Article Text

Abstract
AIM The management of suppurative keratitis due to filamentous fungi presents severe problems in tropical countries. The aim was to demonstrate the efficacy of chlorhexidine 0.2% drops as an inexpensive antimicrobial agent, which could be widely distributed for fungal keratitis.
METHODS Successive patients presenting to the Chittagong Eye Institute and Training Complex with corneal ulcers were admitted to the trial when fungal hyphae had been seen on microscopy. They were randomised to drop treatment with chlorhexidine gluconate 0.2% or the standard local treatment natamycin 2.5%. The diameters, depths, and other features of the ulcers were measured and photographed at regular intervals. The outcome measures were healing at 21 days and presence or absence of toxicity. If there was not a favourable response at 5 days, “treatment failure” was recorded and the treatment was changed to one or more of three options, which included econazole 1% in the latter part of the trial.
RESULTS 71 patients were recruited to the trial, of which 35 were randomised to chlorhexidine and 36 to natamycin. One allocated to natamycin grew bacteria and therefore was excluded from the analysis. None of the severe ulcers was fully healed at 21 days of treatment, but three of those allocated to chlorhexidine eventually healed in times up to 60 days. Of the non-severe ulcers, 66.7% were healed at 21 days with chlorhexidine and 36.0% with natamycin, a relative efficacy (RE) of 1.85 (CL 1.01–3.39, p = 0.04). If those ulcers were excluded where fungi were seen in the scraping but did not grow on culture, the estimated efficacy ratio does not change but becomes less precise because of smaller numbers. Equal numbers ofAspergillus (22) andFusarium (22) were grown. TheAspergillus were the most resistant to either primary treatment.
CONCLUSIONS Chlorhexidine may have potential as an inexpensive topical agent for fungal keratitis and warrants further assessment as a first line treatment in situations where microbiological facilities and a range of antifungal agents are not available.
- fungal keratitis
- corneal ulcers
- chlorhexidine
- Bangladesh
Statistics from Altmetric.com
Ophthalmologists working in a humid tropical environment are aware of how serious the problems of corneal ulcers caused by fungi can be. Often the onset follows a minor injury to the cornea in an agricultural worker, progresses slowly, and may be treated with traditional remedies before the sufferer presents with an advanced ulcer at an eye clinic. A prolonged period of pain and time unable to work follows, which subsistence farmers can often not afford, ending in perforation of the cornea and evisceration or enucleation of the eye. The ophthalmologist frequently has no access to a microbiology laboratory, and specific antifungal drugs for the eye are not available.
The proportion of suppurative keratitis due to filamentous fungi is sometimes underestimated. In reports from Bangladesh this proportion has varied from 23%1 to 33%,236%,3 and 40%.4 In southern Florida, fungi accounted for 35% of isolates.5 In Accra, Ghana, it was found that fungi alone were responsible for 49% of positive cultures, and if mixed fungal and bacterial infections were included, fungi occurred in 56% of cultures.6 A wide range of species of fungi have been isolated. The commonest genera areAspergillus andFusarium. The subject of mycotic keratitis has been thoroughly reviewed by Thomas.7
In a search for stable, inexpensive antimicrobial agents which could perhaps be made widely available in tropical countries, we tested fungal isolates from Ghana and India against chlorhexidine, povidone-iodine, propamidine, polyhexamethylene biguanide (PHMB), and econazole by placing the drugs in wells punched in Sabouraud’s dextrose agar media in petri dishes.8 Propamidine and PHMB showed no activity against the majority of fungi. While econazole 1% proved effective against the greatest number of organisms, chlorhexidine, and povidone-iodine both showed good dose related responses in vitro. A small pilot study was then conducted in India. The ineffectiveness of povidone-iodine in the clinical situation was disappointing, while chlorhexidine was much superior in effectiveness to povidone-iodine and equivalent to econazole.8 A masked randomised trial of three concentrations of chlorhexidine gluconate compared with 5% natamycin (the standard treatment available in that part of India) showed that 0.2% chlorhexidine gave the best results, without any toxicity.9
The aim of the present study was to determine whether the optimal concentration of chlorhexidine gluconate, 0.2%, was as effective against fungal ulcers as the best treatment (natamycin 2.5%) normally available at the time in Bangladesh so that it can be used as an alternative when natamycin or other specific antifungal agents are not available. A randomised trial was conducted at the Eye Infirmary and Training Complex, Chittagong (EITC), where a reliable and efficient microbiological laboratory has been established.24Sufficient numbers of fungal corneal ulcers are seen each week so that a small clinical trial could be completed within a few months.
