Article Text

Abstract
The number of patients seen with glaucoma related pathologies is predicted to increase significantly over the next few years as a result of an ageing population, increased optometric screening, and raised public awareness. In addition, the recent glaucoma literature proposes more aggressive management of ocular hypertension, open angle glaucoma, and narrow angle pathologies. This will overburden many glaucoma services and demands a reappraisal of current management strategies. Using a database of patients compiled from their tertiary referral glaucoma service as an example, the authors discuss the current controversies relating to each glaucoma subtype, encompassing issues relating to disease prognosis, efficacy of treatment, and resource management. They also suggest a range of strategies aimed at streamlining glaucoma clinics. Examples include shared care schemes, multidisciplinary teams, clinic guidelines/protocols, and alteration of clinic review times. The predicted effect of such schemes on clinic workloads is discussed, together with any existing validation.
- ACG, angle closure glaucoma
- BRVO, branch retinal vein occlusion
- CRVO, central retinal vein occlusion
- HRT, Heidelberg retina tomograph
- HRVO, hemiretinal vein occlusion
- IOP, intraocular pressure
- NLES, North London Eye Study
- OHT, ocular hypertension
- PAC, primary angle closure
- PACG, primary angle closure glaucoma
- PI, peripheral iridotomy
- POAG, primary open angle glaucoma
- RTA, retinal thickness analyser
- glaucoma
- service
- hypertension
- shared care
- ACG, angle closure glaucoma
- BRVO, branch retinal vein occlusion
- CRVO, central retinal vein occlusion
- HRT, Heidelberg retina tomograph
- HRVO, hemiretinal vein occlusion
- IOP, intraocular pressure
- NLES, North London Eye Study
- OHT, ocular hypertension
- PAC, primary angle closure
- PACG, primary angle closure glaucoma
- PI, peripheral iridotomy
- POAG, primary open angle glaucoma
- RTA, retinal thickness analyser
- glaucoma
- service
- hypertension
- shared care
Statistics from Altmetric.com
- ACG, angle closure glaucoma
- BRVO, branch retinal vein occlusion
- CRVO, central retinal vein occlusion
- HRT, Heidelberg retina tomograph
- HRVO, hemiretinal vein occlusion
- IOP, intraocular pressure
- NLES, North London Eye Study
- OHT, ocular hypertension
- PAC, primary angle closure
- PACG, primary angle closure glaucoma
- PI, peripheral iridotomy
- POAG, primary open angle glaucoma
- RTA, retinal thickness analyser
- glaucoma
- service
- hypertension
- shared care
- ACG, angle closure glaucoma
- BRVO, branch retinal vein occlusion
- CRVO, central retinal vein occlusion
- HRT, Heidelberg retina tomograph
- HRVO, hemiretinal vein occlusion
- IOP, intraocular pressure
- NLES, North London Eye Study
- OHT, ocular hypertension
- PAC, primary angle closure
- PACG, primary angle closure glaucoma
- PI, peripheral iridotomy
- POAG, primary open angle glaucoma
- RTA, retinal thickness analyser
- glaucoma
- service
- hypertension
- shared care
The management of patients with glaucoma, or those at risk of the disease, currently constitutes a major part of the workload of the general ophthalmologist. In one UK unit, 8% of primary care referrals were found to be glaucoma related,1 while earlier data from another hospital eye service revealed that 25% of follow up attendances and 13% of new referrals were either glaucoma suspects or patients with glaucoma.2 By extrapolating data from the North London Eye Study (NLES),3 the Royal College of Ophthalmologists suggests that, at present, there are 570 000 suspected cases and 15 000 definite cases of primary open angle glaucoma (POAG) in the United Kingdom.4 More importantly, as the population ages and optometric screening increases in efficiency, these numbers are likely to increase. Estimates based on official population projections and epidemiological prevalence surveys have predicted that the number of cases of POAG in England and Wales will increase by a third by 2021, and then continue upwards at a similar pace to 2031.5 Such figures clearly demand a reappraisal of current hospital glaucoma services, which are often already under-resourced. This is especially pertinent given the more aggressive treatment regimes proposed in the recent literature regarding this disease group.6,7,8,9,10
In order to assess and improve our glaucoma service at Moorfields Eye Hospital, we have developed a database with the aim of recording all patients attending the glaucoma clinics. This is not yet complete, but includes approximately 90% of patients at outreach clinics that are using this system. Other outreach clinics and our tertiary referral clinics remain only partially represented. To date there are 7186 patients on the database, for which the diagnostic composition is shown in table 1.
