peripheral retinal degeneration and RRD
Areas of abnormal vitreo-retinal adhesion (oral bays, meridional complexes, retinal tufts) can predispose to retinal breaks during PVD. However, efforts at characterising these lesions indicate they are uncommonly associated with RRD and carry a low risk of progression (<2%).17 Similarly, most peripheral retinal degenerations are poorly characterised in epidemiology studies. The association with lattice degeneration is better known. Lattice degeneration is a vitreo-retinal degeneration of unknown pathogenesis. Normal worldwide prevalence is between 6% and 9.5%.45–47 The prevalence increases with myopia from 4.3% in emmetropia to 14% in myopia of greater than −3 D.48 Although Byer suggests the incidence of RRD from retinal breaks associated with lattice degeneration is low (0.3–0.5%), lattice degeneration may be associated with up to 60% of RRD.49 RRD patients with lattice are younger and more myopic than those without. Of Swedish patients with RRD and lattice (29.7%), one-quarter had a refractive error of greater than −5 D compared with 15.7% in eyes without lattice.6 A clinical report from India showed that 26.8% of eyes had lattice and a similar proportion were also myopic (31.3%).50 A higher proportion of lattice degeneration was found in Japanese studies (60–65%), with refractive error in these cases showing a myopic deviation away from the mean of >2 D.15 51 Depending on population characteristics, lattice degeneration appears to be an important factor associated with RRD in myopic eyes.
Clinical characteristics of RRD
Tractional, PVD-induced retinal tears or atrophic retinal holes can cause RRD.19 Clinical studies observe a higher frequency of tractional tears in phakic RRD: India (186/395 vs 116/395)50, America (880/1353 vs 578/1353)19, Helsinki (217/352 vs 61/352.44 Round hole detachments occurred mainly in myopic eyes with lattice. Tears were more frequent in non-myopic phakic patients >40 years old. In two US studies, atrophic holes accounted for 3% and 14% of detachments.52 53 In Japan, of patients with lattice degeneration, 40% of RRDs were caused by tractional tears and 20% by atrophic holes.15 Giant retinal tears and retinal dialysis are uncommon, accounting for 0.6–5.3% of phakic RRD.15 19 50 Macular hole RRD is uncommon in European44 and American54 series (0.5% and 1.7%), but accounts for 8.9% and 21.1% of RRDs in more myopic series.15 55
Macular status
Macular attachment at presentation is an important prognostic indicator of visual outcome. Western studies support a macula off detachment rate of 40–60%,7 44 compared with a higher rate of 86.8% in developing countries.50 Schepens et al noted a macula off presentation in 65.1% of phakic RRDs in 1973 compared with a largely unchanged rate of 69% in the UK in 1997.19 56
Refraction and RRD
Myopia and especially high myopia are major risk factors for RRD.43 57 58 Independent of age, an eye with a spherical equivalent refractive error of −1 to −3 D has a fourfold increased risk of RRD compared with an emmetropic eye, increasing to tenfold with a refractive error of greater than −3 D.59 60 Myopia predisposes to RRD through increased vitreous liquefaction, earlier PVD and higher incidence of vitreo-retinal degeneration.17 Myopic patients are more likely to have RRD at a younger age and bilateral RRD.10 48 60–62
In Scandanavia, myopic detachments (greater than −2 D) composed 40% and 50.3% of all phakic detachments in young age groups. This was four to six times higher than myopia prevalence in contemporary estimates.5 6 In Croatia 46.9% of all phakic detachments were myopic (greater than −0.75 D) compared with 22.8% of the general population.14 A higher rate of low myopia (66–68%) was seen in Beijing and Shanghai.10 11 In New Zealand, myopia of greater than −6 D increased the risk of early RRD by 90%.16 The strong association between myopia and RRD in young age groups is evident. However, ethnic differences are likely to underlie the reported variation, as myopia prevalence in Asian countries is known to be 1.5 to twofold higher than Caucasian populations of similar age.15 63 64
Cataract extraction and pseudophakia
The risk of RRD after cataract extraction varies with the surgical method employed. This is due to a higher rate of PVD after cataract extraction and a lower hyaluronic acid concentration causing vitreous collapse.17 65 The cumulated 6-year-risk of RRD after cataract surgery is increased by a factor of between six and eight, increasing linearly for 20 years.66–69 In the 1950s clinical series found a quarter of all RRDs were aphakic.19 Over time the reported proportion of aphakia has declined (42.7% in 1976; 18.6% in 1981; 4.7% in 1990; <10% in 2000),4 6 10 15 reflecting cataract surgery trends.
