Article Text

Abstract
Aim: To report on a new model of preschool vision screening that was performed in metropolitan Seoul and to investigate the distribution of various ocular disorders in this metropolitan preschool population.
Methods: Vision screening was conducted on 36 973 kindergarten children aged 3–5 years in a stepwise manner. The first step was home screening using a set of five picture cards and a questionnaire. The children who did not pass the first step (VA <0.5 in at least one eye or any abnormal responses on the questionnaire) were retested with regular vision charts at the regional public healthcare centres. After this retest, some children were referred to ophthalmologists. The referral criteria for visual acuity were <0.5 at 3 years and <0.63 at 4 or 5 years in at least one eye.
Results: Of those screened, 7116 (19.2%) children did not pass the home screening tests and 2058 (28.9%) out of the 7116 were referred. The results of the ophthalmological examination in eye clinics were only available for 894 children (43.4%) of those who were referred. The rest of the children did not visit ophthalmologists because they had been checked at an eye clinic, were currently under treatment, or for personal reasons. Refractive errors were found in 608 (1.6%) children. Astigmatism was associated in 78.2% of ametropes. Amblyopia was discovered in 149 (0.4%) children and refractive error was the major aetiology with a predominant rate (82.5%). Manifest strabismus was detected in 52 children. The positive predictive value of vision screening for any ophthalmological disorder was 0.77, and 0.49 for significant disorders requiring treatment.
Conclusions: This preschool vision screening model was highly accessible to the children and their parents, easy to administer, and effective to detect a variety of ocular disorders. However, the participation rate of the referred children in the examinations by ophthalmologists was quite low. The performance and efficiency of this screening programme need to be optimised with further revision.
- KFPB, Korean Foundation for the Prevention of Blindness
- PHC, public healthcare centres
- PPV, positive predictive value
- VA, visual acuity
- amblyopoa
- preschool vision screening
- refractive error
- Seoul
- South Korea
- KFPB, Korean Foundation for the Prevention of Blindness
- PHC, public healthcare centres
- PPV, positive predictive value
- VA, visual acuity
- amblyopoa
- preschool vision screening
- refractive error
- Seoul
- South Korea
Statistics from Altmetric.com
- KFPB, Korean Foundation for the Prevention of Blindness
- PHC, public healthcare centres
- PPV, positive predictive value
- VA, visual acuity
- amblyopoa
- preschool vision screening
- refractive error
- Seoul
- South Korea
- KFPB, Korean Foundation for the Prevention of Blindness
- PHC, public healthcare centres
- PPV, positive predictive value
- VA, visual acuity
- amblyopoa
- preschool vision screening
- refractive error
- Seoul
- South Korea
Undetected ocular disorders can cause serious problems in a child’s mental and social development. Important ocular disorders in children include amblyopia, strabismus, significant refractive error, and other various ocular diseases. Amblyopia is one of the most common causes of visual deficit in childhood. Amblyopia may cause an impaired reading performance when a child enters school, psychosocial difficulties later in life, and may preclude the individual from a particular occupation.1,2 According to the WHO recommendations for health related screening programmes, detection of ocular disorders in children is worthwhile because the condition is a serious health problem, reliable diagnostic tests are available, and effective treatment is possible at least in young children.3 The primary purpose of preschool vision screening is to detect amblyopia in order to initiate treatment as early in life as possible, and subsequently maximise a child’s visual potential.4–7 Unfortunately, many cases of amblyopia are not diagnosed until the child is too old to benefit from treatment.8
In South Korea, a regular preschool vision screening programme has been carried out since 1997 and a nationwide screening programme has been performed for three years. In Seoul, the capital of South Korea, which contains a quarter of the total national population, 113 000 children are born annually who should be screened for developmental visual deficits. Well organised screening efforts for these children would seem to be of value in this country.