Methods
The ulcers of successive patients attending EITC, Chittagong, with suppurative keratitis were scraped for microscopy and culture, after the history had been taken and the visual acuity measured. The specimens were examined microscopically as a wet mount in 10% potassium hydroxide and as a heat fixed mount with Gram stain. It was necessary that fungal hyphal elements were observed for the patients to be recruited to the trial. Corneal scrapings were cultured at 28°C in Sabouraud’s dextrose agar (SDA), chocolate agar, and blood agar media. If there was no growth on the 14th day the cultures were discarded. The sensitivity tests for fungi were done by the well diffusion method, filling 7 mm wells punched in SDA in a plate with 0.2% chlorhexidine, 2.5% natamycin, and 1% econazole. The diameters of the zones of inhibition were taken and 7 mm subtracted.
Exclusion criteria were patients with only one eye; those with diabetes mellitus; those with polymicrobial infections; those who were unwilling to participate fully or attend for follow up; children under 1 year of age; and cases where the ulcer had already perforated. After informed consent had been taken, passport-type Polaroid photographs of each patient were taken for future identification and attached to the records.
There were two arms to the study, 0.2% chlorhexidine gluconate drops and 2.5% natamycin drops. Chlorhexidine gluconate 20% solution was supplied by Moorfields Eye Hospital, London, in an amber coloured glass bottle and stored at 4°C by the EITC laboratory in Chittagong. Small volumes of this solution were diluted with distilled, deionised, pyrogen-free water (kindly supplied by Glaxo Wellcome, Bangladesh) and placed in 10 ml high density polyethylene screw capped eye drop bottles. These were autoclaved at 115°C for 30 minutes, and inspected for any evidence of evaporation or change of colour; all were found to be satisfactory. These bottles were kept at room temperature until provided to the patients. Natamycin 2.5% was already available in the EITC as the standard treatment for fungal keratitis. The formulation of natamycin 2.5% suspension was natamycin 27.5 g; sodium hydroxide 1.2% solution 150 ml; hydrochloric acid 5% solution added to adjust pH to 6–7.0; benzalkonium chloride 1% 5.5 ml; distilled water to 1000 ml. Ten ml eye drop bottles were filled, sterilised by gamma radiation, and refrigerated for storage. The randomisation of individuals was computer generated in London, and the codes for the alternative treatments sealed in serially numbered opaque envelopes, which were opened in sequence by the research ophthalmologist as the trial progressed. It was not possible to mask the ophthalmologist or nurses to the medications because of their different appearances.
The scraped ulcer was measured in its greatest diameter with the slit-lamp beam height adjustment of a Haag–Streit-type slit lamp, and again at right angles to the first diameter. An initial close up photograph was taken. The depth of the ulcer was estimated in a narrow slit lamp beam viewed from a wide angle. The area of infiltration was expressed as a percentage of the area of the cornea. The presence or absence of deep lesions (posterior corneal abscess; endothelial plaque) was recorded and the risk of perforation assessed.
The eligible patients were admitted to hospital and treated with one drop half hourly for the first 3 hours, then 1 hourly for 2 days, 2 hourly for 5 days, and 3 hourly for 2 weeks—a total of 3 weeks’ treatment. Treatment was continued longer with chlorhexidine in three patients who were still showing evidence of improvement at 3 weeks. The drops were given during the waking hours (7 am–9 pm). The nurses maintained a log book for each application of the medicines.
Signs of a favourable response at 5 days were: (a) blunting of the margins of the ulcers, (b) improvement in signs of inflammation, (c) reduction in cellular infiltrate and oedema, (d) reduction in corneal epithelial defect, (e) signs of re-epithelialisation, (f) reduction in anterior chamber hypopyon if present, and (g) decreased complaint of pain by the patient. If there was no favourable response by 5 days, or clear cut signs of deterioration of the ulcer developed later, the trial drug was withdrawn, the code checked, and the ulcer managed with the best alternative treatment. The patient was classified as “treatment failure” at 21 days. Econazole 1% drops became available as a reserve medication only towards the end of this trial because of a failure in supply. Natamycin 5% drops and clotrimazole 1% ointment also became available in Bangladesh during the period of the trial and could be used as back up. The alternative treatment was with one or more of these agents, used consecutively or together.