Studies from Minnesota revealed 26.6% and 19% of RRD cases had previous cataract surgery.2 7 Between 1971 and 1981, 18.6% of RRD cases had prior cataract extraction in Sweden. Twenty years later, the Swedish RRD register reported that 30.8% of more than 1000 detached eyes had prior cataract surgery.6 8 By contrast, the combined proportion of aphakia and pseudophakia in China has been reported as only 10%,10 and further UK and South American studies have supported this observation.12 13 More recently, a New Zealand study reported a high rate (33%)of pseudophakia.16 As a consequence of changing trends in cataract surgery and poorly reported rates, an accurate comparison of the incidence of pseudophakic RRD in previous studies is difficult. However, of the available data, reports in the last decade indicate a slightly higher incidence of pseudophakic RRD than the preceding decade (see table 1).
Increased rate of cataract surgery
Higher life expectancy and advances in cataract surgery has seen the proportion of pseudophakic individuals in developed countries rise. The Rochester Epidemiology Project reported a linear rise in cataract surgery rates between 1980 and 1994.70 The estimated prevalence of unilateral pseudophakia in North Carolina increased from 7.6% to 9.8% between 1998 and 2002, with the prevalence of bilateral pseudophakia more than doubling.71 Between 1986 and 1990 the number of cataract operations in Sweden rose from 227 to 328 per 100 000 of population and in the UK, the rate of cataract surgery increased 3.7-fold between 1989 and 2004.72 73 The estimated prevalence of pseudophakia or aphakia in the US is 5.1% in those >40 years old (6.1 million), and this is expected to rise (to 9.5 million) by 2020.74
The overall incidence of RRD has not shown this linear rise (figure 2). However, the proportion of pseudophakia in RRD series appears to be increasing. A vitreo-retinal centre in London analysed cases of RRD in 1980 and again in 1999 finding that pseudophakia rose from 0.8% to 24%. Other UK reports support this large increase.75 76 In a series of 4203 primary RRD cases in France the proportion of pseudophakia rose from 13% to 33% between 1989 and 2000.77 Strikingly, a comparison between the proportion of pseudophakic RRD in Minnesota between 1970–8 and 1976–95 showed no significant difference, despite a fourfold rise in the rate of cataract extraction between 1980 and 1994 in the same region.2 7 70
Variation, bias and the need for further research
The overall variation reported in these studies is large and likely to be due to differences in study design and population examined. However, this variation persists when examining non-traumatic phakic cases only and in reports from regions of comparable myopia prevalence and elderly population distribution, suggesting a potential (undiscovered) underlying influence. The methodology employed in eight of 14 studies described were retrospective reviews, which may provide an accurate incidence estimate of the population studied, but are often limited by the precision of diagnostic and operational coding. While studies examined define RRD clinically, their inclusion with regard to re-operations, trauma, non-operated cases and outpatient cases differ. No studies have attempted to apply capture–recapture methodology to estimate under-ascertainment rates or have estimated the proportion of non-operated or outpatient cases. Similarly, few recent estimates of RRD incidence have used large samples sizes; most reporting <500 cases. A detailed national or international register may allow for longitudinal studies and a more inclusive estimate of RRD incidence and its variation over time. As outpatient procedures and day-case surgery become increasingly widespread, reliance on inpatient operative records to estimate RRD incidence are likely to become insufficient. A clear consensus on case definition would permit better comparison of data between studies.
Conclusion
The incidence of RRD varies with population studied and is limited by study design and inclusion criteria. The largest annual incidence of RRD is in the 60–70-year group with large studies supporting a secondary peak in young myopes and a higher overall incidence in men. Most series support a bilateral rate of RRD of between 5% and 15%. The higher prevalence of myopia in Asian countries does not appear to reflect a higher RRD incidence in these countries. Ethnic variation or as yet undiscovered genetic factors may underlie this observation. Depending on the characteristics of the study population, myopia and lattice degeneration may be associated with RRD in up to 66% of cases. The overall incidence of RRD worldwide is inconsistent, and from the limited data available, it does not appear to be rising despite a linear increase in cataract surgery rates in developed countries.
References
Supplementary materials
Web Only Data bjo.2009.157727
Files in this Data Supplement:
Footnotes
Funding Royal College of Surgeons Edinburgh.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.