The aim of this study is to report a new model of preschool vision screening that was performed in metropolitan Seoul and to investigate the distribution of various ocular disorders detected in this metropolitan preschool population. We believe that evaluating this preschool vision screening performance could help us determine the current need for action with regard to earlier and better vision screening programmes.
SUBJECTS AND METHODS
The Seoul Metropolitan Preschool Vision Screening Programme was part of the South Korean nationwide preschool vision screening programme that was conducted in 2001. We performed our preschool vision screening in a stepwise manner. The first step was home vision screening. In early March of 2001, a home vision test kit was sent to the parents of 36 973 kindergarten children aged 3–5 years. These subjects were identified from the Ministry of Health and Welfare database, which covered basic information on kindergarten children including their birth dates and addresses. All of these children were attending the kindergartens operated under governmental supervision. The enrolled children represented 10.1% of the total same age group of children who lived in Seoul. The test kit comprised instructions, a picture card, and an answer sheet. Parents were instructed to perform the test under bright light at a distance of 3 m and to use tissue paper and plastic tape to patch alternately the eye not being tested. The instructions included demonstration photos of vision testing which the parents were to follow. The picture card consisted of the following five familiar images; a fish, butterfly, airplane, duck, and car (fig 1). These figures were designed to correspond to a visual acuity (VA) measurement of 0.5 at 3 m. The picture card was cut into five pieces, and the child was shown the figures one at a time. A child who was able to identify three of the five figures correctly was considered to have a VA of 0.5 or better, which we considered normal for this age group. In addition, parents were asked to fill in the enclosed questionnaire concerning abnormal ocular behaviours such as a squint, photophobia, or eyelid drooping. Each parent was encouraged to perform the whole process of the home vision test properly and completely and then asked to bring the answer sheet to their child’s kindergarten.
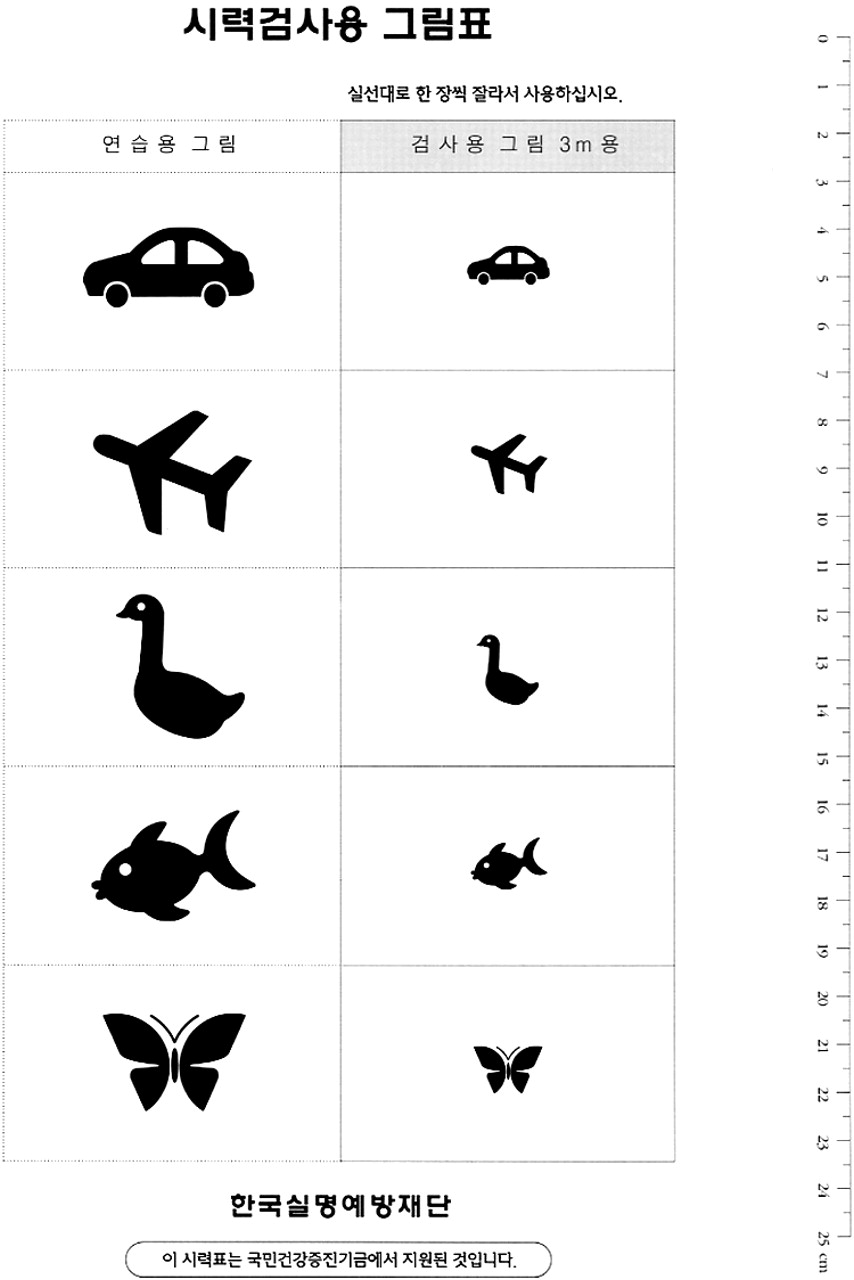