The outcome measure was healing at 21 days of treatment. Secondary outcomes were evidence of a toxic effect on the cornea or conjunctiva by the antimicrobial agents or development of early cataract. “Healing” at 21 days meant that there was intact epithelium, with or without scar formation, but (i) no perforation, (ii) no anterior staphyloma, (iii) no adherent leucoma, (iv) no fluorescein staining, (v) no hypopyon, and (vi) improvement in vision, or vision no worse than baseline level.
The development of signs of toxicity was an additional indication for withdrawing the initial treatment, but this proved not to be necessary in this trial. Signs of toxicity were defined as (a) patient’s intolerance such as pain or burning sensation, (b) swelling of the eyelids, (c) increased conjunctival congestion and chemosis, (d) conjunctival staining with fluorescein, or (e) punctuate corneal erosions.
The eyes were examined daily while in hospital, and the findings were recorded on the second, fifth, and seventh day, and at 21 days. Further close up photographs of the corneal ulcers were taken on the fifth and seventh days and any time during the next 2 weeks. Each patient was given a discharge summary with the date on which he should come back to the hospital for review. Follow up travel costs were offered to all patients. A postcard was mailed 5–7 days before the due date as a reminder. If they failed to come after this, an ophthalmologist went to see some patients in their homes and the rest were brought to the hospital for follow up. In spite of all these efforts a few could not be seen and were considered as lost to follow up.
A sweep follow up was carried out of all the patients at a minimum of 6 months after discharge from hospital, so the time of this final assessment varied from 6 months to 1 year, depending on the time of presentation.
The results were expressed as efficacy (percentage with successful outcome) and as relative efficacy (RE), a ratio obtained by simply dividing the proportion of successful results with chlorhexidine by the percentage of successful results with natamycin (chlorhexidine/natamycin); 95% confidence limits were calculated for relative efficacy. Adjustment was made for the confounding effect of the following factors: age, sex, duration of ulcer, prior antibiotic treatment, severity of ulcer, ulcer area, depth of ulcer, degree of hypopyon, and degree of infiltrate. This was done through analysis of data stratified by levels of the confounders (one at a time), using the Mantel–Haenszel method. Adjusted estimates of the efficacy ratios with 95% confidence limits and p values were calculated.
The categories of the prognostic factors (potential confounders) are detailed in Table 1. Ulcers were categorised as severe when they had a diameter of 6 mm or more; when the ulcer involved more than one third of the corneal thickness; when the infiltration involved the deep one third; when there was scleral suppuration, or the possibility of perforation; and if there was a posterior corneal abscess or endothelial plaque.
Baseline characteristics of the two treatment groups
Results
The number of patients recruited to the trial was 71, of which one grew bacteria on culture and was therefore excluded from analysis as a mixed infection. Of the remainder, 35 were randomly allocated to the chlorhexidine 0.2% group and 35 to the natamycin 2.5% group (Fig 1). Twenty patients were classified as having severe ulcers, with little prospect of recovery (although three severe ulcers were in fact healed beyond 21 days by chlorhexidine 0.2%).
