Article Text

Abstract
Aim: To identify predisposing factors and to define clinical and microbiological characteristics of bacterial keratitis in current practice.
Methods: A retrospective analysis of the hospital records of patients presenting with bacterial keratitis and treated at the Quinze-Vingts National Center of Ophthalmology, Paris, France, was performed during a 20 month period. A bacterial keratitis was defined as a suppurative corneal infiltrate and overlying epithelial defect associated with presence of bacteria on corneal scraping and/or that was cured with antibiotic therapy. Risk factors, clinical and microbiological data were collected.
Results: 300 cases (291 patients) of presumed bacterial keratitis were included. Potential predisposing factors, usually multiple, were identified in 90.6% of cases. Contact lens wear was the main risk factor (50.3%). Trauma or a history of keratopathy was found in 15% and 21% of cases, respectively. An organism was identified in 201 eyes (68%). 83% of the infections involved Gram positive bacteria, 17% involved Gram negative bacteria, and 2% were polymicrobial. Gram negative bacteria were associated with severe anterior chamber inflammation (p=0.004), as well as greater surface of infiltrates (p=0.01). 99% of ulcers resolved with treatment, but only 60% of patients had visual acuity better than the level at admission, and 5% had very poor visual outcome.
Conclusions: Contact lens wear is the most important risk factor. Most community acquired bacterial ulcers resolve with appropriate treatment.
- bacterial keratitis
- contact lens
- cornea
- ulcer
Statistics from Altmetric.com
Bacterial keratitis is a serious ocular infectious disease that can lead to severe visual disability.1 The severity of the corneal infection usually depends on the underlying condition of the cornea and the pathogenicity of the infecting bacteria. Many patients have a poor clinical outcome if aggressive and appropriate therapy is not promptly initiated.2–4
Bacterial keratitis is rare in the absence of predisposing factors.5,6 Until recently, most cases of bacterial keratitis were associated with ocular trauma or ocular surface diseases. However, the widespread use of contact lenses has dramatically increased the incidence of contact lens related keratitis.7–9 The spectrum of bacterial keratitis can also be influenced by geographic and climatic factors. Many differences in keratitis profile have been noted between populations living in rural or in city areas, in western, or in developing countries.4,9–12
In recent years the literature extensively addressed this issue but only a few publications reviewed large series of patients with bacterial keratitis.6,13,14 Very little information is available on the frequency of factors predisposing to bacterial keratitis and on the demographic characteristics of those patients. The aim of the study was to identify predisposing factors and to define clinical and microbiological characteristics of bacterial keratitis in our current practice. We report a retrospective study to evaluate a large population of patients with bacterial keratitis. The influence of demographic, medical, and ocular factors noted at presentation were reviewed.
PATIENTS AND METHODS
We reviewed the charts of all patients with bacterial keratitis who were treated in our hospital during the period January 1998 to September 1999. A bacterial keratitis was defined as a suppurative corneal infiltrate and overlying epithelial defect associated with presence of bacteria on corneal scraping and/or that was cured with antibiotics. Patients suspected of having or with a positive culture for fungal, viral, or acanthamoeba infection were excluded.
The following data were collected from each chart: patient age and sex, and duration of the symptoms at the time of the presentation. History and examination were focused on the following risk factors: corneal trauma, contact lens wear, ocular surface diseases (that is, previous herpetic infection, bullous keratopathy, dry eye syndrome, blepharitis, or other eyelid abnormalities), corneal surgery (refractive surgery, penetrating keratoplasty). There were eight cases in which contact lens wear was associated to ocular surface disease. Those cases were classified as ocular surface diseases. The size of the infiltrate was measured in square millimetres and its location was determined according to five zones: central, nasal superior, nasal inferior, temporal superior, and temporal inferior. The ulceration depth was evaluated as <⅓, ⅓–⅔, and >⅔ of the total corneal thickness. Anterior chamber inflammation, when present, was scored from 1 to 4 + for Tyndall effect and cells. We recorded the antibiotics and other treatments that were administered before examination.