A set of five picture cards used in the home vision test. The figures in the left side column are for exercise and those in the right side column are for the test.
Children with VA less than 0.5 in either eye or any abnormal behaviours on the questionnaire were scheduled for retesting in the public healthcare centres (PHCs) as the second step of this vision screening programme. Visual acuity retesting was performed by nurses at each regional PHC using Jin’s vision chart at a distance of 4 m. The nurses were pretrained by some of authors to perform vision testing, corneal reflex test, and history taking. Jin’s vision chart (JV Institute, Seoul, Korea, www.jvinstitute.net) is one of the commercially available regular VA charts that use logarithmic progression, and was recently made according to the standards provided by the International Organization for Standardization (ISO) and the American National Standards Institute (ANSI) (fig 2). The chart has been widely adopted for clinical use in South Korea. On the basis of this vision retesting, children who had VA of less than 0.5 at the age of 3 years, VA of less than 0.63 at the age of 4 or 5 years in either eye or who had two or more lines’ difference between the eyes were referred to eye clinics. Other referral criteria were history of suspected ocular misalignment and other ocular diseases.

{kind=link}
{kind=link}
Jin’s vision chart used at the step of retest. This chart consists of 11 lines based on the progression of LogMAR from 0 to 1.0. Visual acuity was expressed as a decimal notation.
At the eye clinics, routine ophthalmological evaluation was performed, including monocular VA testing, retinoscopy under cycloplegia (cyclopentolate 1% and tropicamide 1%), prism cover test at distant and near fixation, ocular motility testing, and examination of the ocular media and fundus. Prism cover tests were performed with full optical correction if there was a significant refractive error. Refractive error was defined as hyperopia ⩾2 diopters (D), myopia ⩾1 D, and astigmatism ⩾1 D. Anisometropia was defined as a difference in refraction between the eyes of ⩾1 D spherical or ⩾1.5 D cylinder.
After the standard diagnostic investigation, the ophthalmologists were supposed to fill out the report form and provide it to the Korean Foundation for Prevention of Blindness (KFPB). The KFPB, which is the administrative centre of this preschool vision screening programme, collected and analysed all feedback reports sent by the ophthalmologists.
