Article Text

Abstract
Aims: The aim of this study was to report the development or progression of tractional retinal detachment (TRD) after the injection of intravitreal bevacizumab (Avastin) used as an adjuvant to vitrectomy for the management of severe proliferative diabetic retinopathy (PDR).
Methods: The clinical charts of patients who experienced the development or progression of TRD after an intravitreal injection of 1.25 mg bevacizumab before vitrectomy for the management of PDR were reviewed.
Results: Eleven eyes (patients) out of 211 intravitreal injections (5.2%) that developed or had progression of TRD were identified. All eyes had PDR refractory to panretinal photocoagulation (PRP). Nine patients had type 1 diabetes mellitus (DM), and two patients had type 2 DM. Patients had a mean age of 39.5 years (range 22–62 years). In the current study, all patients used insulin administration and had poor glycaemic control (mean HbA1c 10.6%). Time from injection to TRD was a mean of 13 days (range 3–31 days). Mean best correct visual acuity (BCVA) at TRD development or progression was logarithm of the minimal angle of resolution (LogMAR) 2.2 (range 1.0–2.6) (mean Snellen equivalent hand motions; range 20/200 to light perception), a statistically significant worsening compared with baseline BCVA (p<0.0001). Eight eyes underwent vitrectomy and three patients refused or were unable to undergo surgery. The final mean BCVA after surgery was LogMAR 0.9 (range 0.2–2.0) (mean Snellen equivalent 20/160; range 20/32 to counting fingers), a statistically significant improvement compared with TRD BCVA (p = 0.002).
Conclusions: TRD may occur or progress shortly following administration of intravitreal bevacizumab in patients with severe PDR.
Statistics from Altmetric.com
Proliferative diabetic retinopathy (PDR) is a major cause of visual loss in patients with diabetes mellitus.1–3 Studies have demonstrated not only a correlation of vascular endothelial growth factor (VEGF) levels with the severity of PDR, but also a reduction in levels after successful laser treatment of PDR.4 5 Thus a rational approach to treating neovascularisation in these patients would include the use of anti-VEGF agents.6–8
Bevacizumab (Avastin; Genentech Inc., San Francisco, CA, USA) is a full length humanised antibody that binds to all subtypes of VEGF and has been approved by the US Food and Drug Administration for the treatment of metastatic colorectal cancer.9 Recent reports have suggested that bevacizumab may be useful in the treatment of choroidal neovascularisation, diabetic macular oedema, PDR and macular oedema associated with retinal venous occlusive disease.7 10–15
Panretinal photocoagulation (PRP) is currently the mainstay of therapy for PDR, significantly reducing the risk of blindness in these patients.16 17 However, there are instances when it is difficult or impossible to administer PRP because of media opacity, such as vitreous haemorrhage. There are also cases that do not respond with complete regression even after extensive PRP: in such cases intravitreal bevacizumab could be considered as an alternative salvage therapy.
Recently, it has been reported that intravitreal injection of bevacizumab may be also useful for early vitreous haemorrhage in PDR in order to decrease the risk of new haemorrhages while clearing occurs and to minimise the indications of vitrectomy.18 In addition, Chen and Park19 and Avery et al20 have suggested that preoperative intravitreal bevacizumab might be helpful to facilitate vitrectomy in severe PDR cases. In such cases, the preoperative use of bevacizumab might reduce the risk of intraoperative bleeding facilitating the removal of fibrovascular membranes, particularly when preoperative PRP cannot be placed.
The purpose of this retrospective case series is to report the development or progression of tractional retinal detachment (TRD) following intravitreal bevacizumab as an adjuvant to vitrectomy for the management of severe PDR.
PATIENTS AND METHODS
We reviewed the medical records and obtained follow-up information on all patients in our files with TRD who had undergone intravitreal injection of 1.25 mg bevacizumab before vitrectomy for the management of PDR from September 2005 to November 2006 at seven centres from Brazil, Argentina, the USA, Costa Rica, Puerto Rico and Venezuela. The “off-label” status of this medication, and possible systemic and ocular complications, were discussed in detail and informed consent was obtained from all patients. Institutional review board/ethics committee approval was obtained for this study at all seven institutions.
