Article Text

Abstract
Objective To estimate the incidence and describe the demographic characteristics of keratoconus (KC) in Colombia using national health registry data between January 1st 2015 and December 31th 2020.
Methods and analysis We conducted a nationwide, population-based study using the Integrated Social Protection Information System from the Colombian Ministry of Health, the unique official database in the country. We used the International Classification of Diseases code for KC (H186) to identify the number of new cases of KC and estimate the incidence rates both overall and according to age and sex. We made a standard morbidity ratio map to graph Colombia’s morbidity risk of KC onset.
Results Of 50 372 424 subjects, 21 710 had KC between 2015 and 2020. However, due to the COVID-19 pandemic, all the incidence rates of this study were based on the 18 419 reported until 2019. The incidence rate in the general population was 10.36 (95% CI 10.08 to 10.64) per 100 000 inhabitants. The incidence peak among males was in their early 20s and females in their late 20s. The overall male to female incidence rate ratio was 1.60. Regarding the distribution of the disease, most cases were reported in Bogotá (48.64%), Antioquia (14.04%) and Cundinamarca (10.38%).
Conclusion We performed the first nationwide, population-based study of KC in Latin America, finding distribution patterns similar to those reported in the literature. This study provides valuable information on the epidemiology of KC in Colombia, which is helpful in the development of policies for the diagnosis, prevention and treatment of the disease.
- epidemiology
- public health
- cornea
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The incidence of keratoconus has been described in other population-based studies, ranging from 1.3 to 32.3 per 100 000 inhabitants.
Data for South America are scarce and limited to cohorts that do not reflect nationwide epidemiology data.
WHAT THIS STUDY ADDS
This study describes the incidence of keratoconus in a developing country in South America based on a nationwide database for the first time, finding an incidence of keratoconus in Colombia of 10.36 (95% CI 10.08 to 10.64) per 100 000 inhabitants, with a high number of new cases among those in their 20s.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study describes and adds new information about the epidemiology of keratoconus in Latin American developing countries.
We provide valuable data for the development of policies for diagnosis, prevention and treatment of the disease.
Introduction
Keratoconus (KC) is a progressive ectatic corneal disease that leads to corneal protrusion and thinning, resulting in irregular astigmatism and visual impairment. Generally, it has been considered a bilateral but asymmetrical condition.1–3 Clinically, it can be asymptomatic in subclinical stages until blindness in cases of scarring or hydrops.1 3 Glasses and contact lenses can restore visual acuity in most patients with KC.1 3 However, severe cases require surgical procedures such as cross-linking, intracorneal ring segments and corneal transplantation. Of all patients with KC, 10%–20% will undergo at least one penetrating keratoplasty.4–6
Although the aetiology of KC is not entirely understood, several risk factors have been associated with its development. Age, ethnicity, consanguinity, atopy and mechanical trauma are some of the main risk factors described.7 However, environmental factors such as ultraviolet exposure,8–10 pollution11 12 and smoking13 14 have also been reported.
The number of KC cases has been increasing in the last decades. This could be explained by the improved understanding of the disease and new imaging modalities that can diagnose KC more frequently and at earlier stages than in the past.15 The reported annual incidence ranges from 1.3 to 32.3 per 100 000 inhabitants.16 17 Vast differences between studies may be attributed to study population, ethnicity, diagnostic criteria and diagnostic devices used.7
KC is more common in the Asian continent.18 Thus, most studies related to the epidemiology and burden of the disease are focused on these populations, while few studies described the incidence and prevalence of KC in Latin America.19 20 In Colombia, Barraquer-Coll et al21 described a prevalence of KC and pellucid marginal degeneration of 2.84% in a single-centre, cross-sectional study including 91 426 patients. The Colombian Ocular Diseases Epidemiology Study (CODES) is a series of reports focusing on the description of epidemiology data for ocular diseases in Colombia. Herein, we report the incidence of KC using the national health registry data over a period of 6 years.
