Article Text

Abstract
Aim: To describe the diagnostic and therapeutic management of cytomegalovirus (CMV) anterior uveitis unassociated with retinal necrosis in immunocompetent patients.
Methods: Patients referred between 2001 and 2003 for management of unilateral, chronic, recurrent uveitis associated with secondary glaucoma underwent extensive investigation including laboratory tests for herpes virus infections. Specific antiviral treatment was initiated in all cases and the level of ocular inflammation was evaluated during the follow up.
Results: Five patients, three men and two women, were included. Median age was 50 years old (range 30–80 years). Anterior unilateral uveitis without iris atrophy was observed in all cases. Uveitis was chronic in three cases and recurrent in two cases. Glaucoma was observed in all patients with a median intraocular pressure of 30 mm Hg (range 22–43 mm Hg). Five patients responded initially to specific anti-CMV therapy. Even though glaucoma surgery was necessary in two cases, both ocular inflammation and glaucoma were controlled in all cases. Relapses occurred in three cases after cessation of therapy, requiring prolonged maintenance therapy with valganciclovir.
Conclusions: CMV infection and specific antiviral therapy should be considered in all cases of relapsing or chronic iridocyclitis and secondary glaucoma. Maintenance regimens of valganciclovir may be necessary to prevent further relapses.
- CMV, cytomegalovirus
- EBV, Epstein-Barr virus
- HSV, herpes simplex virus
- IgG, immunoglobulin G
- KP, keratic precipitates
- PCR, polymerase chain reaction
- PSS, Posner-Schlossman syndrome
- PVU, presumed viral uveitis
- VZV, varicella zoster virus
- anterior chamber paracentesis
- cytomegalovirus
- uveitis
- ganciclovir
- glaucoma
- polymerase chain reaction
- Posner-Schlossman syndrome
- CMV, cytomegalovirus
- EBV, Epstein-Barr virus
- HSV, herpes simplex virus
- IgG, immunoglobulin G
- KP, keratic precipitates
- PCR, polymerase chain reaction
- PSS, Posner-Schlossman syndrome
- PVU, presumed viral uveitis
- VZV, varicella zoster virus
- anterior chamber paracentesis
- cytomegalovirus
- uveitis
- ganciclovir
- glaucoma
- polymerase chain reaction
- Posner-Schlossman syndrome
Statistics from Altmetric.com
- CMV, cytomegalovirus
- EBV, Epstein-Barr virus
- HSV, herpes simplex virus
- IgG, immunoglobulin G
- KP, keratic precipitates
- PCR, polymerase chain reaction
- PSS, Posner-Schlossman syndrome
- PVU, presumed viral uveitis
- VZV, varicella zoster virus
- anterior chamber paracentesis
- cytomegalovirus
- uveitis
- ganciclovir
- glaucoma
- polymerase chain reaction
- Posner-Schlossman syndrome
- CMV, cytomegalovirus
- EBV, Epstein-Barr virus
- HSV, herpes simplex virus
- IgG, immunoglobulin G
- KP, keratic precipitates
- PCR, polymerase chain reaction
- PSS, Posner-Schlossman syndrome
- PVU, presumed viral uveitis
- VZV, varicella zoster virus
- anterior chamber paracentesis
- cytomegalovirus
- uveitis
- ganciclovir
- glaucoma
- polymerase chain reaction
- Posner-Schlossman syndrome
Cytomegalovirus (CMV), a member of the herpes virus family, is known to be the most common cause of acquired viral retinitis in immunocompromised hosts.1 CMV infection causes both acute retinitis and anterior uveitis in immunocompromised patients, most of whom have AIDS, and is rarely seen in immunocompetent individuals. Recently, the spectrum of CMV related intraocular infections in immunocompetent individuals has been expanded to include apparent infections of the anterior segment with concomitant anterior uveitis, but without a typical retinitis.2 We report an additional series of five cases in whom the presence of cytomegalovirus infection was confirmed by antibody determinations and/or polymerase chain reaction (PCR) of aqueous humour from eyes with chronic anterior uveitis, but without posterior segment disease.