Pre-injection examination included Snellen or Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity measurement, slit-lamp biomicroscopy and dilated fundus examination. Although not a formal exclusion criterion, patients with a history of uncontrolled hypertension and recent thomboembolic events were not usually injected with bevacizumab; however, this decision was taken at the discretion of the treating physician. Inclusion criteria for the use of intravitreal bevacizumab before vitrectomy for the management of PDR included TRD, persistent vitreous haemorrhage and incomplete regression even after extensive PRP.
An aliquot of commercially available bevacizumab (0.18 ml) was prepared for each patient and placed in a tuberculin syringe using aseptic techniques. After the eye had been prepared in a standard fashion using 5% povidone/iodine, an eyelid speculum was used to stabilise the eyelids, and the injection of 1.25 mg (0.05 ml) bevacizumab was performed 3.5–4 mm posterior to the limbus, through the pars plana with a 30-gauge needle under topical anaesthesia or subconjunctival lidocaine. Following the injection, intraocular pressure and retinal artery perfusion were confirmed, and patients were instructed to administer topical antibiotics for 3–7 days.
Statistical analysis was performed using GraphPad Instat Version 3.0 for Mac OSX (GraphPad Software, San Diego, CA, USA). Patients’ BCVAs were transferred from their records and converted to a logarithm of the minimal angle of resolution (logMAR) scale for analysis. The paired t test was used to compare mean values to analyse mean logMAR visual acuity statistically. Correlation was considered significant if the p value was ⩽0.05.
RESULTS
Eleven eyes (patients) out of 211 intravitreal injections (5.2%) that developed or had progression of TRD were identified. All patients had had a PRP at least 2 months before intravitreal bevacizumab. All eyes had PDR refractory to PRP. Eight (72.7%) patients were white and 3 (27.3%) patients were Hispanic. The mean age of the study group was 39.5 years (range 22–62 years), and 54.5% were male (six men and five women). Nine patients had type 1 diabetes mellitus (DM) with more than 15.5 years from diagnosis (range 14–30 years), and two patients had type 2 DM with 1 year from diagnosis. In the current study, all patients used insulin administration for glycaemic control and had uncontrolled diabetes associated with elevated glycosylated haemoglobin (mean HbA1c 10.6%). Seven eyes had local TRD on indirect ophthalmoscopy, ultrasound, or biomicroscopic non-contact fundus examination with a 66- or a 78-diopter lens before intravitreal bevacizumab. The clinical findings of all 11 eyes with PDR and TRD after intravitreal bevacizumab are presented in table 1.
Time from injection to TRD was a mean of 13 days (range 3–31 days). The mean baseline (before intravitreal bevacizumab) BCVA was LogMAR 0.8 (range 0.3–1.6) (mean Snellen equivalent 20/125; range 20/40 to 5/200). At TRD development or progression, the mean BCVA was LogMAR 2.2 (range 1.0–2.6) (mean Snellen equivalent hand motions (HM); range 20/200 to light perception (LP)), a statistically significant worsening compared with baseline BCVA (p<0.0001). One patient (case 9) developed a retinal break as a result of the increased traction, and a combined total tractional-rhegmatogenous retinal detachment was apparent 3 weeks after intravitreal bevacizumab.
Eight eyes underwent vitrectomy, two patients refused or were unable to undergo surgery, and in one patient surgery was not recommended. Vitrectomy was performed within 10 days after the development or progression of TRD. Tractional retinal detachments were managed with vitrectomy, membranectomy, photocoagulation and extended intraocular tamponade with gas in all patients that underwent surgery. Final mean BCVA after surgery was LogMAR 0.9 (range 0.2–2.0) (mean Snellen equivalent 20/160; range 20/32 to counting fingers (CF)), a statistically significant improvement compared with TRD BCVA (p = 0.002). Sub-group analysis of final BCVA after vitrectomy demonstrated that all eight (100%) eyes improved two or more ETDRS lines of BCVA compared with TRD BCVA. However, compared with baseline BCVA, final BCVA after vitrectomy demonstrated that four (50%) eyes improved, two (25%) eyes remained stable, and two (25%) eyes lost two or more ETDRS lines of BCVA (table 1).