All suspected infectious corneal infiltrates and ulcers were scraped for microbial culture and sensitivity studies before treatment was initiated or changed. A corneal smear was taken after topical anaesthesia. Two slides were done for the direct microscopic examination with spatula. The stainings that we used were May Grünwald Giemsa (MGG) on one slide, Gram, periodic acid Schiff (PAS) or acridine orange for the second slide (depending on the MGG results or if acanthamoeba infection was suspected). The results of the stainings were transmitted to the clinician if they provided an aetiological diagnosis or if specific appropriate therapy had to be initiated before the culture results were available. Inoculation of agar culture plates (chocolate polyvitex agar, Schaedler broth with globular extract, Portagerm-Amies agar swab (Biomérieux, France) and Sabouraud-chloramphenicol-gentamicin medium) was performed with cotton swab applicators. The chocolate polyvitex agar was incubated in an atmosphere containing 3% carbon dioxide, and all media were incubated at 37°C, excepted Sabouraud medium, which was incubated the first night at 37°C and then at 30°C. The media were examined every day, during 1 week for the chocolate polyvitex agar, 2 weeks for Sabouraud-chloramphenicol-gentamicin agar, and 1 month for the Schaedler broth. The bacteria were identified using standard methods: Gram staining, BBL crystal (Becton Dickinson), and/or Api (Biomerieux) strips, biochemical tests. A single colony of a virulent organism or at least three colonies of an organism that usually is not considered to be highly pathogenic on the ocular surface (such as coagulase negative staphylococcus) were considered to be positive cultures. The resistance to antibiotics was evaluated with the standard disc diffusion method and interpreted according to the guidelines established by the National Committee on Clinical Laboratory Standards (Villanova, PA, USA). Contact lenses and storage cases were also analysed.
The decision to admit patients and the use of fortified antibiotics were influenced by the severity of the keratitis, based on an overall clinical impression and the ability of the patient to instill antibiotic eye drops. The standard fortified antibiotherapy consisted of topical ticarcillin (6 mg/ml), gentamicin (20 mg/ml), and vancomycin (50 mg/ml), whereas commercially available antibiotics used were topical fluoroquinolone (ofloxacin or ciprofloxacin) either alone or in combination with aminoglycosides. Eye drops were administered alternatively every 15 minutes during the first 2 hours, then every hour for the following 48 hours. The treatment was progressively tapered and/or modified according to the clinical response and the bacteria susceptibility.
Outpatient charts were consulted to determine visual acuity in the affected eye at last visit and to identify patients who subsequently underwent penetrating keratoplasty. Patients were considered to have a “good” clinical outcome when corneal healing was not associated with a visual loss (visual acuity better than the level of initial examination), “poor” outcome if they had one to three lines loss of visual acuity, “very poor” outcome if visual loss was superior to four lines or if a major complication occurred, or if they underwent penetrating keratoplasty.
Univariate analysis was used to evaluate the possible associations between bacterial types, clinical characteristics, risk factors, and clinical outcomes. χ2 Test and Wilcoxon rank sum test were used for univariate study. The variable lists were reduced to those with p value less than 0.1 in the regression analysis. Multivariate study was performed with logistic regression model in order to predict the occurrence of “very poor” visual outcome. spss software (V11.0) for Windows was used for statistical analysis.
RESULTS
Clinical characteristics
A total of 291 patients (300 eyes) were seen with a corneal infiltrate that was compatible with a diagnosis of bacterial keratitis during the study period of 20 months; 228 eyes (76%) were examined for the first time in the emergency department of our hospital whereas 72 (24%) were referred by general practitioners or ophthalmologists, most of whom practise in Paris area, and were already being treated with topical antibiotics: fluoroquinolones (27 cases), aminoglycosides (18 cases), rifamycin (11 cases). Nine patients were treated with corticosteroid eye drops. Self medication with topical anaesthetics were noted in three cases.
The age of the patients ranged from 6 months to 94 years (mean age 39 years). Sex distribution was close to 1:1 (152 men and 139 women). Most of patients were living in urban areas. No significant difference in risk factors was noted between patients living in rural or urban areas.