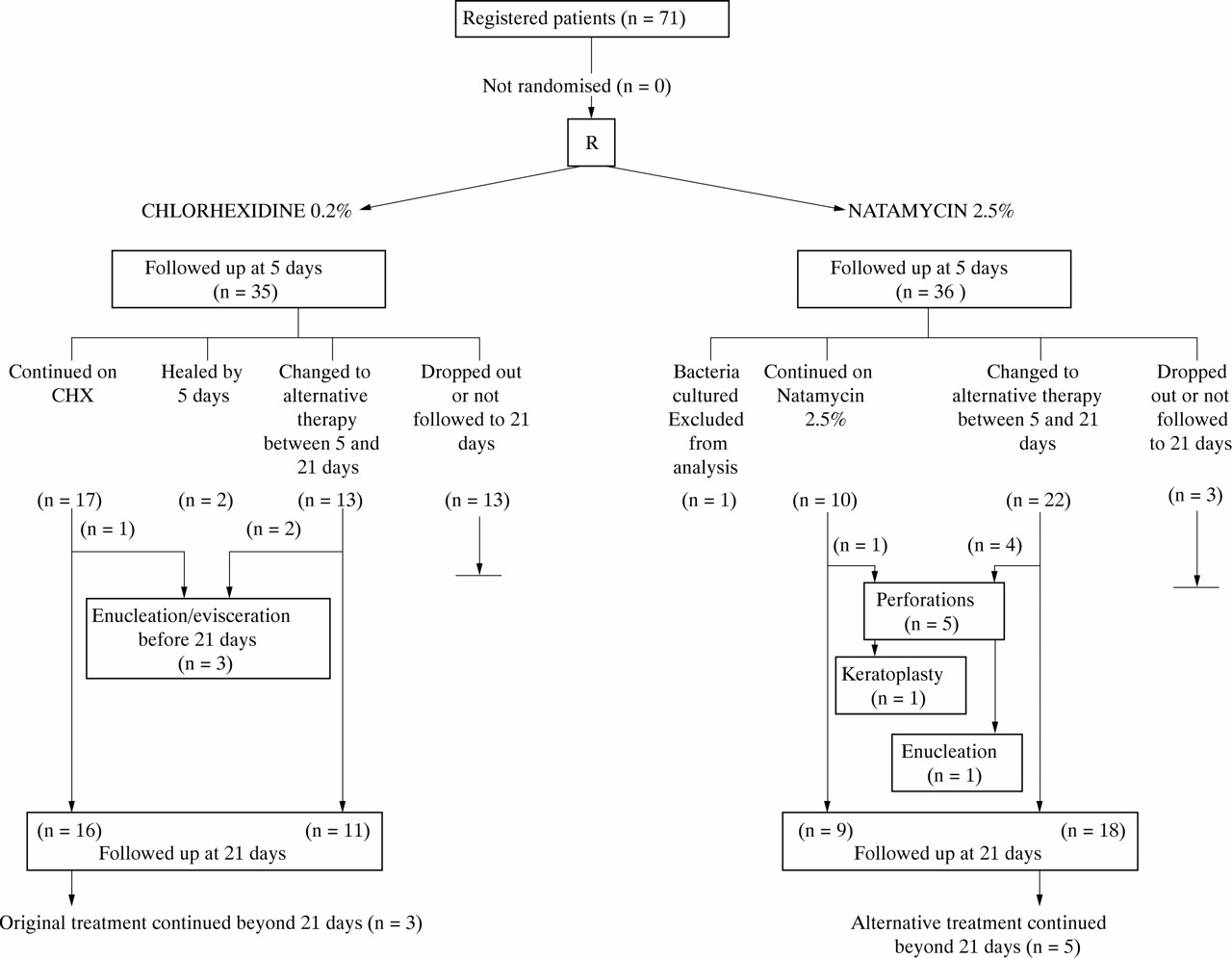
Flow of patients through the various stages of the trial.
The baseline characteristics of the patients and ulcers were compared in the two treatment groups as shown in Table 1. In the chlorhexidine group, three affected corneas had a posterior corneal abscess, and a further three had an endothelial plaque while none of the natamycin group had deep lesions. Twelve of the ulcers in the chlorhexidine group were classified as severe compared with eight in the natamycin group. Those with threat of perforation were nine and six respectively.
FAVOURABLE OUTCOME AT DAY 5 (TABLE 2)
At 5 days a significantly higher proportion in the chlorhexidine group showed a favourable outcome (31/35, 88.6% efficacy) and two were already healed compared with the favourable outcome in the natamycin group (18/35, 51.4%). The relative efficacy (RE) at this point was 1.72 with 95% confidence limits of 1.24–2.63 (p <0.001). The RE remained significant and close to 1.7 after adjustment for confounding effects of potential prognostic factors: age; sex; duration of ulcer before treatment; prior antibiotic treatment; severity of ulcer; depth of ulcer; degree of infiltrate; and degree of hypopyon.
Favourable outcome at day 5: comparison of the two treatments
When the ulcers were stratified into severe and non-severe, the superiority of chlorhexidine in treating the severe ulcers becomes apparent, with an RE of 7.33 at this stage. The original treatment was then continued in those with a favourable outcome at 5 days but if improvement was not maintained they were changed to alternative therapy at various times between 5 and 21 days (Fig 1).