Database of patients attending Moorfields’ glaucoma service
The group of “other” glaucomas includes congenital and secondary forms. These comprise a small number of patients that require regular hospital supervision and will not be discussed further here. However, the management of all four other groups bears consideration in the light of the changes mentioned above.
PRIMARY OPEN ANGLE GLAUCOMA
As can be seen from the clinic profile given, POAG patients constitute the largest group of patients followed up in the glaucoma clinics. There is no doubt that, until such a time as we can distinguish progressive from non-progressive disease, all of these patients need to be reviewed. Their numbers, however, make it critical that follow up is done as efficiently as possible. This is of particular importance for the many stable glaucoma patients. How best to go about this has been the subject of much debate over the past 10 years and several ideas have been discussed. A popular option has been the use of a multidisciplinary team of glaucoma assessers, as first suggested by the Optical Services Audit Committee in 1990,11 in reference to increasing the contribution made by optometrists. This prompted an interest in community shared care schemes12–15 and was followed by guidelines on shared care issued by the Royal College of Ophthalmologists in 1996.16 These recommended shared care for patients with stable glaucoma and ocular hypertension, where it was not possible to provide an adequate service in the hospital outpatient department. Criteria were given for the suitability of patients, including standardised measurements, optometric training, frequency of follow up, referral protocols, lines of communication, validation, audit, and funding. More recently, a Department of Health Working Party on Glaucoma Care Pathways has been established to discuss potential shared care strategies.17 This has proposed the use of specialist community optometrists who have been trained in glaucoma management and who have prescribing rights.
One such shared care scheme has recently been evaluated in Bristol.18 A total of 403 stable glaucoma patients were randomised to either 6 monthly optometric review by trained community optometrists,19 or to the hospital eye service. Patients were only included if they had stable POAG or ocular hypertension (OHT), visual acuity greater than 6/18 in both eyes, and were fully cooperative. A research team evaluated all patients before randomisation and at 2 years.20 Results showed no significant differences in any of the key visual variables, or procedures undertaken, between the two groups. However, patients under optometric review were frequently re-referred to the hospital service, most commonly for changes in the visual field. Patient satisfaction was significantly higher for many aspects of community care, especially timekeeping and travel.21 However, the costs of community optometric follow up significantly exceeded hospital follow up, at an annual cost per patient of £70–£110 compared with £15–£60. This cost was, in part, because of the expense of optometric referral back to the hospital service. In addition, only a subgroup of clinic patients was actually eligible for entry into the scheme.
Another approach to the problem of overburdened clinics has been to use a multidisciplinary team within the hospital setting.22 Such a system is widely used in our own department and involves trained optometrists and nurse practitioners seeing stable glaucoma patients. Proformas can help to streamline such clinics by forming a guide to staff and standardising consultations. If appropriate, the concept can be extended even further by having clinical guidelines relating to the frequency with which stable patients are seen and which tests should be performed at each visit. However, it is important that such hospital based schemes are subject to the same rigorous validation and audit that the Royal College of Ophthalmologists’ guidelines recommend for community shared care schemes.
The frequency of POAG reviews is another important factor that is far too frequently forgotten in the planning of clinic profiles. None the less, it has a tremendous impact on the service, as highlighted by the example given below. The requests for follow up from one typical specialist glaucoma clinic with 54 patients are shown in the first column of table 2. They result in an average requested clinic follow up time of 15.9 weeks.