Predisposing factors of bacterial keratitis are summarised in Table 1.
Frequency of predisposing ocular conditions in bacterial keratitis
Contact lens (CL) wear was the most common risk factor. This was encountered in 151 eyes (50.3%). Soft CL were noted in 89.4% of cases, rigid gas permeable CL in 8.6%, and hard PMMA CL in 2% of cases. Mean age of the patients with CL related microbial keratitis was 32 years and the mean delay between the onset of the symptoms and the first examination was 48 hours in this group.
Ocular surface diseases were present in 21% of cases and acute corneal trauma (abrasion, laceration, penetration) in 15% of cases. Among keratopathies, herpes was present in 12 cases, bullous keratopathy in 10 cases, and exposure keratopathy in six cases. Mean age of the patients with ocular surface diseases was 56 years. In this group, the delay between the onset of the symptoms and the first examination was 7 days. No risk factors were identified in 9.4% of cases. Systemic risk factors were diabetes mellitus (seven cases), immunosuppressive treatment (six cases), psychiatric disorders (two cases), and allergy (two cases). There was no significant correlation between systemic risk factors and severity of clinical presentation.
Keratitis involved the right eye in 45.7% (137) of cases, and the left eye in 54.3% (163) of cases. Infection was bilateral in nine patients (3%).
Visual acuity on presentation ranged from 20/20 to no light perception. Mean visual acuity was 0.51 (SD 0.4).
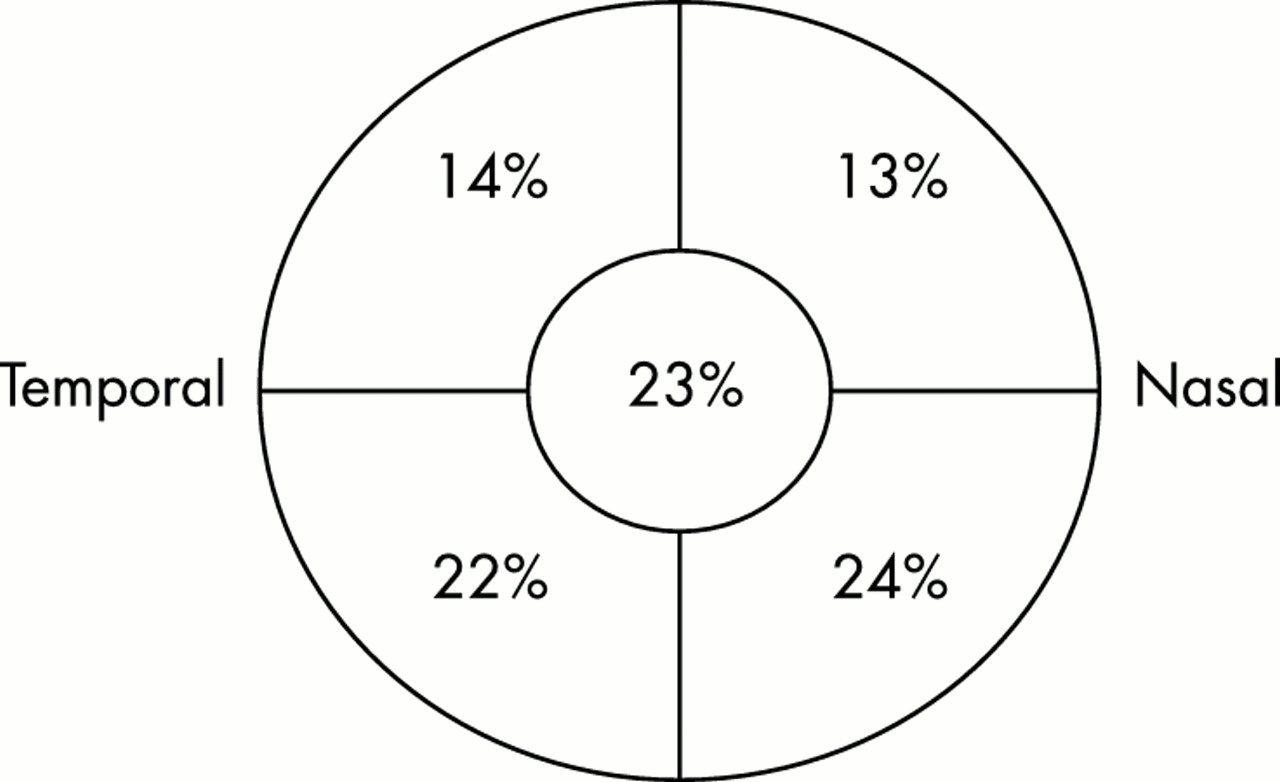
The location of the infiltrates was distributed as shown in Figure 1. There was a predominance of inferior localisations (46%). Corneal infiltrates were unique in 251 eyes (82%) and multiple in 49 (18%).