PATIENTS AND METHODS
We retrospectively reviewed the charts of five patients, examined between 2001 and 2003 at the Pitié-Salpêtrière Hospital, Paris, France, or at the University of Miami School of Medicine, Miami, Florida, USA. Anterior chamber paracentesis for the diagnosis of idiopathic unilateral chronic or recurrent uveitis was performed and CMV DNA was found in aqueous humour in all patients. The study complied with the policies of the respective review boards. Informed consent was obtained in all cases. The same diagnostic strategy has been reported to yield a specific viral diagnosis in 86.4% of patients with necrotising herpetic retinitis.3 As controls, 10 aqueous humour samples from patients with clinical features of an active uveitis (toxoplasmosis, syphilis, sarcoidosis) were analysed.
PCR analysis of the aqueous humour for herpesviruses (herpes simplex viruses, HSV-1, HSV-2, varicella zoster virus (VZV), CMV, and Epstein-Barr virus (EBV)) was performed using a commercially available assay (one patient, University of Miami) or according to the following protocol (four patients, Pitié-Salpêtrière Hospital). Volumes of 10–20 µl of aqueous humour were used for each PCR reaction. PCR assays were performed using previously published primers.3 The sensitivity of these tests for detection of CMV is 10−5 copies ×106/l.
Antibody determinations were performed in cases 1–4 using the Enzygnost anti-VZV, anti-HSV, and anti-CMV immunoassays (Dade Behring) that allow detection and quantitative determination of IgG antibodies. We compared values obtained in serum and aqueous humour at the same dilution. Intraocular synthesis of specific antibodies was evidenced by calculating the ratios of titres of IgG directed to various antigens in serum with those observed in aqueous humour. This approach is similar to that we use for the determination of intrathecal (cerebrospinal fluid) synthesis of specific antibodies, in cases of viral encephalitis.4 It is based on the determination of the values of specific antibody titres directed towards various viruses (HSV, VZV, and CMV) in serum and eye, analysed at same dilutions. The serum to eye ratios of various specific antiviral antibodies are then compared with each other, to rule out possible diffusion of antibodies from the serum. Focal specific antibody production is defined either by a serum to eye ratio lower than 100 and/or by a relative ratio at least superior to 4 in favour of CMV IgG.
RESULTS
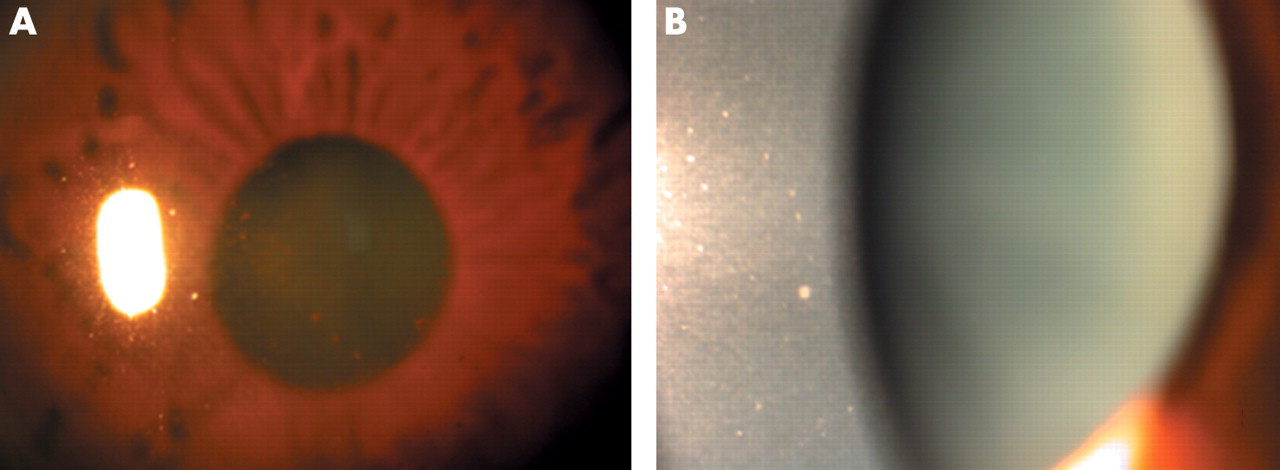
All patients had unilateral chronic or recurrent anterior uveitis and were HIV negative (table 1). Median age was 45 years old (range 17–80 years). Aciclovir was previously used in two cases without efficacy. All patients were receiving antiglaucoma agents at initial examination and were suspected of steroid responsiveness before viral identification. Median intraocular pressure was 30 mm Hg (range 22–40 mm Hg). Viral replication was associated with ocular hypertension even though antiviral therapy did not resolve this issue in two cases with further glaucoma surgery. Steroid responsiveness is another aetiological factor, especially in these two patients. Systemic investigation revealed no immunological defect. Other infectious serologies were non-contributory. Inflammation had been present for a median of 8 years (range 3 months–43 years) before confirmation of viral infection. Three patients had brown active appearing keratic precipitates (KP), which were initially interpreted as indicating pigment dispersion, but none showed iris atrophy or transillumination defects (fig 1). Fundus examination, fluorescein angiography and/or optical coherence tomography excluded posterior segment involvement including peripheral retinal vasculitis and macular oedema.