Follow up appointment times in a specialist glaucoma clinic
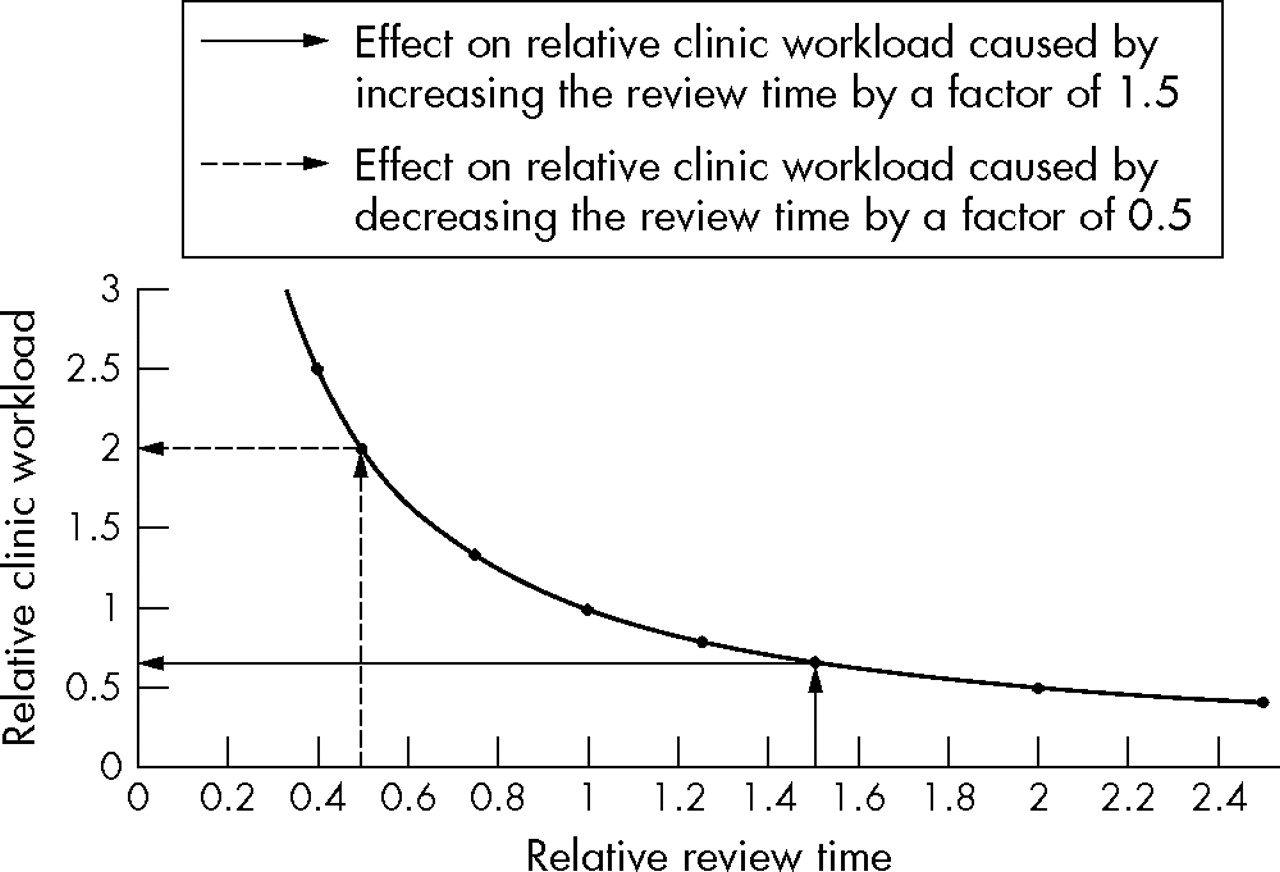
Assuming that requests for 1 week follow up are unmovable, increasing all other requests to the next time slot (that is, from 2 weeks to 3 weeks, from 3–4 months to 6–8 months, etc) will give you column two of table 1. This produces an average requested clinic follow up time of 23.6 weeks and increases the average clinic wait by a factor of 23.6/15.9 = 1.5. If sustained, this will alter the relative clinic workload in accordance with figure 1, which shows it drop to 0.7 of its previous level in this case.

Change in the relative clinic workload with relative review time.
Other scenarios can be modelled and plotted on figure 1 to get an idea of the impact on clinic workload. For example, if each of the patients in the clinic above were to be reviewed in the time slot earlier than that requested, as shown in column three of table 1, the average time to review would be decreased by a factor of a half. This would double the average clinic workload.
Altering clinic follow up times will also have an effect on the number of new patients seen, as illustrated in figure 2. In the specialist glaucoma clinic used as an example, 10% of clinic slots are for new referrals. If clinic follow up times increase by a factor of 1.5 then 4.3 times as many new patients can be seen in each clinic. In contrast, halving clinic follow up times will mean that all of the new patient slots are used up by follow ups and new referrals will either have to be overbooked into the clinic or have a tremendously long waiting time. This will result in them failing to meet charter standards.

{kind=link}
{kind=link}
Change in the relative number of new patients seen with relative review time.