{kind=link}
Location of the principal corneal infiltrate. Inferior, nasal, and temporal locations were the most frequently observed; 4% of the infiltrates were diffuse.
The infiltrate surface was less than 5 mm2 in 123 eyes (41%), 5–15 mm2 in 115 (38.3%), and greater than 15 mm2 in 62 (20.7%).
The infiltrate depth was less than one third in 232 eyes (77.2%), between one third and two thirds in 39 (13.1%), and over two thirds in 29 (9.7%).
Anterior chamber inflammation was absent in 75.6% of cases. A 1+ to 2+ Tyndall effect was present in 16.6% of cases, whereas severe anterior chamber inflammation (3+ to 4+) and hypopyon were present in 1.7 and 6.1% of cases, respectively. Corneal neovascularisation was observed in 35 eyes (11.7%).
Two patients had corneal perforation.
Microbiological characteristics
In 207 eyes (68.2%), bacteria were identified from the corneal cultures. In patients in whom antibiotic therapy had been initiated before examination (73 eyes), our hospital culture grew an identifiable organism in 58% of cases. The bacterial spectrum is shown in Table 2. Gram positive bacteria were predominant (83% of all positive cultures), mainly coagulase negative Staphylococcus species; Gram negative bacteria (17%) were mostly Pseudomonas and Serratia species. Polybacterial infection was noted in six cases (2%). Twenty eight per cent of culture positive isolates were detected on smears.
Organisms isolated in bacterial corneal ulcers. Polybacterial infection was noted in 6 cases
In CL wearers group, 63.3% of the corneal scrapings were positive. Thirty per cent of isolated bacteria were Gram negative, mostly Pseudomonas aeruginosa. Contact lens and/or storage cases cultures were performed in 67 cases (Table 3). An organism was identified in 83.6% (56) of cases. Ninety seven per cent of the organisms were Gram negative bacteria. The bacteria isolated were similar to the organism recovered by corneal scraping in 14 cases.
Contact lenses bacteriological study
The percentage of Gram positive bacteria was 91% in the ocular surface disease group and 100% in the corneal trauma group.
Gram negative bacteria were associated with severe anterior chamber inflammation (p=0.004), as well as greater surface of infiltrates (p=0.01). No other correlations were found between the type of bacteria and other clinical characteristics recorded at the time of presentation.
Treatment and clinical outcome
Outpatient treatment had been initiated in 227 of the 300 cases (75.7%). Initial therapy consisted of antibiotics without corticosteroids in all the cases. It was based on patient history, clinical features, bacteria identification. Fortified antibiotics (combination of ticarcillin, gentamicin, and vancomycin) were used in 213 cases (71%) whereas commercially available antibiotics (fluoroquinolone monotherapy or combination with tobramycin and/or rifamycin) were administered in 29% of cases. The mean duration of hospital stay was 9 days (range 3–60 days). Complications of bacterial keratitis were noted in 18 eyes (6%). Among them, there were nine endothelitis, two endophthalmitis, five posterior synechias, one hyphaema, one severe ocular hypertony. Complications were mostly associated with previous history of keratopathy (eight eyes), corticosteroid initial treatment (five eyes), self medication with anaesthetics (three cases). Two eyes went on to penetrating keratoplasty and two eyes were enucleated.