Demographic and clinical features of patients presenting with CMV uveitis

Keratic precipitates (KP) in patients with CMV uveitis. (A) Multiple brown KP predominantly in the inferior part of the cornea in a patient with presumed viral uveitis. (B) Central white-grey KP in the central cornea of a patient with Posner-Schlossman-like syndrome.
PCR tests of aqueous humour were positive for CMV and negative for other viruses (table 2). PCR was negative for herpes viruses in all controls with other aetiologies of uveitis. Specific intraocular production of anti-CMV IgG antibodies was detected in cases 1–4. In three cases (2–4), very high ocular concentrations of CMV specific IgG were evidenced by high titres in the eye with serum to eye ratios of 9, 14, and 40 respectively, whereas no HSV or VZV specific IgG were present in the eye despite high IgG titres in the serum. In case 1, which was PCR positive in two different samples, the serum to eye ratio of CMV IgG was 90 at a late stage of disease whereas HSV and VZV IgG were undetectable in the eye despite elevated titres in serum.
Laboratory confirmation of CMV infection and visual outcome of patients after specific antiviral therapy
Specific anti-CMV therapy was started in all patients after diagnostic testing (table 2). Intravenous ganciclovir or foscarnet were administered for cases 1–4 at an induction course for at least 2 weeks followed by oral valganciclovir (450 mg twice a day) for a period of 2 months (see fig 2). Case 5 was treated with oral valganciclovir only. Topical corticosteroids were tapered and treatment for glaucoma continued as indicated. Relapses occurred in three patients after cessation of therapy (table 2). PCR testing was positive in these three patients after each relapse. Valganciclovir was restarted with control of inflammation. After a 6 month period of re-treatment they remained asymptomatic and free of inflammation off medication with a mean follow up period of 14 months.

