Article Text

Abstract
Aim: To evaluate the reliability of lens density measurement with anterior segment optical coherence tomography (OCT) and its association with the Lens Opacity Classification System Version III (LOCS III) grading.
Methods: Fifty-five eyes from 55 age-related cataract patients were included. One eye from each subject was selected at random for lens evaluation. After dilation, lens photographs were taken with a slit lamp and graded against the LOCS III standardised condition. Anterior segment OCT imaging was performed on the same eyes with a high-resolution scan. The association between the anterior segment OCT nucleus density measurement and LOCS III nuclear opalescence (NO) and nuclear colour (NC) scores was evaluated with the Spearman correlation coefficient. Anterior segment OCT measurement precision, coefficient of variation (CVw), and intraclass correlation coefficient (ICC) were calculated.
Results: The mean NO and NC scores were 3.39 (SD 1.10) and 3.37 (SD 1.27), respectively. Significant correlations were found between anterior segment OCT nuclear density measurements and the LOCS III NO and NC scores (r = 0.77 and 0.60, respectively, both with p<0.001). The precision, CVw and ICC of anterior segment OCT measurement were 2.05 units, 4.55% and 0.98, respectively.
Conclusion: Anterior segment OCT nucleus density measurement is reliable and correlates with the LOCS III NO and NC scores.
Statistics from Altmetric.com
Grading of lens opacity is for epidemiological study of cataract prevalence, as well as assessment of their severity and progression. An ideal lens grading system should be objective and reproducible. The Lens Opacification Classification System III (LOCS III), a widely used lens grading system,1 is based on the evaluation of three sets of photographs on an 8.5 inch×11 inch colour transparency taken under the slit lamp, and compared with the standard colour photographic transparencies of cortical cataract (C), nuclear opalescence (NO), nuclear colour (NC) and posterior subcapsular cataract (P). Although the LOCS III has become the standard in evaluating cataract morphology and density, it may be limited by being a largely subjective classification system. The standard colour photographic transparencies only provide an integer value on the scale, and the grader needs to assign decimal values between these photographic standards.
The anterior segment optical coherence tomography (OCT) (Visante OCT, Carl Zeiss Meditec, Dublin, California) is an imaging technology commercially available for direct visualisation of the anterior segment. The design is based on low-coherence interferometry using a superluminescent diode with a wavelength of 1310 nm. The scan speed is up to 2000 axial scans per second with axial resolution of about 18 μm. While anterior segment OCT has been found to be reproducible in evaluating the corneal thickness,2–4 anterior chamber angle 5–7 and anterior segment biometry,8 9 to our knowledge, its application to assess lens morphology and density has not been investigated. The purpose of this study is to evaluate the reliability of lens density measurement with anterior segment OCT and its association with the LOCS III.
METHODS
Subjects
Fifty-five eyes from 55 age-related cataract patients with different degrees and types of lens opacities were enrolled. All of them were Hong Kong Chinese and had no previous ocular surgery or laser treatments and history of any ocular diseases other than age-related cataract. The study was conducted in accordance with the Declaration of Helsinki (1996) and the ICH GCP (E6) Guideline, and approved by the Clinical Research Ethics Committee (Kowloon Central/East) with informed consent obtained from all participants.
Lens opacities grading
Pupils were maximally dilated with phenylephrine 2.5% and tropicamide 1% eye-drops to a diameter more than 6 mm on the day of examination. The crystalline lens opacities were graded against the LOCS III standards by one trained grader with the Haag-Streit slit-lamp microscope. After dilation of a participant’s pupils, the grader assigned a numeric grade to the degree of nuclear opalescence (0.1 to 6.9), nuclear colour (0.1 to 6.9), cortical opacity (0.1 to 5.9), and posterior subcapsular opacity (0.1 to 5.9) under standardised conditions. In this study, only the NO and NC scores were used to determine the association with the anterior segment OCT measurements.