Methods
Design
We conducted an observational, descriptive, claim database, cross-sectional study using the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Population
The information and data in this study were obtained from the national database created by the Colombian Ministry of Health, known as the System of Information of Social Protection (SISPRO), which stores, processes and systematises Colombian citizens’ health registers (data set).22 The data are collected by medical staff during each medical contact (inpatient or outpatient) from private and public health providers and insurers using the International Classification of Diseases (ICD-10). In addition, the demographic and clinical data are grouped in the RIPS (Individual Registry of Health Services Provision).23
It should be noted that the Colombian health system has one of the most prominent coverages in Latin America, encompassing 50 million inhabitants, representing 97.78% of the population in 2020, according to the last survey of the National Administrative Department of Statistics (DANE) (data set).24
Data collection
Data were extracted from the SISPRO dynamic tables from 2015 to 2020 (data set). The ICD-10 code for KC (H186) was used. To delimit the results, we performed the first filter by year (2015–2020) and the type of diagnosis (confirmed new) to determine the incidence. Afterwards, additional filters, such as residence location, age and sex, were added to describe the sociodemographic status of the disease. Finally, a database in Microsoft Excel (Microsoft, Redmond, Washington, USA) was elaborated and validated to record the information.
Statistical analysis
The crude incidence rate of KC in the Colombian population was estimated for 6 years (2015–2020) using a standardised crude rate per 100 000 inhabitants of confirmed new KC cases divided by the consultation population of the Colombian medical service (considering these as the risk population). For the incidence analysis, the patients were divided and stratified by sex and age in quinquennium. Twenty-four patients were excluded from the analysis by sex because they did not have this information reported. Still, they were included in the analysis of the total patients by age. Considering that the data are secondary and may not represent the parameter of the total number of cases, 95% CI for the rates was calculated assuming a Poisson error. These analyses were performed with R V.4.0.4.
Additionally, since the pandemic significantly affected the results in 2020, we used a statistical model for spatial data based on the Gaussian Markov random fields (GMRF) to predict what would have happened this year regarding the incidence of the disease. We used the conditional autoregressive model, a type of GMRF. This model approach visualises the geographical domain as an undirected graph with a vertex in each region and an edge between two vertices if the corresponding regions share a geographical edge. This creates well-defined neighbours for each region, which are used to define the joint or conditional distribution. As a result, the distribution will be the multivariate normal distribution. More detailed information regarding the statistical analysis is found in online supplemental material 1.
Supplemental material
Bias control
In this study, selection bias may occur due to several filters applied to the diagnostic data in SISPRO (data set). Also, due to the scarcity of cornea supraspecialists in the country, underestimation and misclassification bias with other ICD codes like H187 (other corneal deformities) may occur.25 However, we only included patients with a ‘confirmed new diagnosis’ to prevent these biases. Additionally, the H186 ICD-10 code is not commonly used by general physicians but by ophthalmologists. Further, since we do not have access to clinical charts, we cannot assert that there are no repeated patients because it is secondary information. After applying filters, the total data accuracy cannot be guaranteed because the database does not allow us to rectify the identification numbers. However, the Colombian Ministry of Health and healthcare provider institutions constantly update and correct data with errors to control this bias. Previous studies based on SISPRO (data set) have determined the concordance rate of the database using ICD-10 with medical records to be up to 83.4%.26 27 Therefore, these data are the most accurate approximation.
Results
The SISPRO database from 2015 to 2020 recorded 27 017 352–34 370 304 consultations (data set). From 2015 to 2020, there were 21 710 new cases of KC throughout the country. However, considering the high probability of under-reporting due to the COVID-19 pandemic in 2020, we analysed the 18 419 cases reported until 2019, including 9685 (52.58%) males and 8734 (47.42%) females.