{kind=link}
{kind=link}
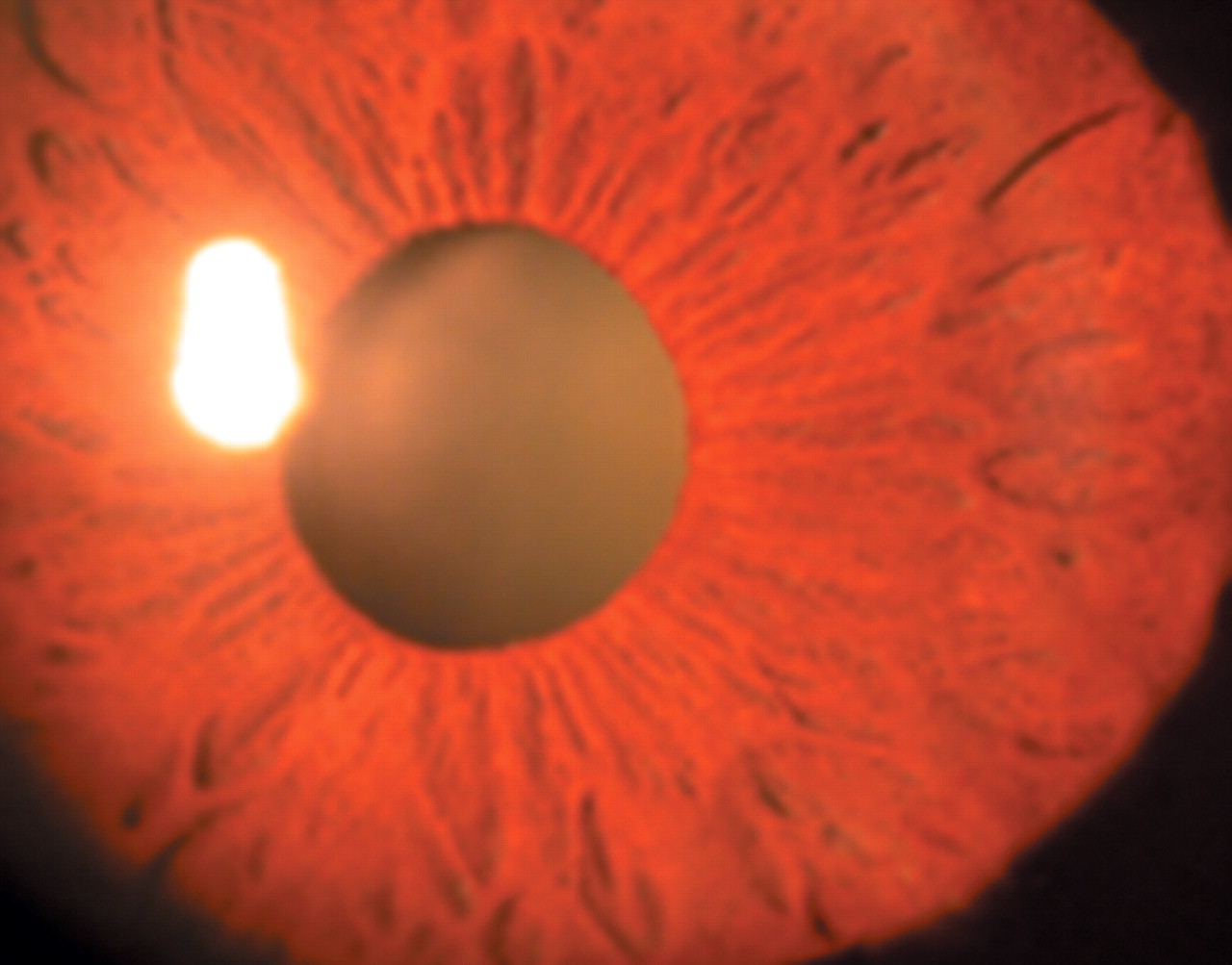
Same patient as in figure 1A, keratic precipitates and secondary glaucoma improved 2 weeks after an induction regimen of intravenous ganciclovir.
DISCUSSION
Analysis of ocular fluids in patients with suspected viral uveitis is useful in confirming the infectious aetiology. Although this technique is most often used in the cases of necrotising herpetic retinitis,3,5,6, herpetic iridocyclitis has also been diagnosed in this manner.7 Usually cases with unilateral anterior uveitis and iris atrophy associated with secondary glaucoma are selected for testing of intraocular fluids for antibodies or viral DNA. In this series, patients with chronic, long lasting or recurrent anterior uveitis were found to have CMV as the causative virus, therefore allowing us to propose specific anti-CMV therapy that resulted in remission in the majority of patients after failure of previous treatments with aciclovir and/or topical corticosteroids.
Similar cases have been reported. In 2000, Mietz et al reported local synthesis of anti-CMV antibodies in the aqueous humour of a patient with anterior uveitis, but PCR testing was negative for CMV, VZV, and HSV.8 Therapeutic response to ganciclovir suggested that inflammation might be related to CMV infection. Two cases of recurrent anterior uveitis with sectoral iris atrophy were previously ascribed to CMV, based upon a positive PCR from aqueous humour taken during a phase of active uveitis.2 This series expands the number of confirmed cases of anterior uveitis related CMV infection in immunocompetent patients to eight.