Anterior segment optical coherence tomography imaging
The anterior segment optical coherence tomography (ASOCT) (Visante OCT Model 1000, Carl Zeiss Meditec, Dublin, California) is a non-invasive, high-resolution tomograhic and biomicroscopic device designed for anterior segment imaging and measurement. The Visante anterior segment OCT received FDA approval for imaging the anterior segment in 2005. The power reaching the cornea is less than 6.5 mW at the cornea. To our knowledge, there has been no report so far in the medical literature suggesting that reflectivity at an infrared wavelength of 1310 nm would affect vision in the visible wavelengths. Analogous to an ultrasound B-scan, ASOCT acquires multiple A-scans and aligns them to construct two-dimensional images. Each selected eye was imaged with ASOCT with a “high-resolution corneal” scan type (scan length 10 mm; scan depth 3 mm) with the subject fixated on an internal fixation target. The pupil was dilated to at least 6 mm, and the scan line was adjusted to a horizontal position bisecting the pupil. The real-time charge-couple device displaying the position of the scan and the eye was available to allow a more precise alignment. The high-resolution scan type was selected for imaging because it provides higher-quality images compared with the low-resolution scanning protocols. However, as the thickness of a normal adult human lens is often more than 3 mm, anterior and posterior halves of the lens were captured separately in two consecutive scans. The polarisation of the scan, saturation and noise of the images were standardised at 45, 50 and 5, respectively. The eyes were all imaged under room light (light intensity = 368 lux).
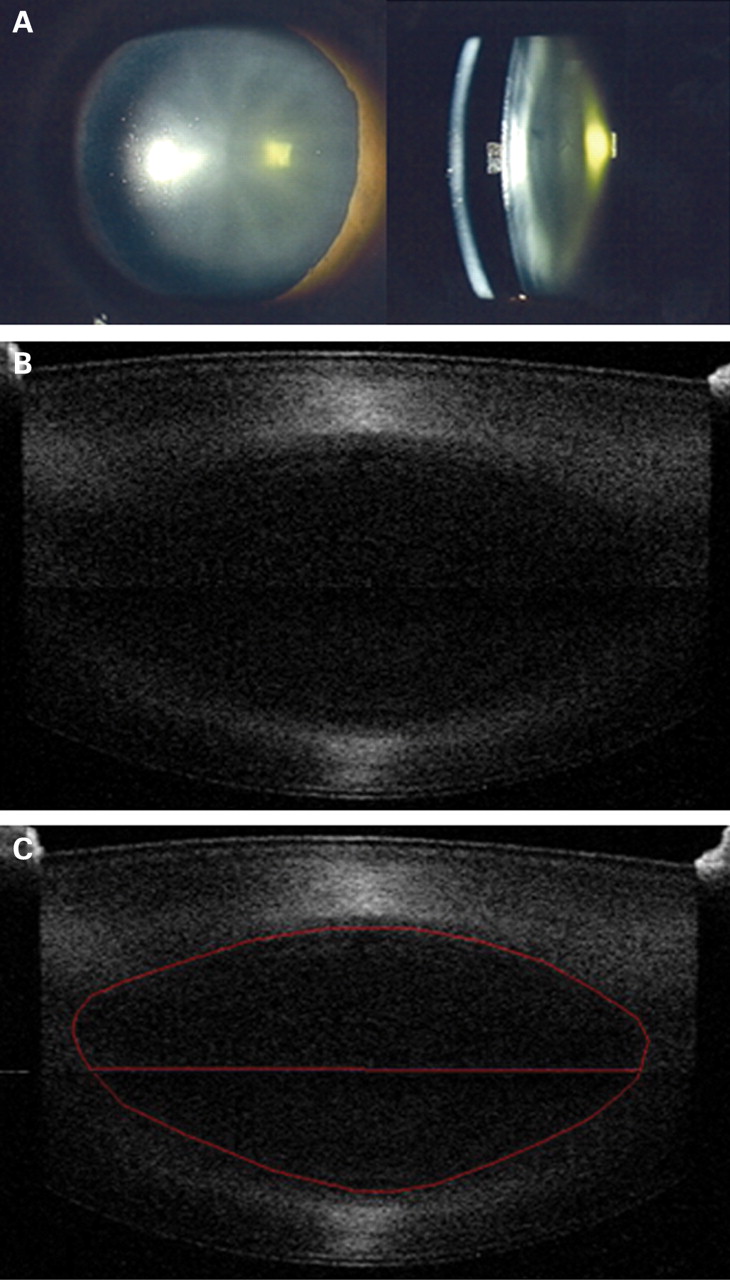
The built-in software of the Visante ASOCT automatically corrects optical and instrument distortions of the image to reduce the measurement error of corneal thickness and anterior chamber depth. This process is known as dewarping. However, the algorithm was unable to dewarp image of the lens and produced artefacts. Therefore, in this study, the uncorrected images were exported for analysis. The area selected for lens density measurement only encompassed the nucleus. The pixel intensity was measured using image-analysis software (Sigma Scan Pro version 5, Systat software, Point Richmond, California). To compensate for the background noise in the OCT images, the mean pixel intensity of the anterior chamber was also measured in each eye. The adjusted pixel intensity of each half of the lens nucleus was calculated as the mean pixel intensity of the lens minus the mean pixel intensity in the anterior chamber. Finally, the average adjusted pixel intensity of the entire nucleus (nuclear cataract density) was derived from averaging the density measurements from each half of the lens (see figs 1, 2).


Evaluation of repeatability