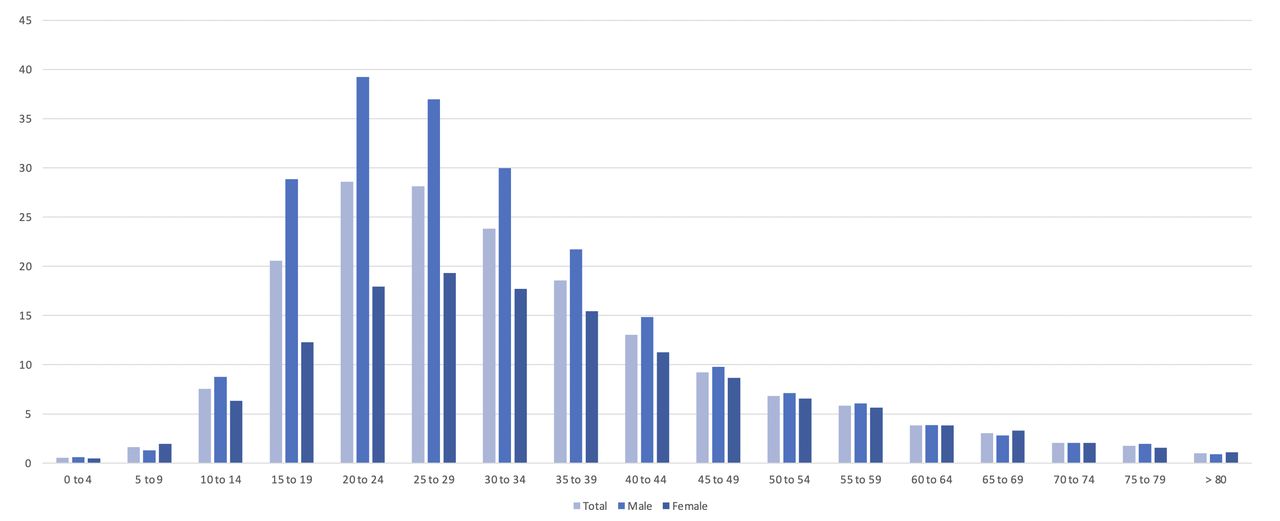
There were 2600 (14.11%), 2604 (14.13%), 3293 (17.87%), 4165 (22.61%) and 5757 (31.25%) incident cases in 2015, 2016, 2017, 2018 and 2019, respectively. The incidence rate of KC in the general population was 10.36 (95% CI 10.08 to 10.64) cases per 100 000 inhabitants. In males, it was 12.76 (95% CI 12.37 to 13.14) cases per 100 000 inhabitants; in females, it was 7.96 (95% CI 7.60 to 8.32) cases per 100 000 inhabitants. The peak incidence was at 20–24 years of age in males (39.24; 95% CI 39.12 to 39.35) and at 25–29 years of age in females (19.32; 95% CI 19.19 to 19.44). Males had a higher incidence rate in all ages except for ages 5–9, 65–69 and >80 years; the overall male to female ratio with regard to incidence was 1.60 (range: 0.66–2.35 in the different age groups). Detailed incidence results are presented in table 1 and figure 1.
Number of patients with newly diagnosed keratoconus and the estimated incidence rate (per 100 000 inhabitants) of keratoconus in Colombia in 2015–2019
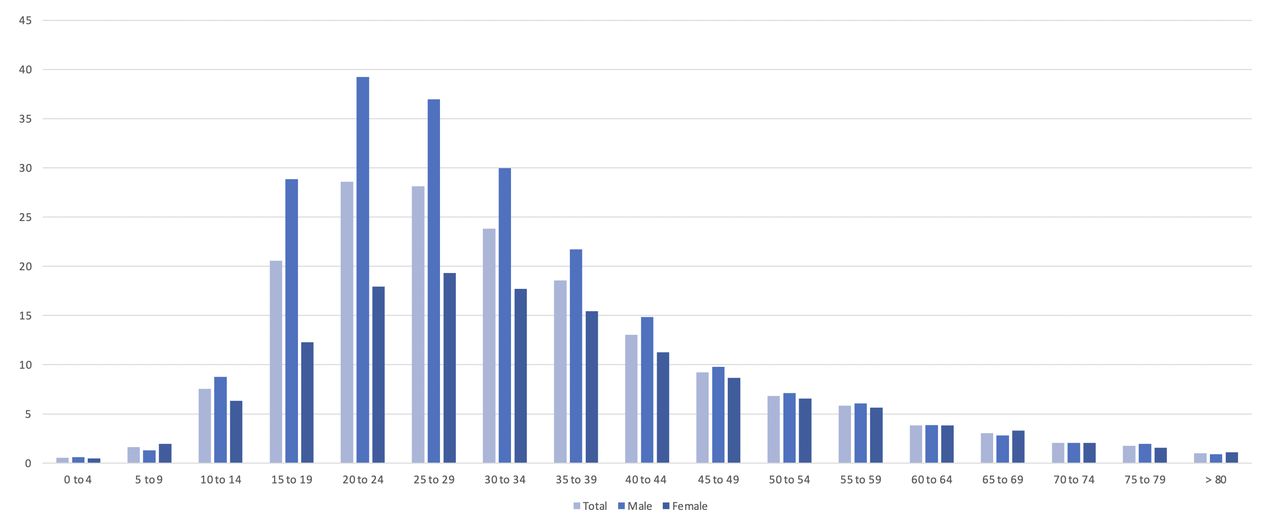
Incidence rates of keratoconus both overall and according to age and sex. Incidence=(number of confirmed new cases by quinquennial age per year/SISPRO consultation registers by quinquennial age per year)×100 000 inhabitants (data set).22 SISPRO, System of Information of Social Protection.