Why do we review patients more often? Change in therapy is the most frequent trigger and is likely to increase as we aim for lower target intraocular pressures (IOPs), based on the evidence of many of the recent large multicentre glaucoma trials.6,7,8,9,10 In addition, increased patient awareness may lead to increased anxiety and a demand for more frequent review. Finally, with the development of a widening range of topical therapies there is a trend towards medical management with more changes of topical treatment regimens and fewer operations.23–25
The above discussion emphasises the consideration that must be given to follow up intervals when managing modern glaucoma clinics. In view of this it may be advisable for consultants to lay down general glaucoma follow up guidelines for their individual service.
GLAUCOMA SUSPECTS
Glaucoma suspects represent the significant number of patients who have been referred to the clinics as “query glaucoma” but in whom the clinical findings are inconclusive. Glaucoma is a dynamic disease and if present will manifest itself by progression with disc and field changes over time. The cohort of “suspects” are those individuals who need following in order to distinguish between normal variants and early glaucoma. This group forms the second largest subgroup on our database, comprising one third of the patients recorded.
Can this number be reduced? A policy of consultant review of all such patients would encourage patients to be discharged as soon as that decision could be made. However, a significant number of glaucoma suspects are still likely to remain because of a reluctance to discharge to community review. The reasons for the latter are twofold. Firstly, there is an anxiety that subsequent progression to frank glaucoma may not be spotted. Secondly, there is a worry that individuals may find themselves bounced between the hospital and high street optometrist leading to a loss of confidence in the periodic eye examinations they so importantly require. Both of these reasons may be addressed by close working relationships and established communication between hospitals and high street optometrists. Provision of “glaucoma cards” with basic information and disc photographs would facilitate this enormously. Similarly, information sheets explaining the spectrum of glaucomatous pathology would enhance patients’ understanding of seemingly conflicting diagnoses and improve compliance. The installation of telemedicine hardware may also have a place in community screening and diagnosis although, to date, this has not been used for glaucoma.
Shared care schemes, aimed at managing glaucoma suspects in the community, have been piloted in a few centres. One study, from Nottingham, assessed whether the distribution of locally agreed referral guidelines to all community optometrists reduced the number of false positive glaucoma suspect referrals to the hospital eye service.26 Data were collected on 207 new patients referred to one glaucoma clinic over two 12 month periods before and after the distribution of the guidelines. Referral accuracy was determined from subsequent hospital notes. Results showed that the number of false positive referrals was unchanged over this period. A second scheme, conducted in Manchester, looked at the effect of community refinement of glaucoma referrals by specially trained glaucoma community optometrists, to whom general optometrists could refer any glaucoma suspects.27 The specialist optometrists worked to an agreed set of referral criteria. This shared care scheme succeeded in reducing the number of referrals to the hospital eye service for suspect glaucoma by 40% and cost benefit analyses estimated a saving to the NHS of £17 per patient. Similar specially trained community optometrists have been included as an integral part of many recent proposals for shared care schemes.17
Finally, it is important to consider the impact that new diagnostic technologies will have on the management of glaucoma suspects. Several new methods of optic disc and nerve fibre imaging are emerging including scanning laser tomography (Heidelberg retina tomograph (HRT, Heidelberg Engineering)), scanning laser polarimetry (GDx nerve fibre analyser (Laser Diagnostic Technologies)), and laser optical cross sectioning (retinal thickness analyser (RTA, Talia Technology)). Such equipment has been reported to show progressive disc cupping and nerve fibre layer loss in patients before any detectable field defects, although longitudinal studies are somewhat limited.28,29 This result has prompted the term “pre-perimetric glaucoma.”
Such technologies are primarily being used as research tools but it is foreseeable that they will become widely available in optometric practices as well as hospital glaucoma units. They may well have a role in distinguishing true glaucoma patients from glaucoma suspects, but their widespread use may also pose several problems. Firstly, they may increase the number of glaucoma suspects being referred to the hospital eye service, augmenting the workload in glaucoma clinics. The number of false positive referrals may also increase because the specificity of the investigations is not 100%. At present these technologies are generally recommended for monitoring change over time or for use in the context of other glaucoma investigations.30–33 Refinement of test combinations and processes for screening has yet to be completed.34
Finally, there is a lack of randomised control data to suggest that early intervention after the detection of damage by any means other than static automated perimetry leads to a favourable benefit:risk outcome for the patient.33 This will put the treating ophthalmologist in a difficult position with regard to managing such referrals, until a time when the necessary trials are conducted.