Three pairs (anterior and posterior halves of the lens) of images were captured consecutively for each patient by a single operator. After obtaining a pair of images, the subject was asked to sit back while the images were stored in a computer. The same procedure was repeated until three pairs of images were collected.
Statistical analysis
Statistical analyses were performed using SPSS version 13.0 (SPSS, Chicago). The association between the LOC III NO and NC scores and ASOCT nuclear density measurements was evaluated using the Spearman correlation coefficient. A multivariate regression model was examined with ASOCT nuclear density as a dependent variable, the LOCS III NO and NC scores as independent variables. The repeatability was measured with three sets of consecutive images. The within-subject standard deviation (Sw), precision (1.96×Sw), coefficient of variation CVw (100×Sw/overall mean) and intraclass correlation coefficient (ICC) were calculated. The Sw was calculated as the square root of the within-subject mean square of error (the unbiased estimator of the component of variance due to random error) in a one-way random-effects model.10 The ICC is the ratio of the intersubject component of variance to the total variance (intersubject variance+within-subject variance). The association between the SD and the mean of the repeated lens density measurements was evaluated using a correlation analysis (Kendall tau correlation coefficient).
RESULTS
A total of 55 patients were included. The mean age was 69.87 (SD 10.13) years. There were 25 males and 30 females. Only one eye in each subject was selected randomly for analysis.
The distribution of the LOCS III scores for 55 eyes is shown in table 1. The mean NO and NC scores were 3.39 (SD 1.10) and 3.37 (SD 1.27), respectively. For anterior segment OCT nucleus density measurement, the average pixel intensity ranged from 12.93 to 40.61 units with a mean of 23 (6.77) units. Figures 1, 2 illustrate two examples of nucleus density measurement. The distribution of ASOCT nuclear density measurement against the LOCS III NO and NC scores is shown in fig 3. There were significant correlations between ASOCT measurements and the LOCS III NO and NC scores (r = 0.77 and 0.60, respectively, both with p<0.001). Multivariate regression analysis revealed that the LOCIII NO score was the only significant factor associated with ASOCT nuclear density in the model (R2 = 0.71, p<0.001). There was no significant correlation between visual acuity (logMAR) and anterior segment OCT lens density measurement or the LOCS III NO/NC scores (p⩾0.126). There was no association between the SD and the mean of the nuclear density measurements (p = 0.602).

Table 2 presents the within-subject SD (Sw), coefficient of variation (CVw), precision and intraclass correlation coefficient (ICC) of ASOCT nucleus density measurements. High repeatability was observed with a CVw of 4.55% (95% CI 3.95% to 5.15%), and the ICC was 0.98 (95% CI 0.96 to 0.99).