Mean follow up was 2.5 months but 17% of the patients were followed no more than a week. Sixty per cent of patients had “good” visual outcome with visual acuity better than the level at admission. Among the others the final clinical outcome was “poor” in 35% and “very poor” in 5% as shown in Table 4.
Demographic, risk factors, clinical, and microbiological characteristics of 15 cases of bacterial keratitis with “very poor outcome”
Statistical analysis revealed that “very poor” visual outcome was significantly correlated with history of ocular surface disease (p<0.0001), history of systemic disease (p<0.001), diffuse, central, or inferior localisations of the infiltrate (p<0.001), severe anterior chamber inflammation (p<0.001), and depth of the infiltrate (p<0.001). There was no correlation between visual outcome and contact lens wear, history of corneal trauma or surgery, number of localisations, and type of bacteria.
The selection procedure of the logistic model retained several variables (surface, stromal depth, presence of corneal new vessels, presence of anterior chamber inflammation) associated with unfavourable outcome. Among them, surface of the infiltrate (p=0.0001) and depth of extension (p=0.003) were the two most important factor to predict “very poor” visual outcome.
DISCUSSION
The current study applied to the general population with bacterial keratitis that presents with a relative broad spectrum of severity as seen in a large ophthalmic centre, including primary, secondary, and tertiary patient care. However, caution is necessary in the interpretation of this study. We did not see those cases of bacterial keratitis that respond promptly to treatment and therefore have no need for referral. We should also acknowledge that the epidemiology of bacterial keratitis reported in this study is specific to the city and the area of Paris, France.
The age profile in our patients is comparable with previous reports.6,14,15 Bimodality in the patients’ age distribution can be attributed to CL related keratitis, corneal traumas in the younger group, and predisposing ocular surface diseases, eyelid diseases in the older group. Bacterial keratitis is rare in the absence of a predisposing factor.
Our series showed that more than 50% of the bacterial keratitis were CL related keratitis. Nevertheless, some cases might include sterile infiltrates such as contact lens related inflammatory infiltrate that improves with discontinuation of contact lens wear. This proportion of CL related infections is more important than the percentages observed in other large series in which about 20–30% of infectious keratitis were associated with contact lens use.13,14
There has been in the past several years a steady increase in CL wearers.8 Subsequently, CL wear is now the major predisposing factor for corneal infection in the United States and Western Europe9,16,17 and a matter of public health concern. Soft CL have greatly increased the risk of bacterial keratitis, which is estimated to be 10–20 times higher with the use of extended wear disposable CL.8 Many physiopathological effects of CL wear have been reported, the most important of which is an induced hypoxia and hypercapnia of the cornea.18
History of ocular surface diseases represents the second most common cause of bacterial keratitis, accounting for 21% of cases. The association of bacterial keratitis with compromised corneas is common, but it also introduces the possibility of eye drop contamination during long term use and microbial resistance resulting from antibiotic use.19 Moreover, we observed that these patients suffering chronic symptoms had delayed referral. This situation is very often associated with very poor visual outcome. This issue was raised previously by Musch et al,6 who demonstrated that infectious ulcer patients with a history of previous ocular surgery, and pre-existing ocular pathology may be in a higher risk group for poor visual outcome.
Acute corneal trauma was present in 15% of cases. Ocular trauma was the most prevalent predisposing factor in young patients in the 1980s.6 However, recent studies showed a decrease of corneal ulcers following traumas,13,14 which is a far more common predisposing factor in rural areas or low income countries4 were it accounts for up to 77.5% of cases.