OCULAR HYPERTENSION
Eyes with OHT are, by definition, normal eyes with an IOP above 21 mm Hg; a figure derived from the normal distribution of IOP within the population. A minimum of 2.5% of the total population served by a given eye department would be expected to have OHT. But what is their risk of progression to glaucoma and visual loss?
The OHTS study9 recently quoted patients with an IOP of more than 25 mm Hg as having a 4.4% chance of progression to POAG after 5 years if treated and a 9.5% risk if untreated, as defined by reproducible visual field abnormalities or disc deterioration. Recent work by a panel of glaucoma specialists35 used lessons learnt from risk assessment in coronary heart disease to try and address the risk of actual loss of vision in these patients. OHTS data were included, along with longer term data from two other population based studies that used legal blindness as a defined end point.36–38 Consideration was also given to the Early Manifest Glaucoma Trial,10 which reported a 50% reduction in risk of progression in treated patients with early manifest glaucoma. Certain studies such as the Collaborative Initial Glaucoma Treatment Study, which showed little field loss with maintenance of low IOP targets, were not suitable for inclusion in the analysis because of the lack of control data and limited follow up.8 All the data given above were applied to a mathematical model of disease progression. This gave an estimated risk of progression from OHT to unilateral blindness of 1.5%–10.5% in untreated patients and 0.3%–2.4% in treated patients over a 15 year period. From these estimates, between 12 and 83 patients with OHT would require treatment to prevent one patient from progressing to unilateral blindness over this time. However, it was emphasised that this number was highly dependent on the patient subgroup in question, being greater for low risk patients and smaller for high risk patients.
What is therefore required is the identification of patients who are at greatest risk. As such, the same group of specialists recently reviewed the glaucoma literature to answer this very question.39 They found that, although many risk factors had been reported in the literature, those most strongly supported by evidence were a higher IOP, a greater cup-disc ratio, a thinner central cornea, and older age. In the OHTS, every 1 mm Hg increase in mean IOP level was associated with a 10% increased risk of progression from OHT to glaucoma.40 Similarly, hazard ratios for the development of POAG were raised by 25% for every 0.1 increase in the horizontal cup-disc ratio, and by 32% for every 0.1 increase in the vertical one. However, there has been some argument that increased cup-disc ratios in OHT patients may be an indication of structural damage and not a risk factor itself.41
A final controversial issue relating to the management of OHT has been the risk of vein occlusions. This has often been cited as a reason to treat all such patients. Certainly, an association between glaucoma and vein occlusions has been proposed in the literature for several decades, with glaucoma prevalence rates ranging from 6–69% in patients with central retinal vein occlusion (CRVO).42 Recently, the odds ratios for a positive history of glaucoma were given as 2.5 (1.5–4.2) for branch retinal vein occlusion (BRVO), 5.8 (3.7–9.1) for CRVO and 4.6 (2.3–9.5) for hemiretinal vein occlusion (HRVO).43 The relation also exists in reverse, with one study quoting a 4.2% rate of developing a vein occlusion in glaucoma patients over a 5 year period, compared to 0.59% in the equivalent general ophthalmic clinic.44
But does the same apply to ocular hypertension? The Eye Disease Case-Control Study Group43,45,46 suggests that this may be the case. Results showed no difference in cup-disc ratios between cases of BRVO, CRVO, or controls, but patients with CRVO were found to have a significantly higher IOP in the fellow eye, despite most already being on glaucoma medication bilaterally. In addition, a comparative case series evaluating the prevalence of both OHT and glaucoma in patients with CRVO and HRVO found a prevalence of glaucoma of 9.9% and of OHT of 16.2%.42 These studies support a hypertensive mechanism of damage and suggest raised pressure is the component of glaucoma most relevant to the association with vein occlusions. However, what remains unknown is the variation in risk with increasing IOP.
ANGLE CLOSURE GLAUCOMA
Patients with angle closure glaucoma (ACG) are fewer in number but are likely to increase given the raised awareness of narrow angle pathologies.47 If a patient has chronic ACG there are few who would disagree on the necessity for repeat review. However, does this apply to the preceding stages? Unfortunately, the literature on the natural progression of angle closure is scarce. Furthermore, definitions relating to the various disease stages have only just been formalised,47 which makes comparisons of studies complicated. Ideally, we would like to know the risk of progression of primary angle closure suspects (PACS) to primary angle closure (PAC) and subsequently to primary angle closure glaucoma (PACG), with and without intervention. This would enable an accurate risk-benefit analysis to be performed for such patients, as has been attempted for OHT.