The incidence of KC increased from 9.62 (95% CI 9.52 to 9.71) in 2015 to 14.02 (95% CI 13.95 to 14.08) in 2019. For 2020, we presented the real reported value of 8.65 (95% CI 8.56 to 9.73) and an estimated value based on the trend from the previous years (15.74; 95% CI 14.64 to 22.02), considering the impact of the COVID-19 pandemic on health assistance. The incidence per year can be found in figure 2.

Annual distribution of keratoconus by quinquennial age in Colombia between 2015 and 2020. The blue line represents the incidence of keratoconus obtained by SISPRO data (data set). For 2020, the red line represents the estimated incidence based on SISPRO data analysis of the previous years, showing a difference of 7.09 per 100 000 inhabitants between the real and estimated incidence.22 SISPRO, System of Information of Social Protection.
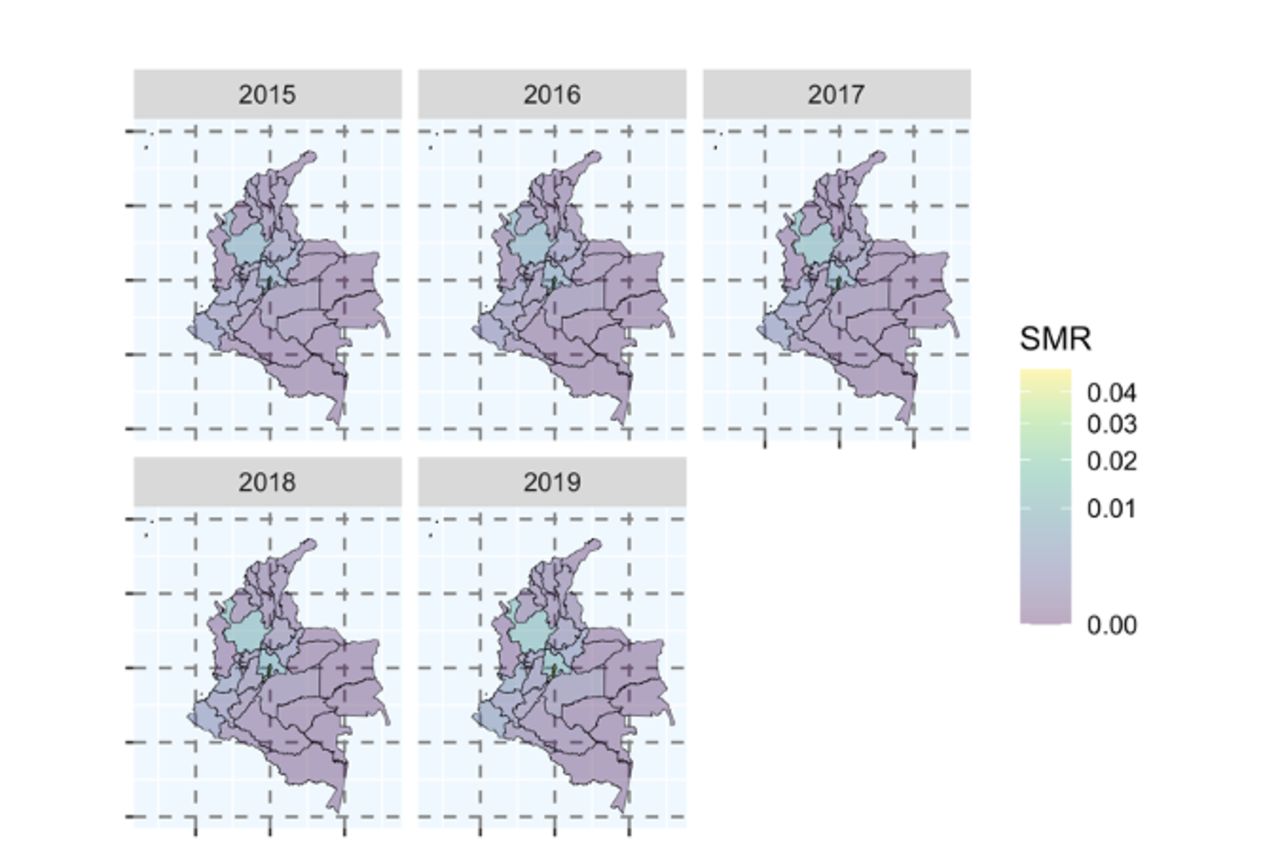
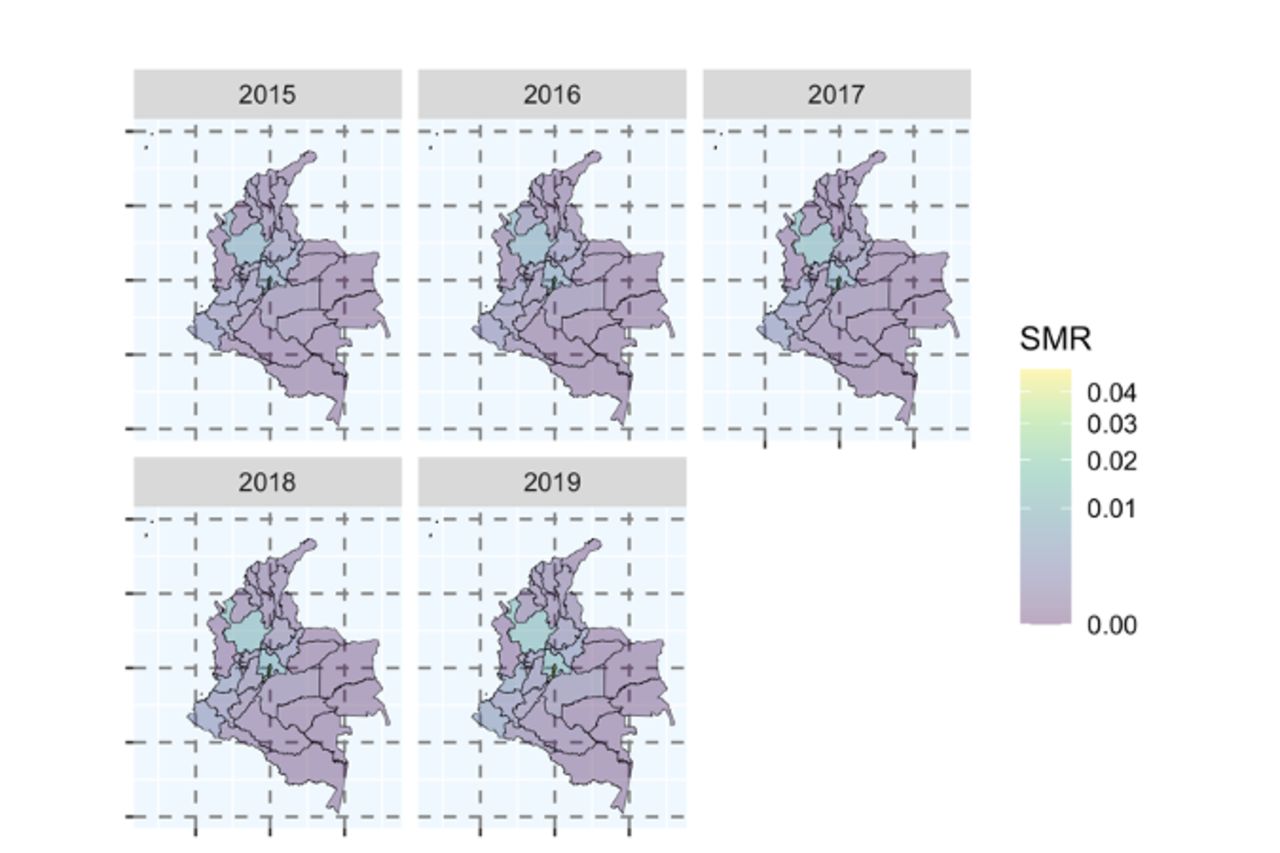
Finally, regarding the distribution of the disease, most cases were reported in Bogotá (48.64%), Antioquia (14.04%) and Cundinamarca (10.38%). More detailed information is available in online supplemental material 2. It is important to note that in 9.61% of the patients, the region of origin was not reported. Figure 3 graphs the standard morbidity ratio maps to identify the morbidity of KC in each department per year; for this analysis, the 1771 cases with no department registered were excluded from the 18 419 cases of KC reported in 2019, for a total of 16 648 cases.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Standard morbidity ratio (SMR) maps of keratoconus in Colombia. The SMR of keratoconus was higher in the Andean region. Several factors could influence this higher risk; for example, the main cities are in these areas, and capital cities have an increased migration index from rural areas and more hospital access than other regions.