HEALED BY DAY 21 (TABLE 3)
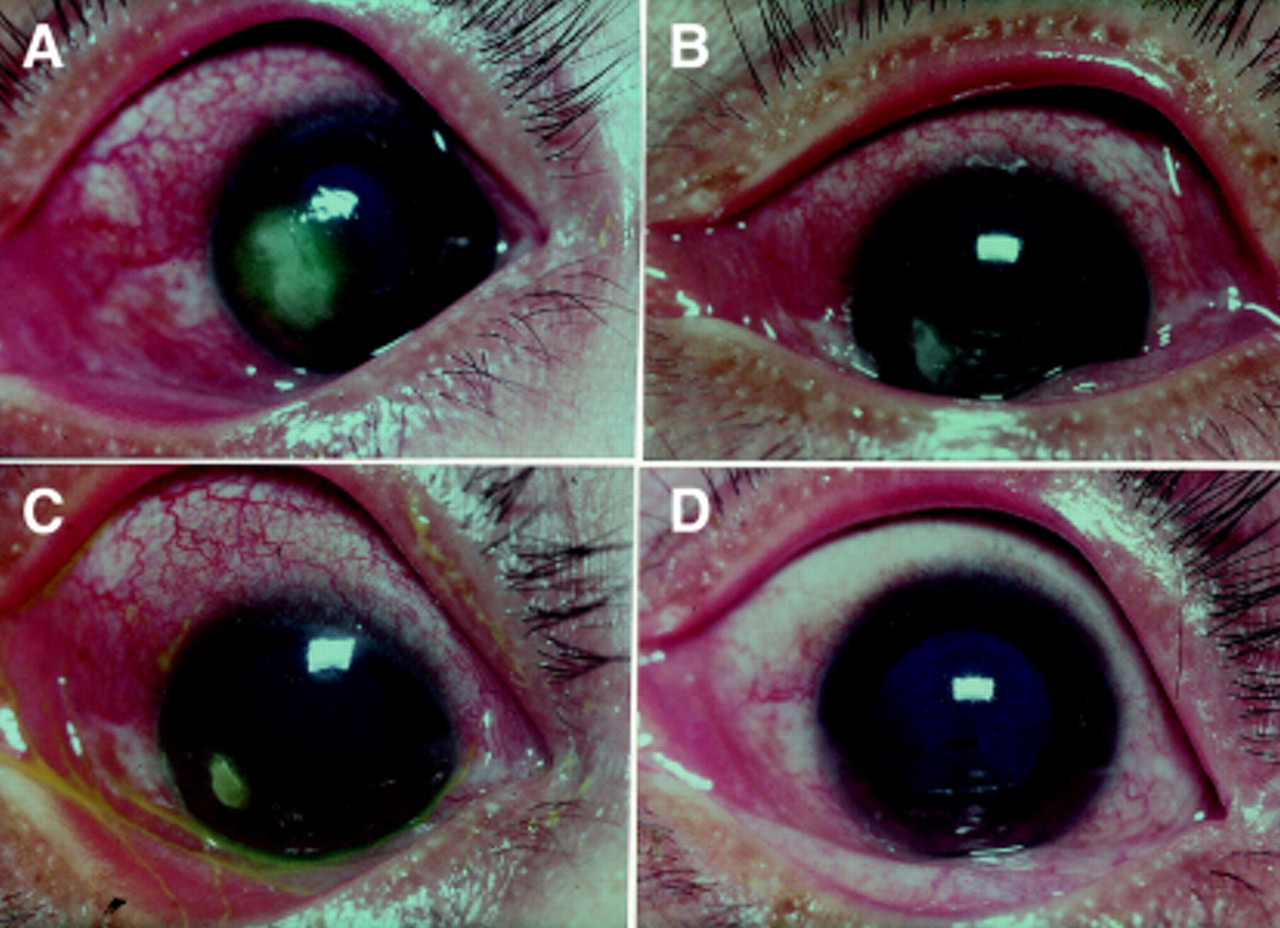
Three patients (one with severe ulcer) in each of the two treatment groups had incomplete follow up and could not be assessed at day 21. None of the severe ulcers healed by day 21 in either treatment group. In patients with non-severe ulcers, however, chlorhexidine seemed more effective than natamycin, the proportion of ulcers healed being 14/21 (66.7%) and 9/25 (36.0%) respectively, a RE of 1.85 (95% CL 1.01–3.39, p = 0.04) (Table 3A). When the results were restricted to those with positive cultures, the estimated efficacy ratio did not change, but became less precise because of smaller numbers: 1.85 (95% CL 0.87–3.93, p = 0.11) (Table 3B). Examples of stages of healing of ulcers caused by Fusarium and treated with chlorhexidine are given in Figures 2 and3.