RESULTS
Of the 36 973 children enrolled in the first step of this screening programme, 35 894 children (97.1%) returned the results of the home vision test. Of these 35 894 children, 35 226 (98.1%) were able to complete the test. Of these 35 226 children, 7116 (20.2%) failed the home prescreening test and were scheduled for the second step retesting. Among them, 878 children failed in the home vision test and the rest (6238 children) failed in the questionnaire study only. Actually, more than 7116 children were presented to PHCs mainly due to the parents’ over concern about their children’s eye status. The extra numbers who did not meet our criteria were not included in this study. On vision retesting in PHCs, 2058 (28.9%) of the 7116 children did not pass our vision criteria and were scheduled for a referral. However, only 1372 (66.6%) of the 2058 children visited eye clinics. Of those 1372 referred children, feedback reports for 894 children (65.2%) were collected by the KFPB. The data for this demographic setting are shown in table 1.
Overall population data for the children screened
Regarding the home vision test using picture cards, 34 348 (97.5%) children passed the test. Only 878 (2.5%) children had VA of less than 0.5 in either eye as is shown in table 2. Regarding the questionnaire evaluation, 6238 children (17.7%) had one or more abnormal behavioural signs. We also found that 72.8% of all children had never taken any kind of VA test before. The overall response to the questionnaire is shown in table 3. The rate of positive answers to question 4, which signalled an abnormality (holding objects close to the eye), was the highest (20.1%), and the positive answer rates of question 7 (frequent blinking or eye rubbing) and question 2 (closing one eye in the sun or extreme light sensitivity) were 7.9%, and 7.8%, respectively.
Results of home vision test in the right eye according to the age
Results of the questionnaire study
The final diagnoses upon referral are listed in table 4. Significant refractive errors were found in 608 children. The distribution of the refractive errors is listed in table 5. Manifest strabismus was reported in 52 children, in whom exotropia was about three times as common as esotropia. Amblyopia was detected in 149 children (0.42% of those screened) and the causes were: ametropia 48.3%, anisometropia 34.2%, strabismus 12.8%, and unclassified 4.7%. In the group of external and anterior segment abnormalities, epiblepharon with trichiasis was detected in 42 children, conjunctivitis in 19, keratitis in eight, bilateral congenital cataract in one child, and ptosis in three children. Another three children had fundus abnormalities: optic nerve hypoplasia (two children) and choroidal coloboma (one child). Table 6 shows a breakdown of ophthalmological abnormalities by each disease category and this illustrates how we handled the data if two or more diseases were coexistent.
Ophthalmological abnormalities diagnosed on the referral examinations
Distribution of refractive errors
Breakdown of ophthalmological abnormalities by each disease category and the final effect of this screening programme
Of those who were found to have any ophthalmological abnormalities (685 children), 395 children (57.7%) failed the home vision test and the remaining 290 children (42.3%) passed the test. Of those who failed the home vision test (878 children), 838 children did not pass the retest in PHCs. Among them, finally, 395 children (45.0%) were found to have one or more ophthalmological abnormality. Meanwhile, of those who failed only on the questionnaire study (6238 children), 290 children (4.6%) were proved to have one or more ophthalmological abnormality. The other detailed data regarding the results of home vision test and the questionnaire study are listed in table 7.
Results of the home vision test and the questionnaire study through the whole process of the screening
Regarding the questionnaire study, we investigated further whether some of the questions actually correlated with ocular abnormalities. Of those who gave positive answers to question 4 (6773 children), 541 (8.0%) were found to have refractive errors on referral examinations and these numbers corresponded to 89.0% of all children with refractive errors. The frequency of positive answers to the question 1 was 911. Of those, only 39 children (4.3%) were diagnosed as strabismus. However, these numbers corresponded to 75.0% of all children with strabismus. Of those who gave positive answers to question 7 (2516 children), 477 (19.0%) had refractive errors and these corresponded to 78.5% of all children with refractive errors. Interestingly, of those who showed three or more positive answers to the questionnaire (609 children), 254 children (41.7%) were found to have one or more ophthalmological abnormalities on referral examination.