Discussion
KC is an eye disease that, with proper treatment, can have excellent visual results; on the contrary, delays in its diagnosis and treatment can lead to blindness and requirement for surgical procedures.4–6 Attention to KC has been increasing recently, and there has been a revolution in the knowledge required to diagnose KC. In the past, KC was diagnosed with slit lamp findings, refraction and keratometry.28 29 However, corneal topography is now seen as the gold standard in the diagnosis and monitoring of ectatic disorders such as KC.30 Studies focused on the epidemiology and incidence of KC offer valuable information for developing preventive and therapeutic strategies. We performed the first population-based study that describes the age-specific incidence of KC in Latin America.
Previously reported incidence rates of KC have varied widely depending on the study population, diagnostic criteria and geographical location. The incidence of KC in other population-based studies ranges from 1.3 to 32.3 per 100 000 inhabitants16 17; we report an incidence rate of KC in the general population of 10.36. This is lower than the incidence reported by Ziaei et al31 of 22.3 per 100 000 inhabitants in a prospective, population-based survey during 2008–2009 in Iran, but higher than the incidence reported in Denmark and England of 3.6 and 3.5 per 100 000 person-years, respectively.17 32 Thus, ethnicity and geographical location influence the incidence of KC directly. A summary of previous population-based studies of KC is presented in table 2.
Previous population-based studies reporting the incidence rate of keratoconus
Previous studies have shown that in the Asian population, KC is more prevalent, has an earlier onset and has a severe disease progression.17 33 The global consensus of KC and ectatic diseases,34 consisting of cornea subspecialists worldwide, affirms that Asians and Arabians have a higher risk of ectasia. However, the information supporting this is not entirely conclusive, as nationwide studies also support a reduced risk of KC in the Asian population compared with Caucasians.35 The difference may be explained by KC being more prevalent in some specific Asian populations, including Indians, Pakistanis and Saudi Arabians,17 33 but not in East Asian people.36 37
Ethnographic characterisation of a South American country is complex due to its rich demographic history. Homburger et al,38 with ancestry-specific principal component analysis, determined that the Colombian population derives primarily from European descendants. DANE (data set) reported a prevalence of 87.58% of white race, followed by 9.34% Afro-American and 4.4% Amerindian.39 The low influence of Asian race supports a lower risk of KC in Latinos (Hispanic heritage) than the Asian population.17 33
KC can affect both genders and sex predilection is not apparent. Some studies report male predominance,33 40 while others report female predominance41 or no predilection.28 36 In our study, males represent 65.8% of all cases, with higher incidence rates in almost all age groups, excluding 5–9, 65–69 and >80 years. Therefore, we conclude that KC in Colombia has a male predilection.
Interestingly, KC appears earlier in males (20–24 years) than in females (25–29 years). This finding has also been reported in other studies40 42; the question of whether males are at greater risk of aggressive disease requiring corneal transplantation has been raised. In a longitudinal, prospective, 9-year follow-up study, Edwards et al43 found that males presented for corneal grafting earlier than females, but the overall percentage figures for surgery are similar for both males and females. Therefore, these results do not support the idea that males have a more aggressive disease than females, only that the disease is present more often and earlier in males than in females. Gender differences in the incidence of KC may be attributable to hormonal and biological changes.44 45 However, more studies are needed to clarify these differences.