Healing of ulcer by day 21 in 64 ulcers with positive microscopy: comparison of the two treatments

Serial photographs of healing of ulcer, classified as severe, by 0.2% chlorhexidine. Study no 25, 15 year old male student, secondary to injury with fingernail. Fungus identified was Fusarium sp. (A) At presentation, with hypopyon, (B) 5th day, (C) 7th day, (D) 10th day, residual epithelial defect. Fully healed on day 26.

{kind=link}
{kind=link}
{kind=link}
Serial photographs of healing of ulcer by 0.2% chlorhexidine. Study no 4, 45 year old female farmer, no history of injury. Fungus identified was Fusarium sp. (A) Ulcer at presentation, (B) fifth day, (C) 7th day. (D) Ulcer healed on 17th day.
Adjustment for confounding effects of other prognostic factors made little or no difference to the findings in either group.
The organisms isolated from the ulcers in the two treatment groups and their sensitivity in culture to the agents are listed in Table 4. No cultures were obtained on seven cases, and in one a growth of bacteria was obtained. As stated in the exclusion criteria, no patients with polymicrobial infection were included in the trial. There are equal numbers of Aspergillus andFusarium in this series in Bangladesh.Aspergillus fumigatus andAspergillus sp present the biggest problems for treatment. Whereas eight of 20 infections withFusarium followed to 21 days were healed on the initial treatments, only one out of 18Aspergillus responded to either choice of primary treatments (in this case chlorhexidine). However, five moreAspergillus ulcers healed on alternative treatment. Four Aspergillus cases were among the six people who dropped out or were in the last few cases not followed up for 21 days (Fig 1).
Results of cultures of 63 isolates and their sensitivities in vitro to the two primary treatments and to econazole
In the group receiving primary treatment with chlorhexidine and followed up to 21 days, there were seven cases from whichAspergillus was cultured. One (study no 61) healed at 10 days with chlorhexidine, the fungus in this case showing some sensitivity to chlorhexidine, natamycin, and econazole (Table 4). A second case of Aspergillus (study no 17) healed on alternative treatment with natamycin 5% and clotrimazole. Of the other five, one (study no 21) perforated at 21 days and four ended up at 21 days with adherent leucomata. The fungi from two of these (study nos 12, 27) 3were resistant to both chlorhexidine and natamycin 2.5%, one (study no 16) resistant to chlorhexidine alone, and the fourth (study no 20) sensitive to all three drugs.
Eleven cases growing Aspergillus and treated initially with natamycin 2.5% were followed for 21 days. None showed a favourable clinical response at 5 days, so all were switched at that time to alternative treatment. Four healed on alternative therapy of natamycin 5% plus clotrimazole (three) or econazole plus clotrimazole (one). Seven others showed no response to various combinations of natamycin 5%, clotrimazole, and econazole, even though the fungi from four has showed sensitivity to natamycin 2.5% (study nos 06, 15, 47, and 65).
All except one of the cultures ofAspergillus were sensitive to econazole 1% by the well diffusion method (Table 4). Fourteen of 21 cultures showed sensitivity to natamycin 2.5%. There was a smaller response to chlorhexidine, but 15 of 21 cultures were inhibited to at least a small degree by chlorhexidine. On the other hand, all of the other fungi isolated in culture except one (study no 58) were sensitive in vitro to chlorhexidine. The clinical response does not necessarily correlate with the in vitro sensitivities.
Corneal ulcer occurred particularly in the 21–50 age group, which accounted for 65% of total patients. About 35% of the affected people were farmers, others were outdoor working groups—that is, those who are prone to trauma. Trauma was the main predisposing factor for fungal keratitis, accounting for about 56%. Some patients had used steroids or antibiotics before coming, in the same eye, and some of them had used native medicines, even snail juice. About 43% of patients attended the cornea clinic within the first 10 days of illness. Visual acuities were recorded before corneal scraping and 32% of affected eyes presented with hand movements.