Our culture positive rate was 68% and is comparable with previous reports. However, we should point out that this rate might have been decreased by the application of topical anaesthetic before corneal scraping. The spectrum of micro-organisms that produce bacterial keratitis is usually most influenced by contact lens wear or pre-existing disease or injury of the cornea. The most common organisms cultured from bacterial ulcers were Staphylococcus, Streptococcus, Pseudomonas, and Serratia species. Coagulase negative staphylococcus was the most common organism isolated on corneal scrapings (21.8%). Currently, indigenous bacteria such as coagulase negative staphylococcus are increasingly being isolated in bacterial keratitis and have become the bacterial pathogen most responsible for infectious keratitis in our hospital. The same finding has been recently observed by Vajpayee in India,4 in Europe,9 and in the United States.2,3,20–22
Multiple organisms have been reported from the microbial keratitis seen in association with CL wear. We found a moderate shift towards higher prevalence of Gram negative rods compared with that prevalence in the absence of CL wear and we confirmed the results of previous studies.7,23 These results confirm that Gram negative bacteria are more often associated with soft CL wear.8 However, conversely to what might be expected, the percentage of Gram negative organisms is lower than those of Gram positive organisms. Approximately two thirds of CL related bacterial keratitis are associated with Gram positive cocci, such as staphylococci and streptococci and one third is associated with Gram negative rods, especially Pseudomonas aeruginosa, Serratia marcescens, and Serratia liquefaciens.
CL and/or storage cases cultures were positive in 83.6% of cases while corneal scraping was positive in 64.7% of CL wearers. However, the interpretation of these CL and case cultures is difficult since a recent survey showed that 81% of CL cases were contaminated—77% with bacteria, 24% with fungi, and 20% with protozoa.24 Furthermore, the bacteria isolated were similar to the organism recovered by corneal scraping in only 14 cases (25%). Cultures obtained from the contact lenses and the cases (rather than corneal scraping themselves) overwhelmingly yield Gram negative organisms, whereas corneal cultures do in fact produce a high proportion of Gram positive organisms. This result suggests that contact lenses and cases may tend to preferentially harbour Gram negative organisms, but that the causative organism may well not match that organism, and indeed Gram positive organisms are important in contact lens related keratitis.
Interestingly, we found that anterior chamber reaction associated Gram negative rods were more important compared to inflammation associated with Gram positive bacteria. This can be due to the higher pathogenicity of the Gram negative compared to Gram positive bacteria.
Not surprisingly, the severity of the presenting signs (surface and depth of the infiltrate, presence of corneal new vessels, presence of anterior chamber inflammation) were significantly related to bacterial keratitis outcome as already shown.3,11,25 On the other hand, the systemic risk factors (that is, diabetes mellitus, rheumatoid arthritis, immunodeficiency states) and history of ocular surface disease, which were reported as potential risk factors by some authors,6,26 were also found to be prognostic factors in our study. Conversely, CL wear was not associated with “very poor” clinical outcome.
More than three quarters of cases were treated initially on an outpatient basis. Because our hospital is an academic centre, all the patients have been managed traditionally using universal standards: pretreatment cultures and broad spectrum fortified antibiotics. Thus most patients (71%) have received combination therapy with fortified antibiotics, whereas broad spectrum antibiotic therapy with the fluoroquinolones was prescribed in the remaining cases. However, the proportion of severe ulcers, associated with complications and/or with very poor visual outcome, is relatively low (5%) and similar to other large series in which monotherapy with a fluoroquinolone antibiotic was compared to fortified antibiotics.5,11,22,27 These data should probably lead us to widen the use of fluoroquinolones5,11,22,27 even if the present study suggests that Gram positive organisms predominate in the setting of CL related keratitis. However, we believe that the emerging resistance of Gram positive organisms to second generation fluoroquinolones12,19 indicates the necessity to perform pretreatment cultures of corneal ulcers in all patients or to use third or fourth generation quinolones characterised by a superior Gram positive profile.
We reported the first substantive series of French patients with bacterial corneal ulcers. Although not a completely true representation of the population, our study does provide an insight into the spectrum of bacterial keratitis. Our results emphasise the importance of staphylococci as the major cause of corneal infection, and the need to increase public education about proper contact lens use.
REFERENCES
Linked Articles
- Editorial
- BJO at a glance