The final effect of this screening programme, as shown in table 6, was that spectacles were prescribed for 394 children, 35 children needed to be scheduled for surgery, 256 children were recommended for regular check ups, and no pathologic findings were noted in another 209 children. So the positive predictive value (PPV) of vision screening, followed by a referral for any ophthalmological disorder was 0.77 (number of children who had any ophthalmological disorder (685)/number of total referred children (894)); for significant ophthalmological disorders requiring treatment was 0.49 (number of children who were prescribed spectacles and were scheduled for surgery (429)/number of total referred children (894)), and for amblyopia was 0.17 (number of children who had amblyopia (149)/number of total referred children (894)).
DISCUSSION
In Korea, preschool vision screening has not yet been mandated as one of the national healthcare programmes, although this study was sponsored by the Ministry of Health and Welfare. We had to use the limited resources of the healthcare system and develop an appropriate screening method that could be easily administered for a relatively low cost and that could be performed efficiently in our situation. Therefore, we employed a new model of preschool vision screening. We combined a home vision screening test (as a prescreening step) and PHC retesting in a stepwise manner. For the home vision screening, picture cards were used for the VA test. Even though picture cards may lack the scientific validity of Landolt rings, a home screening test cannot be performed unless young children cooperate. Over 98% of the children completed the test and ultimately 149 cases of previously undetected amblyopia (0.42% of those screened) were found, which indicated that this home vision test might be a satisfactory screening tool for this age group.
Picture tests or single optotype tests of VA, such as used in this study, cannot detect every child with amblyopia.9 We therefore added the questionnaire study regarding eye conditions to the home vision screening step. Children who had abnormal ocular symptoms or behaviours on the questionnaire study were included in the PHC retesting group. This was necessary to minimise the risk of amblyopic children being missed by our home vision test using single optotype picture cards. The picture VA tests alone selected only 3% of all screened children, while the questionnaire study identified an additional 17%. Using home vision prescreening the retesting subgroup, which was expected to be a more selective and high risk subpopulation, could be created. Consequently, more selective screening was possible. The subgroup of retested children was checked with regular linear optotypes vision charts having crowding effect.
The questionnaire study was a unique part of our screening methodology. We think that this was helpful to draw more attention from the parents and more active participation in the whole process of this test, especially as this preschool vision screening has not yet been mandated. A voluntary action of filling out the questionnaire and bringing the answer sheet seemed to contribute to increase the participation rate and to create a positive attitude to this test.
As shown in table 7, the PPV of the questionnaire study, which indicated the ratio of the number of children who had any ophthalmological disorder to the number of children who failed in the questionnaire study and passed the home vision test, was very low (4.6%). However, 290 children screened by questionnaire study formed 42.3% of all children with ophthalmological abnormalities. Thus the questionnaire study in our screening test did not seem to be highly efficient in terms of PPV but helpful in detecting potential visual disorders.
The PPV of the home vision test was relatively high. Three hundred and ninety eight children (45.0%) of 878 children who initially failed in the home vision test were finally proved to have any ophthalmological disorders through the whole process of this screening test. Even though most screened children passed the home vision test, those who failed showed a strong tendency to also fail in retest in PHCs and the number of those who had abnormalities among them was 395, which formed 57.7% of all those who had ophthalmological abnormalities. We conclude that the home vision test took a primary role in detecting serious ophthalmological disorders in preschoolers and the questionnaire study played an adjunctive role in our study.