TOXICITY
Both drugs were well tolerated by the patients and none complained of burning or itching following the instillation of the drops. In no case was the drug discontinued because of allergy or of toxic effects. The only clinical sign of toxicity noticed during the 3 weeks of treatment was a temporary (short lived) punctate epithelial keratopathy in one patient receiving chlorhexidine. There was evidence that the drops were being applied in hospital more frequently than 3 hourly in this patient. The epithelial keratopathy disappeared when the 3 hourly regimen was rigidly enforced. There was no early cataract in any treatment group even 6 months to 1 year after treatment.
LONG TERM FOLLOW UP
Of the 65 patients still in the study at 21 days plus the four who had not yet reached 21 days, 59 were visited in their homes at between 6 months and 1 year. This included all four who had not reached 21 days at the end of the trial. Transport was arranged for them to come to the hospital for slit lamp examination. Three severe ulcers which had shown a favourable response at 5 days had healed when the original chlorhexidine treatment had been maintained for 26, 37, and 60 days. There was no evidence of late toxicity.
Discussion
These results suggest that, assessed first at 5 and then at 21 days of treatment and in the long term, chlorhexidine may be superior to natamycin in efficacy against keratitis due to a range of filamentary fungi. Chlorhexidine is well known to be effective against a range of Gram positive and Gram negative bacteria, is being used for the treatment of Acanthamoebakeratitis,1011 and was also thought from one study to be effective against Chlamydia trachomatis.12 Chlorhexidine digluconate is already used as a preservative in eye preparations and is therefore approved for use in low concentrations in the human eye. It has been used in several other clinical situations for about 40 years. These include sterilisation of the skin, prevention of sepsis in wounds and burns, prevention of urinary tract infections, especially in catheterised patients, and antisepsis in practical obstetrics, including vaginal washing with 0.2% chlorhexidine solution. Chlorhexidine is regarded as the most effective antimicrobial mouth wash. The standard preparation is a 0.2% solution, and it has been available for more than 20 years in some countries. The extensive literature on its antimicrobial properties, applications, and safety has been reviewed by Denton.13
In this study chlorhexidine gluconate 0.2% drops have been used regularly in these eyes for 3 weeks, apparently without toxicity. When chlorhexidine was first applied to the sterilisation of soft contact lenses, a number of studies of possible toxicity to animal eyes were carried out. For example, Gasset and Ishii found no detectable changes from applications of concentrations up to 2% to rabbit eyes twice daily for 7 days.14 Aqueous chlorhexidine solutions were evaluated for retardation of epithelial regeneration after experimental corneal abrasions.15 While irrigation with concentrations of 2% or 4% significantly slowed the healing rate, concentrations of 1% or less did not statistically slow healing. The toxicity of chlorhexidine for animal and human tissues has recently been reviewed.11 It is important to stress that some preparations of chlorhexidine, such as surgical scrubs, contain detergents. These must not be used in the eye.
The results suggest that if fungi are seen on Gram staining or in a potassium hydroxide mount, chlorhexidine might be a useful first line agent. At the same time cultures could be set up for sensitivity testing. It is appreciated that this well diffusion method is not standardised, but it may be of use in developing countries by the very nature of its simplicity, to give a general indication of the likely susceptibility of fungal isolates from ulcers. If no improvement is achieved or sensitivity testing indicates likely resistance, a change could be made to other antifungal agents. It is clear that further work is required on inexpensive agents which would be effective againstAspergillus.
In considering chlorhexidine digluconate as a treatment for fungal keratitis in developing countries, where mixed infections may be common and laboratory facilities are not usually available, an advantage may also be its wide antimicrobial action against bacteria, fungi, andAcanthamoeba in situations where specific antibiotics or antifungal agents cannot be obtained and as a prophylactic against infection after superficial trauma to the cornea. The results described suggest that chlorhexidine may warrant further assessment for use as a first line antimicrobial for corneal ulcers when other agents are not available.
Acknowledgments
This study was supported by a grant from the British Council for the Prevention of Blindness. We thank Dr Gill Midgley for assistance with identification of the fungi.