Regarding the age distribution of KC, the diagnosis incidence rate is higher in young people. Similarly, Godefrooij et al46 considered patients between 10 and 40 years as the relevant age category for newly diagnosed KC. The peak incidence rate of KC in the general population was at 20–24 years, 28.59 (95% CI 28.50 to 28.67) cases per 100 000 inhabitants. Although corneal weakness in young ages has been the primary hypothesis of KC pathogenetic factors,47 Kotecha et al48 reported a negative correlation between corneal viscoelastic properties and advancing age due to an increase in cross-linkage of collagen fibrils within the cornea. These may suggest that the cornea gets stiffer with age and that KC progression significantly decreases.
Another interesting finding in our study is the onset of KC at a very young age (from 0 to 9 years of age) in 404 children; this has also been reported by Hwang et al36 in a population-based study in South Korea between 2009 and 2014. KC commonly develops at or after teenage; however, paediatric KC can occur associated with systemic syndromes or diseases such as atopy, Down’s syndrome and connective tissue disorders.12 49 Unfortunately, we cannot assess if these cases were associated with some previously mentioned systemic diseases. In addition, although we do not know precisely how KC was diagnosed in these children, we used only confirmed new cases, so for them to be registered in SISPRO (data set) they must be diagnosed by an ophthalmology specialist using corneal topography, considering the years studied were when corneal topography use was widespread.
The strengths of this study include the large sample size. Ours is the first population-based study in Latin America to use a database from the national health registry and the most extensive study that focuses on the incidence and sociodemographic characterisation of KC worldwide. Previous studies based on SISPRO (data set) have determined the concordance rate of the database using ICD-10 with medical records to be up to 83.4%,26 27 which means the results reported in this study offer valuable insight into the epidemiology of KC in Colombia.
Limitations
Our study has some limitations we have thoughtfully considered and addressed. First, we may have underestimated the incidence of KC since asymptomatic patients who did not use the healthcare service cannot be included. Nevertheless, we believe that we captured the most symptomatic patients considering that the Colombian health system has one of the most prominent coverages in Latin America, encompassing 50 million inhabitants, representing 97.78% of the population in 2020.24 Underestimation and overestimation are frequent in population-based studies; nevertheless, they provide valuable information as they include a large population sample.50
Another limitation innate to nationwide, population-based study is the absence of uniform criteria for KC registration, as individual ophthalmologists register each case. Also, SISPRO (data set) does not allow us to see patients’ identification number and thus we cannot ensure that there are no repeated patients and that duplicates are not found in cases. Nevertheless, we only include confirmed new cases to establish the incidence, avoiding most duplicates. Furthermore, we presume that an ophthalmologist confirmed each case using the gold standard criteria for the time (corneal topography), considering the years included.
Conclusion
This population-based study of the entire Colombian population highlights the age-specific and sex-specific incidence of KC. We found similar demographic patterns to the previous literature reports; we found an incidence of 10.36 (95% CI 10.08 to 10.64) cases per 100 000 inhabitants, an expected incidence for a Latin American population (Hispanic heritage) compared with Asian populations which report higher incidences. The incidence peaks of KC were in the early 20s in males and in the late 20s in females. The overall male to female ratio with regard to incidence was 1.60. Finally, we report the impact of the COVID-19 pandemic on the diagnosis of KC, which is essential to consider as delays in its diagnosis and treatment can lead to blindness and requirement for surgical procedures. This study provides valuable information on the epidemiology of KC in Colombia that is useful for developing policies for diagnosis, prevention and treatment of the disease.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study adheres to the ethical principles for human research established by the Helsinki Declaration, the Belmont Report and Colombian Resolution 008430 of 1993. According to the risks contemplated in Resolution 8430 of 1993, this investigation is considered without risks. The information in the databases used in this article is freely accessible and available for research purposes. In the same way, their coding system ensures data confidentiality.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @warc97
Contributors GM-S, CC-G, WR-C, LFP-P, LZ-P, DP: conception and design of the study, data acquisition and analysis, interpretation of data, drafting the article, revising it critically for important intellectual content, and final approval of the version to be submitted. A-d-l-T: thematic authority, conception, design of the study, data acquisition and analysis, interpretation of data, drafting the article, revising it critically for important intellectual content, and final approval of the version to be submitted. Finally, Ad-l-T accepts full responsibility for the work and the conduct of the study, has access to the data, and controls the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.