Selected case reports
Case 6
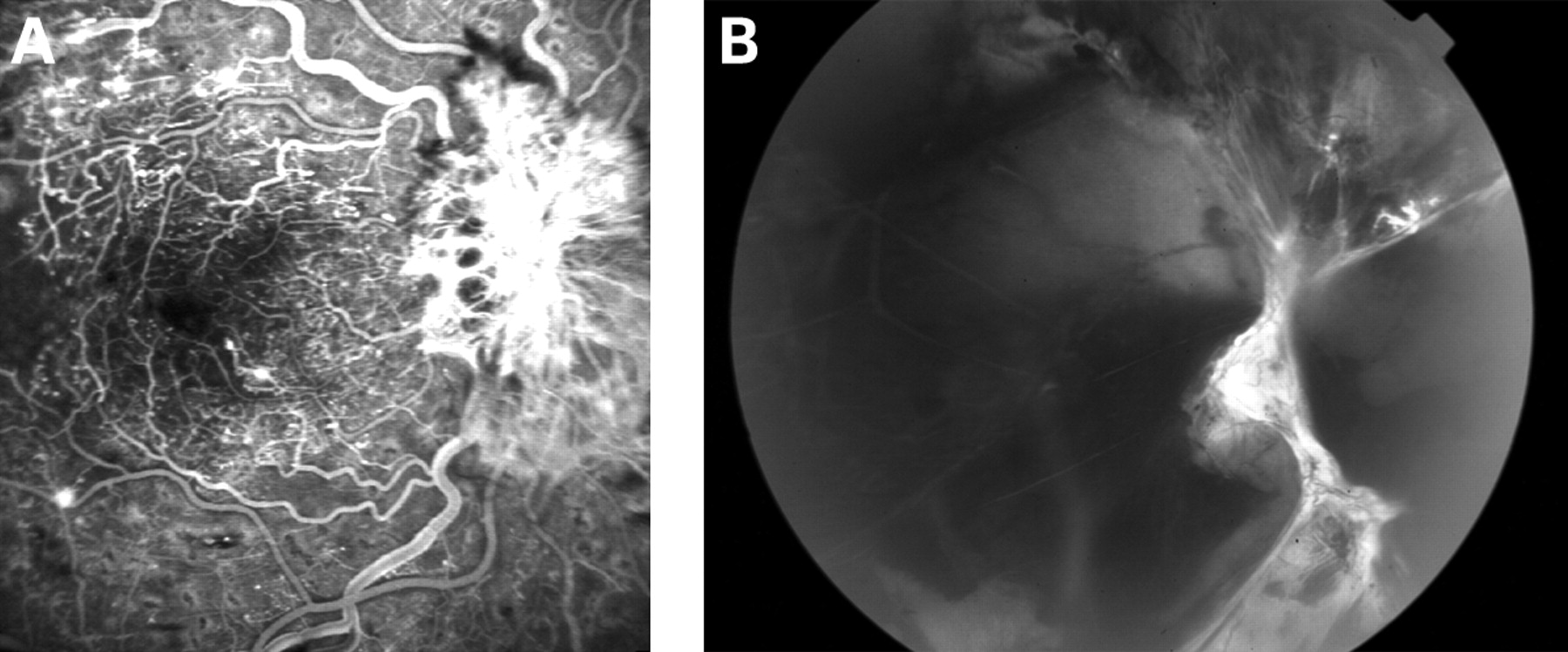
A 22-year-old woman with a history of poorly controlled type 1 DM since age 6 years presented with bilateral PDR. She had a history of panretinal photocoagulation in her right eye. At presentation, her BCVA was 20/200 and fundus examination revealed NVD of 6 disc diameters emanating from the optic disc into the vitreous cavity without any signs of bleeding (fig 1A). Intravitreal bevacizumab at a dose of 1.25 mg was injected into the vitreous cavity in preparation for a vitrectomy for incomplete regression even after extensive PRP. Four days later the patient returned complaining of a sudden visual loss in her right eye. A dense vitreous haemorrhage was present. Extensive fibrovascular proliferation extending from the optic nerve into the vitreous cavity was causing a partial TRD (fig 1B). Pars plana vitrectomy was performed 5 days later. Panretinal photocoagulation was completed and 20% SF6 was left as intraocular tamponade. The retina was successfully re-attached and she recovered BCVA of 20/50 at her final follow-up (20 weeks).