DISCUSSION
In this study, significant correlations were found between the ASOCT nuclear cataract density measurement and the LOCS III NO and NC scores. The slightly higher association with the NO score suggests that ASOCT provides a better surrogate on lens density than lens colour. High repeatability was also demonstrated by the low value of coefficient of variation and high value of the intraclass correlation coefficient. These findings indicate that ASOCT could provide a reliable measurement of lens density.
ASOCT provides objective assessment and quantification of lens density. ASOCT imaging is simple to perform and rapid, and has a low learning curve. This is in contrast to slit-lamp-based photographic grading systems in which slit-lamp settings may influence the grading scores, and more practice and training are required to achieve optimum consistency in lens grading.11 The ordinal scale in the LOCS III grading systems may also be inadequate for detecting small changes in longitudinal studies. In our series, the measured nucleus density ranged from 12.93 to 40.61 units (corresponding to NO scores from 2.0 to 6.0) with a precision of 2.05 units. With a more dynamic range and high measurement repeatability, it is conceivable that ASOCT may serve as a sensitive tool to detect longitudinal change in lens density.
Scheimpflug photography is another imaging modality that has been developed for objective in vivo assessment of lenticular density.12 It measures the light-scattering intensity and densitometrically evaluates the lens opacity from the slit images. Although Scheimpflug photography allows quantitative documentation of the lens, measurement of light scattering intensity at the posterior cortex and posterior capsule could be difficult even if the subject’s pupil was completely dilated.13 Using a superluminescent diode with a wavelength of 1310 nm, ASOCT provides a clear visualisation of the posterior cortex and capsule of the lens. The lens opacity meter is another instrument for cataract density measurement measuring the amount of stray light produced by the lens in response to a modulated beam of incident red light.14 However, inconsistent results were found at pupil diameters of less than 4 mm, and this is probably related to absorption of scattered light by the iris.15
Although we only evaluated the lens nucleus in this study, density measurement is possible also in the anterior and posterior cortex. A more comprehensive assessment of cataract morphology and density could be acquired with multiple scans at different meridians. Because of the scan geometry of the scan probe and the refraction at smooth surfaces of the eye, an algorithm for dewarping was incorporated in the analysis software to correct for image misalignment in the anterior chamber. However, this algorithm was unable to dewarp image of the lens and produced artefacts in Visante ASOCT (fig 4). It has been shown by Dunne et al that lens curvature and dimensions can be measured using paraxial ray tracing formulas.16 As the primary objective was to measure the lens density, the uncorrected images were acceptable for analysis in this study. Dunne et al also reported that ASOCT overestimates corneal thickness by 60 μm.16 However, most in vivo studies, in fact, suggest that ASOCT underestimates central corneal thickness compared with the reference standard—ultrasound pachymetry.2–4 In this regard, ASOCT may appear less “accurate” compared with ultrasound pachymetry. Nevertheless, there is substantial evidence in the literature reporting that ASOCT measurements (central corneal thickness/anterior chamber depth, anterior chamber angles) are reproducible (ie, measurements obtained between visits or within visits are consistent).2–4 19 In other words, ASOCT is a reliable instrument.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
There was no significant correlation between visual acuity (logMAR) and anterior segment OCT lens density measurement or the LOCS III NO/NC scores. This result is not surprising, since lens density could be more related to high spatial frequency contrast and sensitivity. Visual acuity may not be correlated with the LOCS NO/NC grading.17 18 Finally, ASOCT is also limited to receiving any signal behind the iris. Dilation is required to maximise lens exposure.
In summary, ASOCT is clinically useful for evaluation and measurement of lens opacity. It provides an objective measure of lens opacity, and the learning curve for lens imaging with anterior segment OCT is much shorter compared with the LOCS III grading. OCT imaging may serve as a new paradigm to evaluate cataract density in clinical practice and in epidemiology studies.
REFERENCES
Footnotes
Competing interests: CL and RW have received research support in the form of instruments from Carl Zeiss Meditec. RW is a consultant to Carl Zeiss Meditec.
Ethics approval: Ethics approval was provided by the Clinical Research Ethics Committee (Kowloon Central/East).
Patient consent: Obtained.
Linked Articles
- At a glance