Three population based studies exist that look at the risk of progression of untreated PACS to PAC. One, in white people, found that 19% developed PAC over 3 years with one third of those being acute.48 A case-controlled study from India49 re-examined 50 PACS patients after a 5 year interval and found that 22% had developed PAC. One control patient also progressed to PAC, giving a resultant relative risk of progression of 24 (95% CI 3.2 to 182.4). A third study50 looked at high risk Greenland Eskimos with shallow anterior chambers. It reported a much higher rate of progression from PACS to PAC after 10 years, at 35%, but interestingly, 8% of “controls” with normal angles and shallow anterior chambers also progressed. Although this population is high risk, it may partly reflect the type of patients referred to glaucoma services from optometric screening, as the latter tends to identify patients with shallow anterior chambers more readily than those with narrow angles on gonioscopy. Unfortunately, none of the studies found any factors that showed a high positive predictive accuracy in determining which PACS eyes would develop angle closure.
What is the risk further progression from PAC to PACG? This remains uncertain and is further complicated by the fact that PAC can either be acute or chronic and these diseases behave differently. A study from India51 reassessed 28 such patients after 5 years. All were advised to have laser peripheral iridotomy (PI) at the time of their original diagnosis, although only nine did. Overall, 29% progressed to PACG, with only one case arising from those who underwent laser PI. As with the PACS studies, no factors were identified that predicted progression. However, the study did confirm the therapeutic effect of laser PI on patients with PAC. This is supported by work from Mongolia,52 which found that iridotomy alone failed in only 3% of 164 chronic PAC eyes at 2 years. This was in contrast to a failure rate of 47% in eyes with established optic neuropathy (PACG).
The data on acute PAC are more abundant but do not relate to the long term risk of optic nerve damage. Most studies have used IOP as the principal outcome measure and have found good control of IOP with iridectomy or iridotomy alone in eyes of people of European descent, with success rates of 65%–76%.53–57 This is in contrast to Oriental patients where success rates are given as 42.8%.58 Of those patients not controlled, three quarters had IOP rises within the first 6 months. The only long term study of glaucomatous optic neuropathy after acute angle closure also relates to an Oriental population.59 It showed high glaucoma prevalence rates over 4–10 years of 47.8%, with 15.5% of eyes having a cup-disc ratio of >0.9. However, once again, no risk factors for progression were identified.
CONCLUSION
What does all of the above mean for the future of our clinics? Clearly, there are many uncertainties regarding the best management of glaucoma patients, both in terms of follow up and treatment. Much of the future is wrapped up in a more integrated, team based approach to patient care with the involvement of patients, optometrists, and hospital based healthcare professionals in any management strategies and decisions.
POAG patients certainly need regular review. Different multidisciplinary models exist for the management of referrals into the system and for controlling the ever increasing size of glaucoma clinics. However, many such schemes still need validation in the hospital setting, with assessment of their safety, acceptability, and cost effectiveness in particular. In the immediate term, close inspection of frequency of follow up appointments may release significant clinic capacity.
Glaucoma suspects require a reliable local system for regular review. Closer links between high street optometrists and hospital units are essential for this and are also likely to improve patient satisfaction and compliance in the long term. Further evidence regarding the management of “pre-perimetric glaucoma” is also required.
Patients with OHT have an increasing body of evidence for management strategies and many of these need not be purely hospital based. Risk factors such as the level of IOP, patient’s age, and corneal thickness should be utilised in discussing therapeutic strategies with patients. Once again, these management plans need to involve all groups of ophthalmic health professionals.
Angle closure patients require continued review, although follow up strategies should consider whether the patients are suspects or have frank angle closure glaucoma. Once again, local guidelines would be beneficial and require input from patients, high street optometrists, and hospital health professionals.
The workload of glaucoma clinics is likely to increase markedly in the next few years owing to an ageing population, increasing optometric case finding, raised public awareness, and more aggressive management of both OHT and POAG. Furthermore, new interest in the progression of angle closure and its contribution to glaucoma will cause a parallel increase in the management of narrow angle pathologies. This background demands that all glaucoma practitioners critically review their practice with a view to streamlining the service and adapting to the changing environment.
Acknowledgments
The authors thank Ruth Woode-Amissah for compiling the Moorfields’ glaucoma service database and one of our reviewers for their comments on “pre-perimetric” glaucoma.