Case 7
A 45-year-old Hispanic man presented with a 1-month history of visual loss in his left eye. He had poorly controlled type 2 DM diagnosed 1 year earlier. His vision was 20/80 in his right eye and HM in his left eye. He had severe PDR in the right eye with a small localised TRD along the superior temporal arcade (fig 2A). The left eye had dense vitreous haemorrhage without evidence of retinal detachment by ultrasound. His right eye received an intravitreal injection of 1.25 mg bevacizumab in preparation for a vitrectomy. Three weeks later he complained of sudden loss of vision in his right eye, and was noted to have HM vision due to vitreous haemorrhage and a TRD (fig 2B). Vitrectomy was performed the next day in his right eye. His BCVA returned to 20/400 and has been stable for the past 8 months.

{kind=link}
{kind=link}
DISCUSSION
Recently, intravitreal bevacizumab has become popular as a preoperative coadjuvant in cases of severe PDR.19 20 Preoperative suppression of intraocular VEGF should reduce intraoperative haemorrhaging during membrane dissection facilitating the surgery. In our retrospective review, we identified 11 eyes (patients) with development or progression of TRD with decrease BCVA after intravitreal bevacizumab prior to vitrectomy for the management of PDR for an incidence of 5.2%.
The natural course of PDR is characterised by a cycle of proliferation and regression typical of new vessels; proliferation of fibrous tissue accompanying new vessels; formation of adhesions between the fibrovascular proliferations and the posterior vitreous surface; and contraction of the posterior vitreous surface and associated proliferation. The development or progression of TRD in PDR following intravitreal bevacizumab in our patients could have happened by natural history or rapid neovascular involution with accelerated fibrosis and posterior hyaloidal contraction as a response to decreased levels of VEGF.
It could be argued that TRD may develop soon after extensive PRP in diabetes. In addition, all our patients were refractory to extensive PRP. However, all patients had had a PRP at least 2 months before intravitreal bevacizumab. The short time interval between the injection and TRD (mean 13 days; range 3–31 days) suggests a cause–effect relationship. It also suggests that in cases at risk for progression of TRD that might involve the central macular region, timely surgery should be anticipated following intravitreal bevacizumab. Nine out of 11 (81.8%) TRDs developed or progressed 5 days or more after the injection. All patients who developed or had progression of TRD in our study used insulin administration for glycaemic control, and nine patients had elevated HbA1c (⩾9.5%; mean 10.6%).
Avery et al20 have reported that diabetic eyes may be very sensitive to intravitreal bevacizumab. In their study, several patients underwent intravitreal injection of lower doses of bevacizumab: 6.2, 12.5, 62, 125 and 625 μg. Biological effects were noted at all doses, sometimes at 24 h. The durability of this effect is unknown, and larger doses may be shown to produce a longer duration of effect, but to use lower doses seems prudent in eyes with pre-existing significant traction.
In those eyes that underwent vitrectomy, we had the impression that there was a reduced risk of intraoperative bleeding facilitating the removal of fibrovascular membranes. A bloodless field allows for better visibility and the surgeon may be less likely to create an iatrogenic retinal break. In addition, the chances of postoperative complications such as rebleeding or fibrinoid syndrome may be decreased. All these advantages may allow us to save more eyes by utilising preoperative intravitreal bevacizumab regardless of increased traction on some severe PDR cases. In addition, in our TRD cases that underwent vitrectomy, final BCVA was significantly better than BCVA before surgery and when TRD was present.
In summary, TRD in PDR may occur or progress after intravitreal bevacizumab used as an adjuvant to vitrectomy. Most patients had poorly controlled DM associated with elevated HbA1c, insulin administration, PDR refractory to panretinal photocoagulation, and a longer time interval between intravitreal bevacizumab and vitrectomy.
Acknowledgments
The authors would like to thank the Pan-American Collaborative Retina Study Group (PACORES) for contributing patients to this case series.
REFERENCES
Footnotes
Competing interests: R L Avery and D J Pieramici are consultants for Genentech. The other authors have no proprietary or financial interest in any products or techniques described in this article.
Funding: Supported in part by the Foundation for Science Support from Sao Paulo (FAPESP), São Paulo – SP, Brazil, the Arevalo-Coutinho Foundation for Research in Ophthalmology (FACO), Caracas, Venezuela, and the California Retina Research Foundations, Santa Barbara, CA, USA.