There are some potential limitations of our study. Firstly, in our home vision prescreening step, the same vision criteria were applied to different age groups. Although VA of 0.5 was reasonable normal vision for 3 year old children, it might be a relatively low threshold for 4 or 5 year old children. Because the aim of any screening test is to have as few false negatives as possible, we considered it necessary to try to raise our present visual threshold for 4 or 5 year old children from 0.5 to 0.63. The idea of raising the visual threshold was also supported by the fact that only a small percentage of children (less than 3% of those screened) could not pass the home vision test. Of course, in the future, we will have to take into account additional numbers and costs. Secondly, whereas the screening had a high participation rate, the ophthalmologists’ participation rate was relatively low. The rate of feedback reported by ophthalmologists on referral examinations was only 65.2%. The importance of thorough examinations and conscientious medical reports in the screening study should have been stressed further to every practising ophthalmologist. Thirdly, ocular alignment was not assessed in this screening model. Considering our current situation, cover and uncover test could not be performed at the step of prescreening and the retest in PHCs. This explains the relatively low frequency of strabismus (0.15%) in our study. In the near future, however, we think that a stereopsis test, like Lang card test, can be incorporated into our retesting step in the PHCs. Fourthly, in our screening results, visually minor problems, such as epiblepharon and conjunctivitis were included in the ophthalmological abnormalities. It is possible that the visually insignificant eyelid and conjunctival disorders might raise the PPV of the screening test. Although some cases of these had significant refractive errors at the same time, careful consideration was needed. We therefore calculated an additional PPV of 0.49 for significant ophthalmological abnormalities requiring treatment.
There are, however, missing rates in this screening process that are somewhat high. Six hundred and eighty six children (33.3%) of those who were scheduled for a referral did not visit an eye clinic. Of these 686 children, on further investigation, 576 (84.0%) had been checked at an eye clinic and were told their ocular status by an ophthalmologist. Among them, moreover, 439 children (76.2%) were currently or previously under treatment such as wearing spectacles, occlusion treatment for amblyopia, or strabismus surgery. Therefore, we have to state that our vision screening study seemed to be meaningful and efficient in detecting “new” cases with ocular abnormalities. Also, the non-report rate of 34.8% from the ophthalmologists who examined the referred children was not negligible. In phone interviews with each ophthalmologist where possible, we noticed that the main reason they did not report the results of standard ophthalmological examination was the referred children’s relatively normal or insignificant ocular health conditions. This explains why the non-report rate in those who passed in the home vision test and failed in the questionnaire study is relatively high (50.2%) whereas the rate in those who failed in both the home vision test and the questionnaire study is much lower (1.6%), as depicted in table 7. The other reasons why some ophthalmologists did not report included a lack of understanding of this whole screening process and inconvenience in our reporting system, which depended the ophthalmologist’s own willingness.
The present study was performed to substantiate the call for mandatory preschool vision screening in South Korea. With limited public healthcare personnel and resources, we attempted to find a better screening protocol and to standardise the preschool vision screening model. Our evaluation shows that our screening strategy achieved a relatively high screening yield in terms of positive predictive value (0.77 and 0.49).
All screening strategies have their own two characteristics: false positives and false negatives, in other words, sensitivity and specificity.10–12 An ideal screening method would be a highly sensitive and highly specific test that had a high positive predictive value and a very low negative predictive value.13–15 As there is, at present, no absolutely perfect “supertest”, researchers might emphasise either of these characteristics of a screening programme.10 We chose and emphasised the aspect of high sensitivity by using easily testable methodology in spite of expected high false positives. Considering the current paediatric vision screening situation in South Korea, our study shows that this model of preschool vision screening may be an effective and highly productive one.
However, as we also recognised some flaws and limitations throughout the screening process, our Seoul Metropolitan Preschool Vision Screening Programme needs to be optimised with further revision. The detail of the revision will include raising the visual threshold of the home vision test, a more specific and sophisticated questionnaire study, higher rates of eye clinic visits of those who were scheduled for a referral, higher rates of feedback reports from the ophthalmologists, and the incorporation of stereopsis test into the step of retest.
Amblyopia and strabismus are treatable causes of decreased visual function and are the unfortunate causes of permanent vision loss. Although screening cannot reduce the incidence of these disorders, it can certainly reduce the incidence of visual impairment caused by them. The high frequencies of ocular disorders newly detected in this demographic setting attests to the importance of performing early and effective screening eye examinations in children.