Systemic CMV infection of immunocompetent patients is rarely symptomatic. Approximately 80–85% of adults have anti-CMV antibodies by the age of 40.9 In contrast, in severely immunocompromised patients, CMV is a common opportunistic pathogen with symptomatic posterior segment involvement reported in up to two thirds of patients with AIDS before the widespread use of highly active antiretroviral therapy. Despite this, isolated anterior segment involvement was not recognised as a clinical syndrome among AIDS patients although histological evidence of anterior infection with CMV was reported in autopsy cases.10 The absence of a recognised syndrome of CMV associated iridocyclitis in AIDS patients suggests that there is a prominent immunological component in the development of symptomatic iridocyclitis in infected immunocompetent patients. Alternatively, the anterior inflammation noted in a small number of HIV infected patients with CMV retinitis may be the result of anterior segment infection rather than purely a response to the retinal involvement.
Based on slit lamp biomicroscopy, our cases presented initially with clinical features of presumed viral uveitis (PVU) or Posner-Schlossman syndrome (PSS). Chronicity is a major characteristic of PVU. Ocular inflammation persists for a long time and seems to be mild to moderate (low flare values). The absence of sectoral iris atrophy made a possible herpetic infection less probable, since its presence has been considered almost pathognomonic of herpetic infection, but the absence of iris atrophy does not exclude a viral origin. The recurrent episodes of hypertensive iridocyclitis with grey-white medium to large sized KPs, the absence of posterior synechiae, and the white eye with only mild anterior chamber reaction are highly suggestive of PSS. The possible role of CMV in the pathogenesis of PSS was previously highlighted by Bloch-Michel et al based on intraocular production of anti-CMV antibodies.11 Interestingly, Teoh et al have recently reported a case of CMV induced PSS in an immunocompetent patient. Virological confirmation was based on quantitative PCR applied to aqueous humour.12
PCR testing for CMV was positive in all patients included in our small series. This technique is highly sensitive. However, PCR confirms the presence of CMV genome in the aqueous humour but does not confirm productive infection. The high sensitivity of PCR can produce false positive results. Although the analysis of locally produced antibodies is less sensitive, both tests contribute to precise diagnosis. The detection of intraocular synthesis of anti-CMV antibodies suggests active intraocular infection and offers the potential for effective treatment.8 Otherwise, detection of CMV antibodies in aqueous humour can be falsely positive because of diffusion of antibodies from the sera across a disrupted blood-aqueous barrier. The association of local CMV specific antibody production and PCR positivity is a strong argument for CMV infection.
Further evidence for CMV as the aetiological factor in these cases of iridocyclitis is the positive response to specific anti-CMV drugs and relapses after discontinuation of antiviral drugs. Despite clinical features similar to a viral involvement, patients were all clinically unresponsive to aciclovir. CMV is usually resistant to aciclovir. Furthermore, trabeculitis seems to be a consistent complication that becomes resistant to medical antiglaucomatous therapy in the absence of specific anti-CMV therapy.
In our case series, the therapeutic strategy was one of trial and error and the need to switch from one antiviral drug to another. In the two cases of anterior uveitis in immunocompetent patients reported by Markomichelakis et al, treatment with oral aciclovir controlled inflammation temporarily, but recurrences continued and a change to ganciclovir controlled inflammation.2 Therapy was continued for 1 and 2 years, respectively. Switching to ganciclovir or valganciclovir was successful in the first four cases. Maintenance therapy should be proposed in all cases and followed for at least 2 months in the absence of systemic side effects. In the face of any further relapses, duration of maintenance therapy should be increased. Interestingly, specific anti-CMV therapy was not able to control secondary glaucoma in two cases of the present series. This condition was not reported previously and may be attributed to chronic irreversible trabecular alterations requiring further surgery. Similar situations are associated with chronic anterior herpetic uveitis.
At this point, it is difficult to propose a minimal period of antiviral therapy considering the small case series. Although conventional treatment, based on topical corticosteroids and antiglaucomatous drugs, for patients with PSS may be effective, it is possible that a course of specific antiviral therapy would reduce the risk of recurrent attacks.
In summary, this is the first report of various atypical cases of CMV induced uveitis in immunocompetent patients. In cases of unilateral anterior chronic hypertensive uveitis of unclear origin, clinically unresponsive to aciclovir and its analogues, diagnosis of CMV uveitis may be ruled out since an adequate therapeutic approach needs to be initiated as soon as possible. Larger series are necessary to define other clinical entities and the best therapeutic strategy to control uveitis and secondary glaucoma, but also to avoid further recurrences.
Linked Articles
- BJO at a glance
- Editorial